
Abstract
Abstract
Crossed ectopia or transverse testicular ectopia (TTE) is an extremely rare anomaly of testicular descent in which both gonads migrate along the same inguinal canal to the hemiscrotum. Fewer than 100 cases have been reported in the literature. Most cases of TTE involve a concomitant inguinal hernia on the contralateral side. A radiological evaluation and laparoscopy are essential for appropriate diagnosis and treatment. Although a correct diagnosis is not preoperatively made in most cases, we present a 15-year-old boy in whom TTE was diagnosed by magnetic resonance imaging. A laparoscopic evaluation and treatment (orchiectomy) was uneventfully performed.
Introduction
The clinical findings are usually a symptomatic inguinal hernia on the side to which the ectopic gonad has migrated and a nonpalpable testis on the other side. The exact diagnosis is usually not determined before surgical intervention. In fact, TTE is inadvertently diagnosed in most patients during surgery for an inguinal hernia or undescended testis.
Although magnetic resonance imaging (MRI) has been suggested for preoperative localization of nonpalpable testis in experienced clinics, laparoscopy is sufficient for both diagnosis and management of TTE and associated anomalies.6–8
In this study, a patient in whom TTE had been diagnosed by MRI and who underwent a laparoscopic evaluation and orchiectomy is presented.
Case Report
A 15-year-old boy in whom TTE had been diagnosed was referred to our department for further evaluation and treatment. He was admitted with a complaint of painless swelling in the right inguino-scrotal region for the past 3 months that had been gradually increasing. A physical examination revealed a well-developed right scrotum and a poorly developed left scrotum. The right testis was of normal size and palpable in the right hemiscrotum, but the left testis was impalpable.
An MRI demonstrated that the right testis was in a normal location, but the left testis was located in the right inguinal region. We planned a laparoscopy to confirm the diagnosis, further understand the anatomy of the testes and spermatic cords, and exclude the presence of Müllerian duct structures. We performed the laparoscopy by using the open Hasson technique after making a 1-cm semicircular skin incision just under the umbilicus.
During the laparoscopic exploration, a small testicle was found in the right deep inguinal ring (Fig. 1). The vessels and the vas of the ectopic testis were crossing the midline from the left to the right side. Additionally, a right inguino-scrotal hernia was found that consisted of a processus vaginalis. The presence of Müllerian duct structures was ruled out by a detailed explorative laparoscopy. Then, we decided to convert to open surgery because of our limited experience in laparoscopic surgery and close proximity of vascular structures. After a right inguinal transverse incision, a right inguinal exploration was performed. During the hernia dissection, an ectopic small testicle was found in the vicinity of the deep inguinal canal. Cord structures and ectopic testis vessels were mobilized and excised through the right inguinal incision (Fig. 2). The testicle was small in size (∼7 mm), whereas the right testis was normal (∼3×2 cm). Thus, a left orchiectomy/herniotomy was performed, and testis prosthesis was placed into the left hemiscrotum. The patient's postoperative course was uneventful. The histopathologic examination of the excised testis was reported as Sertoli cells only. No tumor cells were observed.
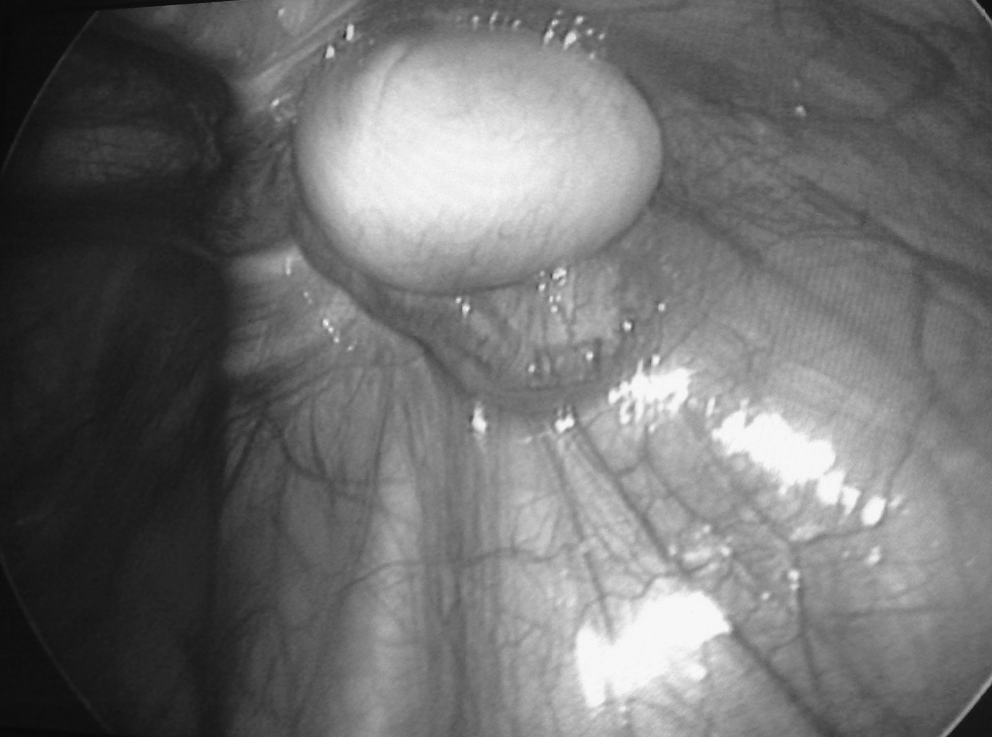
A small testicle was found in the right deep inguinal ring. The vessels and the vas of the ectopic testis were crossing the midline from the left to the right side.

Cord structures and vessels of ectopic testis were mobilized and taken out of the body through the right inguinal incision. The testicle was small in size (∼7 mm), and the right testis was normal in size (3×2 cm).
Discussion
Testes are normally located in the scrotum at birth. Ectopic testis has been reported to occur at different sites, including the superficial inguinal pouch; suprapubic, femoral, and perianal areas; at the base of the penis; and in the transverse inguinal and scrotal region. 7 The most common ectopic location is within a superficial pouch between the external oblique and Scarpa's fascia, a structure called Denis Browne's pouch.
Migration of the testis to the opposite side, in which the testes pass through the same inguinal canal, is known as TTE. The ectopic testis may lie in the opposite hemiscrotum, the inguinal canal, or at the deep inguinal ring. In our case, the left testis was located at the transverse deep inguinal ring.
Hypotheses on descent do not include adequate observational or experimental data to explain TTE, and the mechanism of pathological descent is currently not clear. However, experimental studies suggest that the gubernaculum plays an important role. 9
TTE has been classified according to associated abnormalities: that is, with inguinal hernia alone (type I, 40%–50%), persistent or rudimentary Müllerian duct structures (type II, 30%), or other anomalies without Müllerian remnants (type III, 20%; hypospadias, inguinal hernia, scrotal abnormalities, and pseudohermaphroditism). 10 Thus, our case was categorized as TTE type I.
Due to the high incidence of associated abnormalities, the presence of TTE indicates further exploration for other abnormalities. Ultrasonography, MRI, and laparoscopy may be helpful in the evaluation; although laparoscopy is solely sufficient for the diagnosis, evaluation, and treatment of this entity. 7 We generally prefer laparoscopy for diagnosing and treating nonpalpable testis. The separation of the testicle, vas, and vascular pedicle requires more experience to avoid damage, and the vas deferens and the epididymis may be fused. In these cases, a transseptal orchiopexy through the same inguinal ring should be performed. Laparoscopy-assisted surgery in which the ectopic testis is grasped with a Kelly clamp through the inguinal canal followed by standard orchiopexi is another option for the treatment of TTE. 6 In the present case, we decided to convert to open surgery because of the risk of damage to the vas deferantia, cessation of blood supply of the normal testis due to our limited experience in laparoscopic surgery, and close proximity of vascular structures.
The majority of patients are diagnosed during the earlier ages, and the mean age of the presentation is reported as 4 years. 10 However, at 15 years of age, this patient was one of the oldest reported in the literature. We performed orchiectomy because of the contralateral normal testis, his age, and pubertal status. According to the European Association of Urology (EAU) Guidelines, an intra-abdominal testis in a 10-year-old boy or older, with a normal contralateral testis, should be removed. 11
Although the empty scrotum and swelling in the inguino-scrotal region are warning signs of TTE for practitioners, the diagnosis of undescended testis or TTE may be delayed because of the poor socioeconomic and educational status of parents or the health policies in undeveloped countries.
In conclusion, a diagnosis of TTE should be considered if a unilateral hernia is present with concurrent cryptorchidism of the contralateral side. Ultrasonography and MRI are helpful in the diagnosis. Due to associated abnormalities, a detailed exploration is necessary to assess patients, and a transseptal or extraperitoneal transposition orchiopexy requires more advanced surgical experience and skill. Finally, this pathological abnormality should be operated on as soon as possible due to the risks of infertility and progression to malignancy.
Footnotes
Disclosure Statement
No competing financial interests exist.