
Abstract
Abstract
Background:
Natural orifice translumenal endoscopic surgery (NOTES) has recently gained great enthusiasm, but there is concern regarding the ability to endoscopically manage complications purely via natural orifices.
Aim:
To assess the feasibility of endoscopically managing enteral perforation during NOTES using currently available endoscopic accessories.
Methods:
Twelve pigs underwent transgastric or transcolonic endoscopic exploration. Full-thickness enterotomies were intentionally created to mimic accidental small bowel lacerations during NOTES. These lacerations were then closed with endoclips. In the blinded arm of the study, small bowel repair was performed by a second blinded endoscopist. Adequate closure of the laceration was confirmed with a leak test. Primary access sites were closed with endoclips or T-anchors. At necropsy, the peritoneal cavity was inspected for abscesses, bleeding, or damage to surrounding structures. The enterotomy site was examined for adequacy of closure, adhesions, or evidence of infection.
Results:
Fifteen small bowel lacerations were performed in 12 animals. Successful closure was achieved in all 10 cases in the nonblinded arm. Survival animals had an uncomplicated postoperative course and all enterotomy sites were well healed without evidence of necrosis, adhesions, abscess, or bleeding at necropsy. Leak test was negative in all animals. In the blinded arm, both small intestinal lacerations could not be identified by the blinded endoscopist. Necropsy revealed open small bowel lacerations.
Conclusion:
Small intestinal injuries are difficult to localize with currently available flexible endoscopes and accessories. Endoscopic clips, however, may be adequate for closure of small bowel lacerations if the site of injury is known.
Introduction
Materials and Methods
Technique overview
Pigs (Sus species; 60–80 lbs) underwent either transgastric or transcolonic endoscopic exploration. The small bowel was identified by direct visualization after gaining endoscopic access into the peritoneal cavity. Intentional enteral lacerations of varying lengths were made using an electrocautery needle knife to mimic accidental small bowel perforation. Full-thickness perforation was confirmed by visualization of the mucosa and advancement of the needle knife into the small intestinal lumen. Manipulation of the bowel was performed using biopsy or grasping forceps. Enteral incisions were then closed using endoscopic clips (Resolution Clip; Boston Scientific) initially in a nonblinded fashion by the same endoscopist and subsequently by a blinded second endoscopist. The primary entry sites (gastric and colonic incisions) were closed with endoscopic clips initially and then with T-anchors (generously provided by Wilson-Cook). The study protocol was approved by the University of Florida Institutional Animal Care and Use Committee.
Endoscopes and instruments
Both single- and double-channel gastroduodenoscopes (Olympus Medical Systems Corp.) were used. Endoscopes were treated with 3.4% glutaraldehyde (Cidex Plus; Johnson and Johnson) for high-level chemical disinfection and then air-dried. Before each surgery, endoscopic forceps, esophageal overtube, dilation balloons, and needle knives were cleaned and chemically disinfected with 3.4% glutaraldehyde. Intraperitoneal pressure was monitored and controlled with a manometer (Fisher Scientific manometer, model 8205). Disposable, sterile endoscopic clips (Resolution Clips; Boston Scientific) were used to close bowel lacerations.
Preoperative care
Animals were kept without food (nil per os [NPO]) for 24 hours before surgery. For survival experiments, preoperative enrofloxacin 5 mg/kg i.m. was administered on the day of surgery.
Anesthesia
All procedures were performed under general endotracheal anesthesia. Pigs were preanesthetized with telazol 4 mg/kg i.m., ketamine 2 mg/kg i.m., xylazine 2 mg/kg i.m., and atropine 0.04 mg/kg i.m. Induction was done with isoflurane 3%–5% via mask, delivered with a precision vaporizer prior intubation. General anesthesia was administered with isoflurane 1%–3.5%.
Surgical procedure
Transgastric and transcolonic access
(a) Transgastric access: A single-channel upper endoscope was introduced through the mouth. A complete examination of the stomach was done. The endoscope was then used to place an overtube (US Endoscopy) into the esophagus. Gastric lavage with sterile water and antibiotic solution (Cefazolin 1 g in 200 mL normal saline) was performed through the scope. The solution was allowed to dwell for 15 minutes. The stomach was then washed with sterile water. A sterile double-channel endoscope was then inserted into the stomach through the overtube. External pressure was exerted on the abdominal wall to identify the anterior abdominal wall for gastric incision. Next, a needle knife gastrotomy was performed at the site of stomach wall indentation and balloon dilated to 15 mm over a guidewire for endoscopic access to the peritoneal cavity.
(b) Transcolonic access: Transcolonic access to the peritoneal cavity was obtained as previously described. 9 A single-channel upper endoscope was advanced into the colon via the anus/rectum and two sequential sterile water enemas were administered. The anus and perineum were cleansed with an external Betadine scrub. Residual stool in the rectosigmoid was removed with snares, aggressive washing, and suctioning. Antibiotic lavage was performed with cefazolin as described earlier. A betadine wash was performed through the endoscope. A sterile double-channel endoscope was then inserted to about 25 cm from the anus. Access to the peritoneal cavity was achieved using a needle knife, guidewire, and balloon dilation as described earlier in the section on transgastric access.
Small bowel injury
Intentional small bowel lacerations were made using an electrocautery needle knife (Boston Scientific) to mimic accidental intestinal injury during NOTES. About 1–2-cm incisions were performed (1-cm laceration in the first two animals followed by 2-cm lacerations in subsequent cases). The length of the laceration was gauged by comparing it with an open endoscopic biopsy forceps. The needle knife was embedded into the bowel wall till a full-thickness perforation was made into the intestinal lumen. Full-thickness perforation was confirmed by visualization of the mucosa and advancement of the needle knife into the small intestinal lumen.
Endoscopic repair of small bowel injury
This study focused on the immediate repair of intraoperative small intestinal injury during NOTES. Initially, repair was attempted in a nonblinded fashion by the same endoscopist who performed the small bowel laceration to test the feasibility of endoscopic therapy using currently available endoscopic devices. The injured segment of the small intestine was grasped with a forceps. Endoscopic repair was then started by placing an endoclip (Resolution Clip; Boston Scientific) at one end of the laceration. The entire length of the cut was then systematically clipped, taking care not to leave gaps between clips to eliminate potential sites for leaks. Leak test was performed by instilling sterile water onto the laceration site (submerging the repaired segment) and checking for air bubbles.
As experience with this technique of repair increased, repair was attempted in a blinded fashion by a second endoscopist not present at the time of the initial laceration. This blinded endoscopic surgeon performed NOTES abdominal exploration and attempted to identify the complication site and treat the injury.
Endoscopic closure of the small intestinal laceration was considered successful if (1) the injured segment of intestine could be successfully identified within 30 minutes and repaired with a negative leak test in nonsurvival cases or, (2) in the case of survival experiments, the animal had an uneventful postoperative course (with no evidence of leak or abscess at necropsy 1 week after surgery). Endoscopic management of the intestinal laceration has to be considered unsuccessful if (1) the lacerated segment of intestine could not be located within 30 minutes, (2) the entire laceration could not be successfully closed with endoclips, (3) leak test was positive, or (4) survival animals developed postoperative peritonitis or bowel obstruction from inadequate closure and small bowel leak. Animals have to be euthanized in this situation per protocol to minimize pain and suffering (especially if the enterotomies could not be found or adequately closed).
Postoperative care
Acute studies
Nonsurvival studies were performed in 9 animals: 1 cadaver (first case) and 8 live-anesthetized nonsurvival animals that were euthanized immediately postoperatively.
Survival studies
Survival studies were performed in 3 animals. Postoperatively, a single dose of flunixin meglumine 1.1 mg/kg i.v. was given at the end of surgery. For survival surgeries (1-week survival period), analgesia was provided as per the following protocol: buprenorphine 0.01–0.02 mg/kg i.m. at the start of the procedure and then at 12 hours; flunixin meglumine 1.1 mg/kg i.m. at the end of the procedure; and then either or both drugs as needed beyond 24 hours. Regular diet was resumed the following morning. Animals were closely monitored daily for signs of distress, behavior changes, loss of appetite, and signs of bleeding and peritonitis (fever, abdominal pain, poor food and water intake, lethargy, and decreased activity). At the end of the specified survival time of 1 week, the pigs were euthanized.
Necropsy
Before euthanasia, pigs were anesthetized with a ketamine (20–25 mg/kg) and xylazine (2–4 mg/kg) cocktail i.m. and then euthanized with ≥150 mg/kg pentobarbital sodium i.v. At necropsy, the peritoneal cavity was inspected for abscesses, bleeding, or damage to surrounding structures. The abdominal pelvic cavity was examined for free fluid. After the repaired segment of the small bowel was isolated, it was studied for adequacy of closure, adhesions, or evidence of infection. Leak test was then performed to assess successful closure of the enteral rent.
Results
Twelve pigs underwent either transgastric (n=10) or transcolonic (n=2) peritoneoscopy (1 cadaver [first case], 8 live anesthetized, and 3 one-week survival studies). The small bowel was identified by direct visualization after gaining endoscopic access into the peritoneal cavity. Intentional enteral lacerations 1–2 cm in length were successfully made in all animals using an electrocautery needle knife to mimic accidental small bowel perforation (Fig. 1A and B). Full-thickness perforation was confirmed in all cases. Fifteen small bowel lacerations were performed in 12 animals.
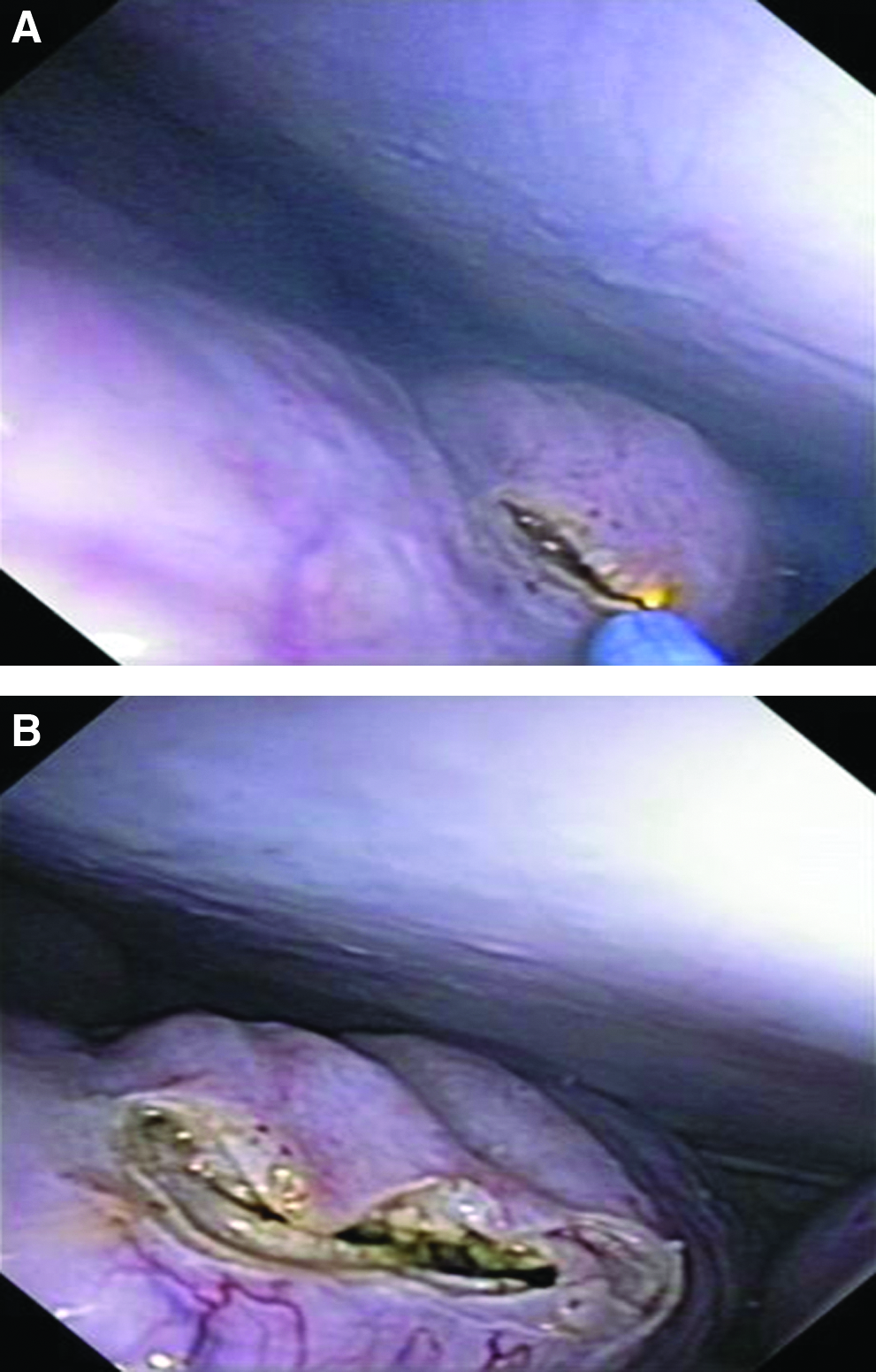
Endoscopic intentional small bowel laceration.
Successful closure of the enteral laceration was achieved in all cases (2–5 clips per laceration, time range: 12–20 minutes) in the nonblinded arm (n=10) of the study as shown in Figures 2 and 3. Endoscopic clips (resolution clip; Boston Scientific, Natick, MA) were able to adequately close the enteral rent without leak. All 3 survival animals had an uneventful postoperative course without any complications and did not require additional analgesia. Food intake and bowel movements were not compromised. At necropsy, there was no evidence of bleeding, perforation, or damage to surrounding structures. Enterotomy sites in survival animals were well healed without evidence of necrosis, adhesions, abscess, bleeding, or spillage of intestinal contents in the peritoneal cavity (Fig. 4). There was no evidence of small bowel luminal obstruction. Leak test was negative in all these animals. Closed gastrotomy and colotomy sites were seen without bleeding, infection, or adhesions.
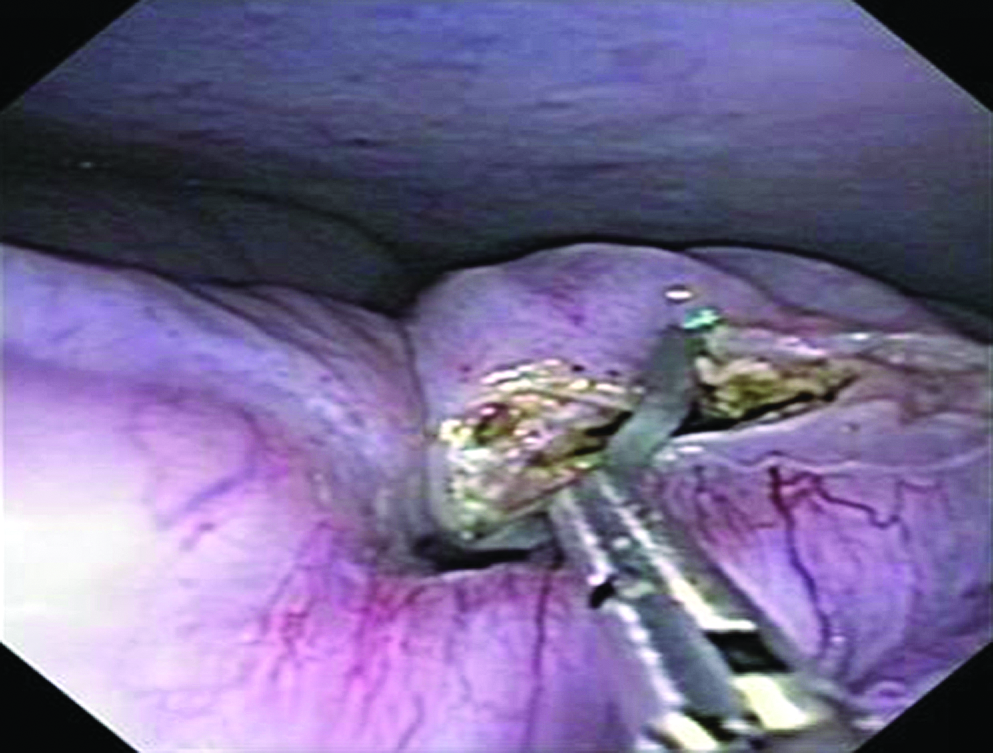
Endoscopic closure of small bowel laceration: the edges of the enterotomy being approximated with an endoscopic clip.
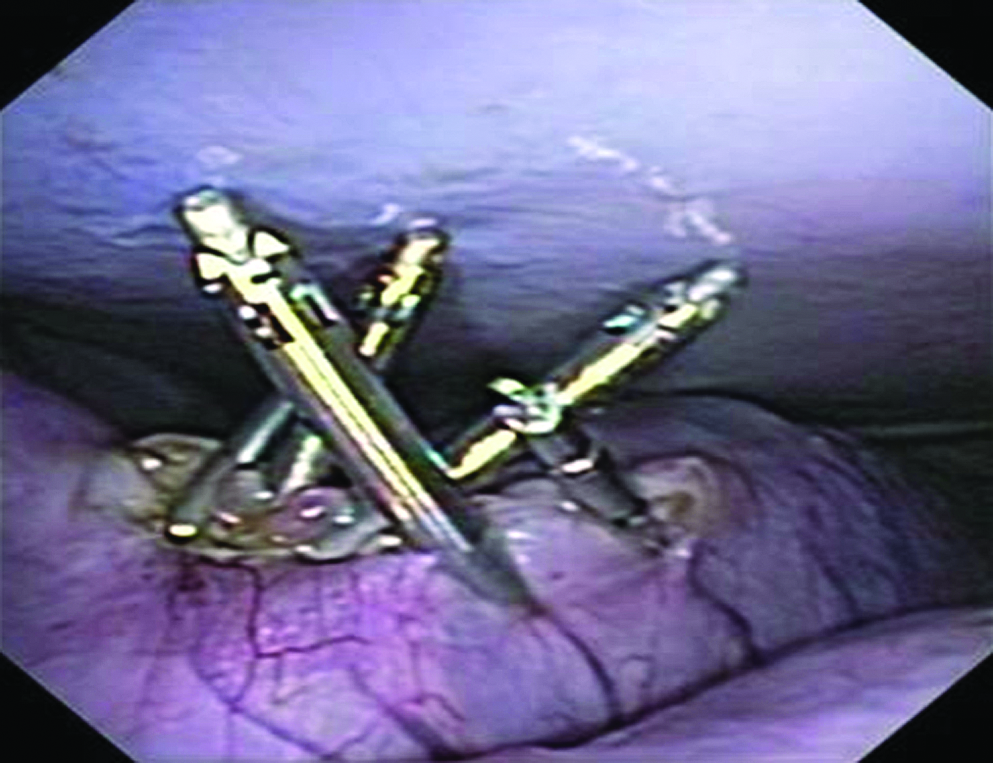
Complete closure of the full-thickness small bowel laceration with endoclips purely via natural orifice translumenal endoscopic surgery.
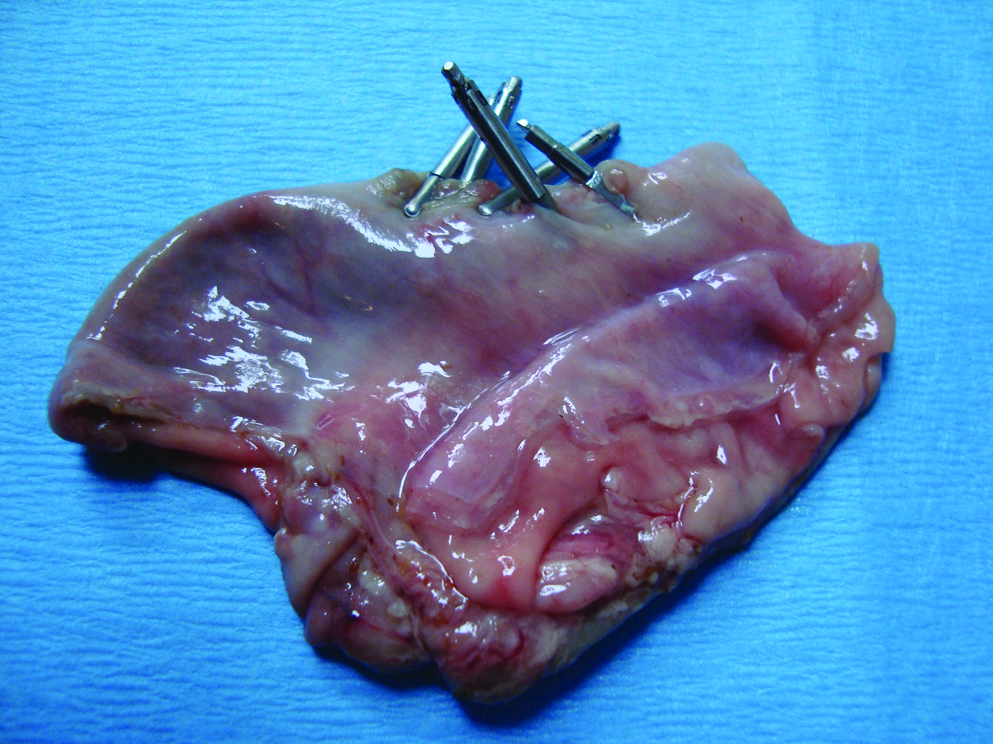
Small bowel specimen at necropsy showing no evidence of necrosis, adhesions, abscess, or bleeding at the site of enterotomy closure.
In the blinded arm, small intestinal lacerations could not be identified by the blinded second endoscopist in both animals under study, as the injured segment of small intestine deflated after the laceration and was lost amidst surrounding bowel loops. These 2 animals were immediately euthanized as predetermined in the protocol, because the enterotomies could not be found. Necropsy revealed open small bowel lacerations. Further studies were not attempted in the blinded arm as it was felt that the entire small bowel could not be adequately examined with currently available flexible endoscopes and accessories to reliably identify and close the site of laceration.
Discussion
The proposed advantages of NOTES over conventional surgery include decrease in postoperative pain, hernias, and adhesions, reduced hospital stay, and absence of a visible scar. This has led to great enthusiasm in this field with recent reports of human NOTES from various parts of the world.13–16 As more complex NOTES procedures are attempted, complications are bound to occur. Ideally, the surgical endoscopist should be able to manage intraperitoneal complications successfully without the need to resort to either a laparoscopy or laparotomy.
Traditionally, surgery has been the mainstay of treatment for bowel perforations. Recently, however, endoscopic clips have been successfully used in the intraluminal closure of fistulas, leaks, and perforations in the gastrointestinal tract. 17 To date, there are no data on the NOTES management of small intestinal lacerations.
In this study, purposeful enteral lacerations were created to mimic small bowel perforations that could occur during routine NOTES procedures. These may occur during peritoneal access, peritoneoscopy, or actual intra-abdominal surgery. Our data suggest that these small bowel lacerations can be adequately repaired intraoperatively via natural orifices using standard currently available endoscopic accessories if the site of injury is known. None of the animals in our study required any extra postoperative analgesia or showed signs of sepsis, peritonitis, or feeding difficulties. All animals had a negative leak test and an uneventful recovery indicating successful closure of primary access sites and sites of intestinal injury in the nonblinded arm of the study. However, in the blinded arm, closure of the intestinal laceration was unsuccessful as the site of injury could not be identified with currently available endoscopes and accessories. Hence, it cannot be overemphasized that complications during NOTES are best avoided.
A few points in our study are worth highlighting. First, various different endoscopic clips are currently available. 18 These include (a) Quickclip2 (Olympus Corp.), (b) Triclip (Cook Medical Inc.), (c) Resolution clip (Boston Scientific), (d) InScope Multiclip Applier (Ethicon Endosurgery Inc.), and (e) Over-the-Scope clip (Ovesco Endoscopy). 18 We used Resolution clips, which are widely used in endoscopic practices around the country for achieving gastrointestinal hemostasis. The prongs of this clip can be opened and closed as needed and rotated, thus allowing precise control for tissue approximation and endoscopic repair in small spaces. A recent article by Raju described techniques of endoclip closure of gastrointestinal perforations during intraluminal endoscopy. 18 Our technique was similar and these endoclips performed very well (provided the site of laceration was evident) in approximating the edges of the laceration. The first clip was placed at one end of the laceration. This seemed to bring the edges of remaining laceration closer and simplified subsequent clip closure. Enteral rents could be successfully closed with 2–5 clips per laceration. Second, as even a small gap in the incision could result in peritonitis and sepsis, meticulous closure of the small bowel incision was performed. Complete closure of the enteral perforation was confirmed by the leak test. We found all of our repaired lacerations to be leakproof with a negative leak test. This was also further consolidated in survival studies without postoperative complications. Third, necropsy examination of the repaired segment of the small intestine in survival animals did not show any evidence of luminal compromise (i.e., stenosis) or adhesions. Postoperative animals had good food intake without signs of intestinal obstruction. Fourth, in the blinded arm, locating the site of laceration after intentional perforation was unsuccessful and quite challenging even though endoscopic repair was attempted soon after the enterotomy. The perforated and therefore deflated segment of intestine was lost amidst other adjacent loops of bowel. The lacerated intestinal segment could not be identified even after lifting adjacent bowel loops (“running the bowel”) with available endoscopic forceps in an attempt to expose the site of injury. This suggests that NOTES repair of small bowel lacerations may currently be performed only with available endoscopic devices, provided the site of injury is known. Hopefully, better tools (e.g., forceps, graspers, and retractors) specifically designed for NOTES will be developed, which will allow complete assessment of the intestine in the future.
Our study is limited by the following factors: (1) lack of comparison with standard laparoscopic closure of intestinal perforations. However, the study was designed to test the feasibility of NOTES repair of small bowel injuries with currently available flexible devices and not to compare it with laparoscopic closure. (2) There was a relatively small number of experimental animals. (3) There was a lack of long-term data on outcomes of endoscopic closure of small intestinal perforations with respect to incidence of adhesions and bowel stenosis. (4) Bowel injuries were caused by the investigators themselves and it may be argued that small intestinal lacerations were only performed in those intestinal segments that were well suited for endoscopic repair; however, this initial study focused on the feasibility of repair of these injuries using currently available endoscopic devices purely via natural orifices. (5) Lacerations were repaired soon after causing bowel injuries. It may be claimed that endoscopic repair is easier in this setting, because septic peritonitis has not been yet developed. We also point out that our study was designed to assess intraoperative endoscopic repair of bowel lacerations that are apparent during the primary NOTES procedure itself. We believe that if such bowel injuries are discovered during NOTES, they will need immediate attention and may be managed endoscopically with currently available devices purely via natural orifices, as described in this study. We describe the endoscopic management of immediate intraoperative complications (i.e., bowel laceration) and further studies are required to assess the ability to manage early and delayed NOTES complications when peritonitis may have already set in. (6) Findings in animal models may not be directly extrapolated to human NOTES.
For NOTES to be accepted into wider clinical practice, management of complications will play a major role. This study provides the initial data that endoscopic management of small bowel laceration is feasible with endoclips purely via natural orifices if the site of laceration is evident. As NOTES advances and surgical systems and tools specifically developed for NOTES become available, it may be possible to adequately examine the small bowel for successful repair of all injuries.
In conclusion, our study shows that small intestinal injuries are difficult to localize with currently available flexible endoscopes and accessories. Endoscopic clips, however, may be adequate for closure of small bowel lacerations if the site of injury is known.
Footnotes
Disclosure Statement
No competing financial interests exist.