
Abstract
Abstract
Background:
Pericardial cysts are usually asymtomatic, benign, congenital mediastinal lesions but may also be acquired after cardiothoracic surgery. The purpose of the study was to evaluate surgical approach and results of our experience with pericardial cysts.
Patients and Methods:
A total of 12 patients who had undergone surgical treatment for pericardial cyst between February 1999 and August 2010 were retrospectively evaluated. All patients were analyzed according to the symptoms, method for the diagnosis, cyst location, management, and outcomes.
Results:
The mean age was 50.4±17 years (range, 23–68 years) with a female-to-male ratio of 8:4. Pericardial cyst were located in the right hemithorax in 8 (67%) patients and left hemithorax in 4 (33%) patients. The cysts were resected by thoracotomy in 4 (33%) patients and by video-assisted thoracic surgery in 8 (67%) patients. There was an excellent long-term follow-up with no morbidity or mortality.
Conclusion:
Videothoracoscopic surgical removal of pericardial cysts is an excellent surgical intervention without serious morbidity and mortality.
Introduction
Materials and Methods
A total of 12 patients undergoing surgical treatment for pericardial cyst between February 1999 and August 2010 were retrospectively reviewed. All patients were analyzed according to the symptoms, method of diagnosis, location of cysts, surgical technique, and outcomes. All patients signed informed consent before surgery. Preoperative chest X-ray and thoracic computed tomography (CT) scan had been used to confirm the diagnosis. Standard posterolateral thoracotomy or videothoracoscopy with three-port technique was used for total excision. VATS was performed under general endotracheal anesthesia with a double-lumen endotracheal tube inserted to allow for ipsilateral lung collapse and single-lung ventilation. Patients were placed in the lateral position used for open thoracotomy. The table was maximally flexed to widen the intercostal spaces. The first trocar, the thoracoscopic trocar, was placed in the midaxillary line in either the sixth or seventh intercostal space for insertion of the thoracoscope into the chest cavity. Placement of other trocars was also guided in general by the location of the target pathology. The three ports were positioned on the chest in an upside-down pyramid configuration, with the lesion at the apex. The working ports were spaced as far as possible from the camera and from each other to minimize the interference of the shafts of the instruments with each other and also to prevent the instruments from obscuring the field of vision. Single-chest tube was used in all cases and removed on the first postoperative day unless otherwise indicated. Postoperative histopathological examination revealed the diagnosis of pericardial cyst in all patients.
Data analysis was performed using SPSS version 16.0 for Windows.
Results
Demographic data of patients are described in Table 1. The mean age was 50.4±17 years (range, 23–68 years), with a female:male ratio of 8:4. Pericardial cysts were located in the right in 8 (67%) patients and in the left cardiophrenic angle in 3 (25%) patients. Atypical location was observed in 1 (8%) patient, that is, next to the aortic arch. Total excision of the cysts was performed in all patients. Operation type and side of the patients are described in Table 2. Operation time for VATS procedure was 24±2 minutes (range, 20–30 minutes). The mean hospital stay was 1.5±0.7 days (range, 1–3 days). There were no surgery-related complications or mortality. There was no recurrence of the cysts.
Discussion
Pericardial cysts are caused by an incomplete coalescence of fetal lacunae during the development of the pericardium. 4 Histologically, these cysts are unilocular, are lined by endothelium or mesothelium, contain clear serous fluid, and are thus referred to as “spring water cysts” 5 (Fig. 1). They are usually solitary cysts adjacent to the pericardium, but 20% of them communicate with the pericardium (Fig. 2). Pericardial cysts may be also acquired after cardiothoracic surgery, although there was no such a patient in our series. 1
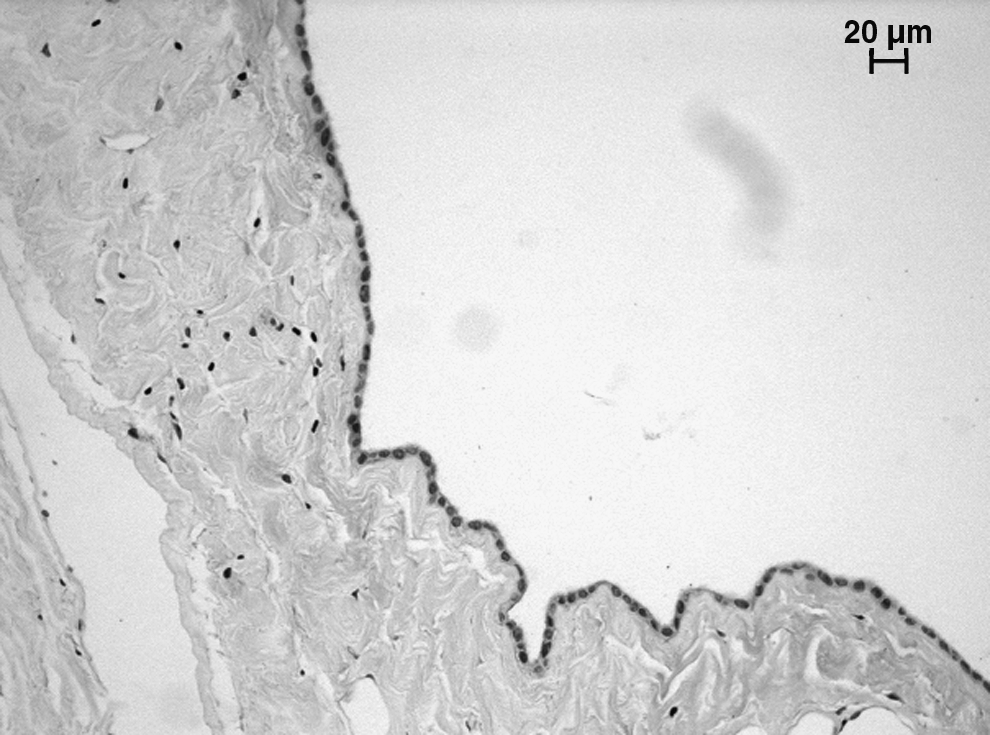
Patient 12: Histological features of a pericardial cyst (single-layer flattened mesothelial lining and a laminated fibrous wall) (hematoxylin and eosin,×200).
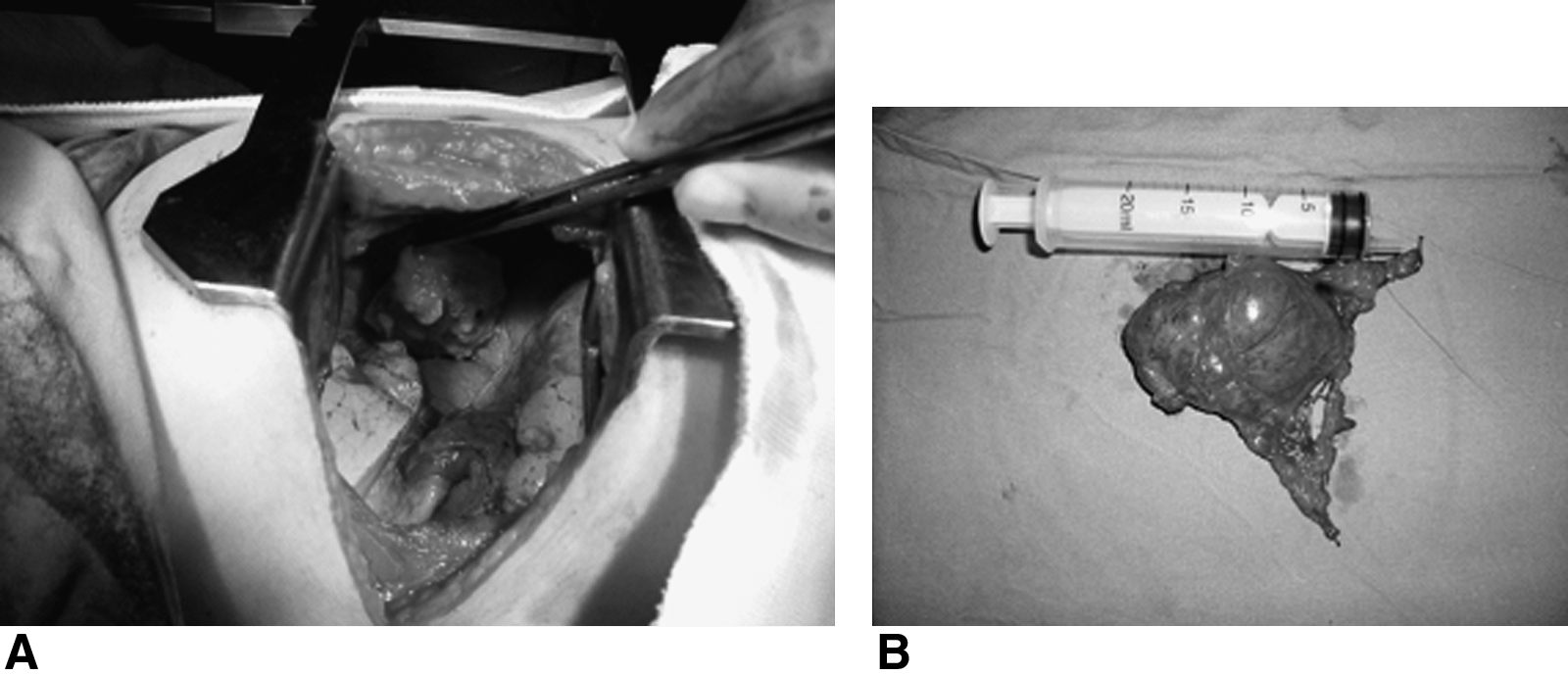
Patient 11: Intraoperative
The majority of pericardial cysts are asymptomatic. They can cause symptoms of dyspnea, thoracic pain, and cough and can mimic tricuspid stenosis, pulmonary stenosis, or constrictive pericarditis depending on the size of the cyst and compression of the mediastinal structures. 3 Only 3 (25%) patients had been symptomatic in our series and this correlated with the literature.
Pericardial cysts are usually detected in middle-aged adults, most frequently in the third or fourth decade of life, and equally in men and women. 3 However, our data do not correlate well with the literature as the patients' mean age was 50.4±17 years and 67% were women.
The most usual radiographic appearance of the pericardial cysts is a well-defined, smooth-walled round mass located along the right border of heart. 3 Once suspected on the chest X-ray, thoracic CT scan with intravenous contrast has been a commonly used modality to confirm the diagnosis. Thoracic CT scan usually shows a sharply defined, thin-walled, oval homogeneous masses and fluid-filled cystic lesion with a near-water density of 0–20 Hounsfield units and fails to enhance with intravenous administration of contrast material. However, as not all cysts have a water density and can have a density higher than water (30 to 40 Hounsfield units), these pericardial or mediastinal cysts may resemble soft tissue masses. 6 The diagnosis can be especially difficult when the lesion occurs outside their typical location of the right cardiophrenic angle (Fig. 3). The differential diagnosis should take into consideration solid tumors, which include angioma, lipoma, neurogenic tumor, sarcoma, lymphoma, bronchogenic carcinoma, metastasis, granulomatous lesion, and abscess. 3 Two-dimensional echocardiography is a noninvasive modality to delineate the exact location of a pericardial cyst and to differentiate a cyst from other potential diagnoses such as a prominent fat pad, left ventricular aneurysm, prominent left atrial appendage, aortic aneurysm, and solid tumors. 1 Transesophageal echocardiography can be useful if transthoracic echocardiography is inadequate in delineating the diagnosis. 7
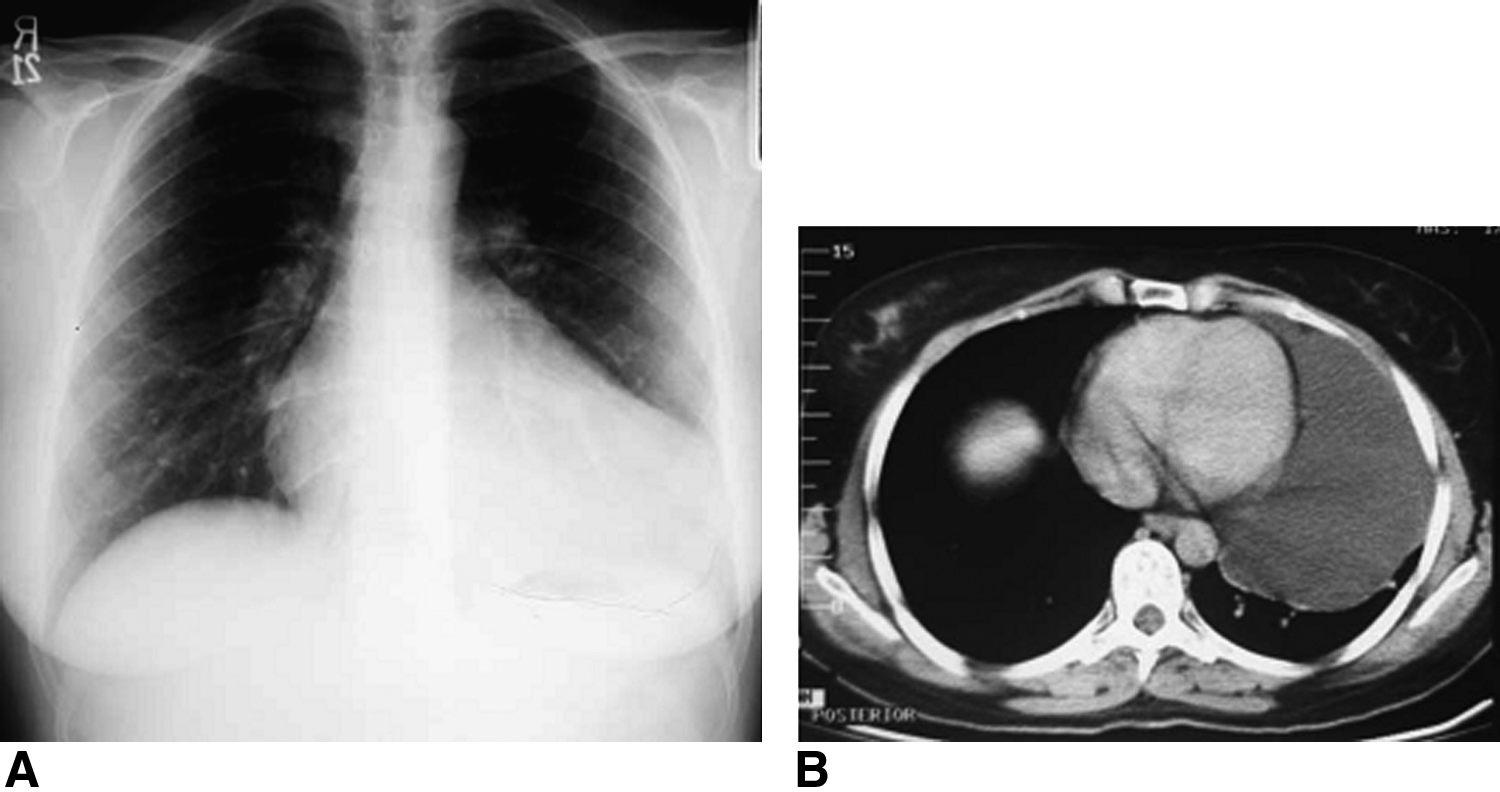
Patient 6:
Surgical resection is widely accepted as the treatment of choice when a patient has symptoms related to a mediastinal mass or the diagnosis is uncertain.2,8 Some authors do not operate on patients with radiographic evidence of pericardial cysts, because these surgeons state that any procedure carries a small risk and patients can be left worse with postthoracotomy pain, which may follow thoracoscopy. 9 In selected nonurgent patients, VATS should be considered as an alternative method of treatment, especially in high-risk surgical cases. Minimally invasive thoracoscopic resection of a pericardial cyst is a good alternative option to open surgical resection, because it minimizes surgical trauma and postoperative pain, has a shorter recovery period, and has a better cosmetic outcome.10–12 We used a thoracoscopic procedure in 8 (67%) patients and there were no postoperative problems. Another alternative surgical procedure is aspiration of the pericardial cyst during mediastinoscopy. 13
Percutaneous aspiration of cysts is an another attractive alternative to surgical resection and may be lifesaving in symptomatic patients, such as those with cardiac tamponade, heart insufficiency, or shock caused by extremely large cysts. 14
Spontaneous resolution of a pericardial cyst has been reported in few cases managed conservatively, the probable mechanism being cyst rupture.15,16 Pericardial cysts usually follow a benign course in the majority of cases, although complications have been reported, which include cyst rupture, erosion of the cyst into adjacent structures, such as the right ventricular wall or superior vena cava, cardiac tamponade, mitral valve prolapse, obstruction of right main stem bronchus, atrial fibrillation, and even sudden death.14,17–23 Considering the complications in nonsurgically treated patients, a conservative treatment approach does not appear to be the best option.
In conclusion, VATS removal of pericardial cysts is the best option with minimal morbidity, without mortality, and with excellent long-term results.
Footnotes
Disclosure Statement
No competing financial interests exist.