
Abstract
Abstract
Transanal endoscopic microsurgery (TEM) was described in 1983 for local excision of rectal tumors. In the context of natural orifice translumenal endoscopic surgery, we have modified the original TEM system and developed a new set of instruments. These are more curved and, in addition, steerable. After extensive studies in an ex-vivo model, we developed a novel technique for transanal rectosigmoid resection and colorectal anastomosis. The technique comprises closure of the rectal lumen by purse-string suture, transection of the rectal wall distal to the closure, circumferential mobilization of rectum and mesorectal tissue in the anatomical plane from below upward, control of the inferior mesenteric vessel, removal of mobilized colorectum through the anus, and, finally, the colorectal anastomosis by either stapled or hand-sutured technique. This procedure was performed on three alcohol-glycerol preserved well-built human cadavers (M:F=2:1). The average operating time was 190 minutes. The average length of the resected specimen was 23 cm. There was no fecal contamination or injury to the resected specimen. Postprocedure laparotomy revealed adequate mesorectal resection and no inadvertent injury to other viscera. During dissection in the pelvis, as the resected rectum was pushed upward, an unobstructed “empty pelvis” situation was developed in the operating site, thus facilitating the mesorectal resection. Transanal access for colorectal surgery seems feasible. It provides a precise definition of the distal safety margin, good view of the pelvis for meticulous mesorectal resection, and reduces the abdominal wall trauma. These may enhance the outcome of colorectal resection. However, further clinical studies can only substantiate these findings.
Introduction
In the context of NOTES, we have modified the original TEM system and developed a new set of instruments for translumenal intraperitoneal work. The instruments are long, curved, and, in addition, are steerable. The curve shaft of the hand instrument as well as the effectors inside the shaft is independently rotatable. 11 This system was initially used to perform transvaginal chlolecystectomy, first in experimental 12 and, subsequently, in a clinical set-up. 13 We then developed a technique for transanal rectosigmoid resection and colorectal anastomosis and conducted a controlled experimental trial in an ex-vivo experimental model by using the regular TEM and the new steerable instrument system. 14 The experimental trial demonstrated the feasibility of transanal rectosigmoid resection and a systematic way to perform the endolumenal colorectal anastomosis either stapled or hand sewn. As a next step of development, we set out to validate the technique on human cadavers. Here, we describe the technique and highlight the possible advantages of transanal access for colorectal surgery in human cadavers.
Materials and Methods
Experimental set-up
The procedures were performed on alcohol-glycerol preserved human cadavers. The cadavers were donated to the Institute of Anatomy, Tuebingen University, Germany, for medical education and research.
Surgical technique
The cadaver was placed on modified Lloyd Davis position. The perineal area was cleaned and draped. The surgeon sat between the legs. The rectal lumen was closed by a purse-string suture. The closure was made at either 2 cm or 8 cm from the dentate line.
In the first scenario, the closure was performed under direct vision with a conventional instrument. The rectal wall was then divided circumferentially 0.5 cm anal to the closure. The initial dissection plane was developed with conventional instruments along the anatomical plane and preceded for about 1.5 cm cephalad. The TEM system was then introduced through the anus, and the perirectal space was inflated with gas (Fig. 1).
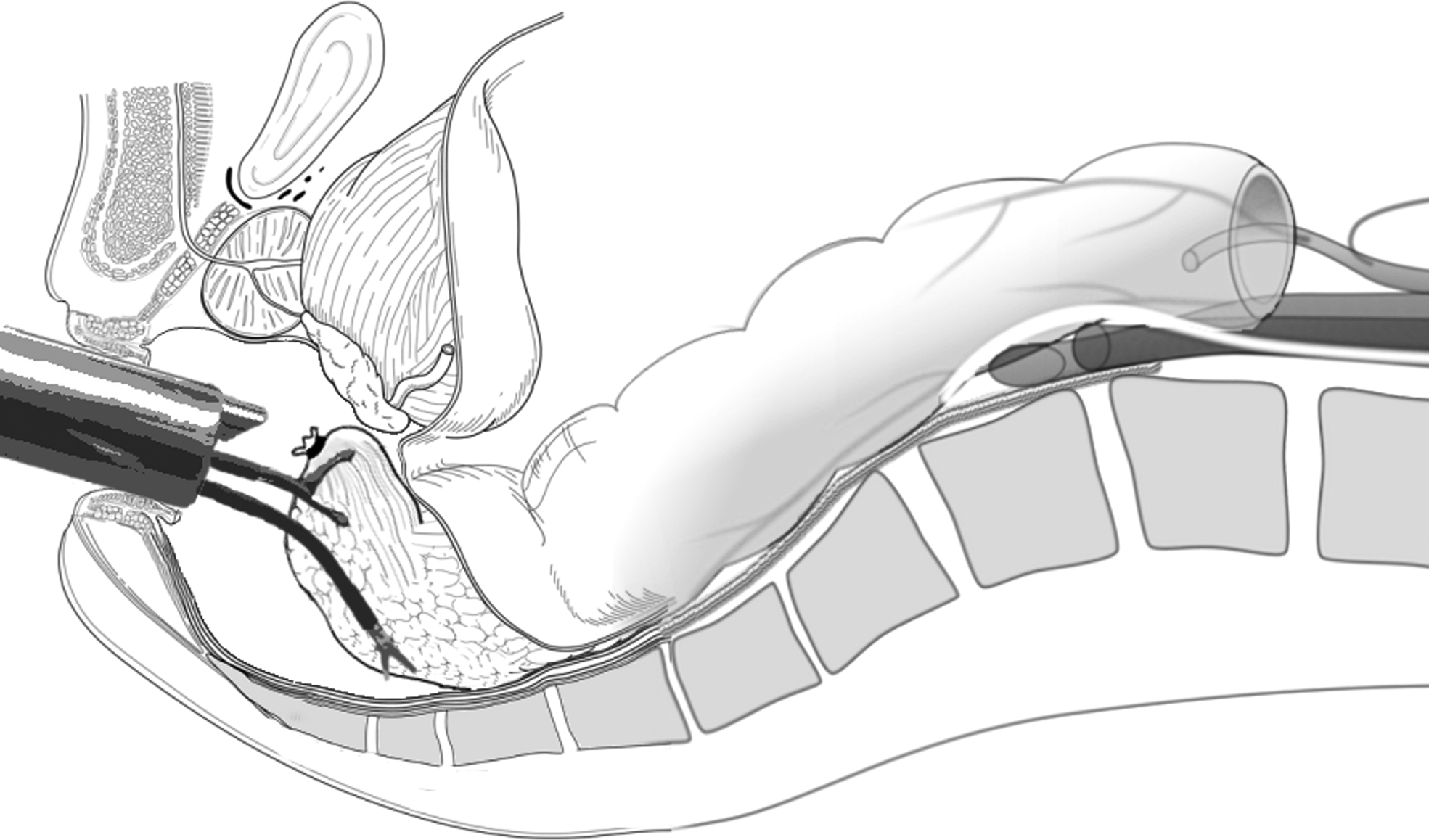
Graphical representation of the dissection in the deep pelvis. The perirectal space is distended with gas. The rectal specimen is held and retracted with a regular transanal endoscopic microsurgery grasper; dissection is performed along the anatomical plane with the new steerable instruments.
In the other scenario, the rectum was closed by endolumenal technique using the TEM system at 8 cm from the dentate line (Richard Wolf GmbH, Knittlingen, Germany) (Fig. 2). The rectal wall was marked circumferentially with coagulation dots 1 cm anal to the closure. Full-thickness rectal transection was initiated with a high-frequency knife along these coagulation points. After complete division of the rectal wall, the dissection plane was developed along the anatomical plane with the TEM instruments.

The technique for endolumenal closure of the rectum. An endolumenal purse string suture is placed at 8 cm from the dentate line. The tail end and the needle end of the thread are kept outside the rectoscope. The threads are then tied with multiple sliding knots.
The further mobilizations of the rectum were carried out anteriorly along the Denonvillers's fascia and posteriorly along the Waldeyer's fascia. The specimen tissue was held by a left-hand TEM grasper. It was retracted to either side or upward for exposure and traction on the operative site. The retraction of the rectal stump toward the abdomen developed an unobstructed “empty pelvis” situation of the operating field (Fig. 3). This “empty pelvis” view, distension of the operative site with gas, and the endoscopic magnification helped identify and develop the dissection plane. The new curve steerable scissor was held on the right hand, and a sharp dissection was carried out along the anatomical plane (Figs. 4 and 5). The bulging of the seminal vesicle was realized anteriorly in the male specimen. The nerve fibers of the lower hypogastric plexus were visualized and protected. The abdominal cavity was entered by dividing the anterior peritoneal reflection (Fig. 6).
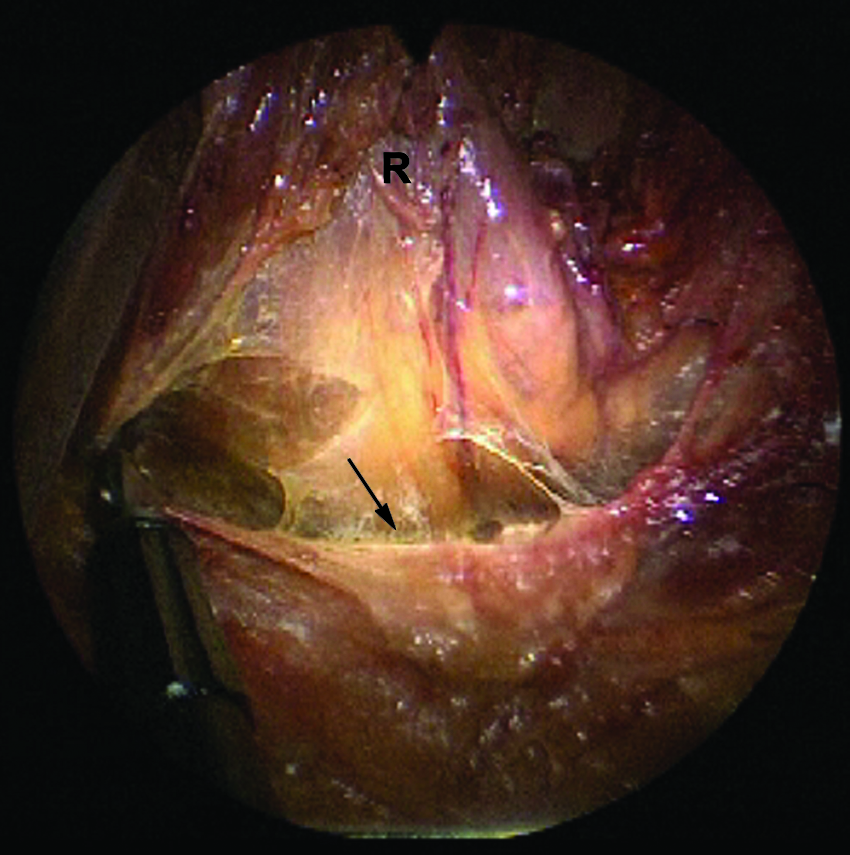
The lower rectum (R) is retracted cephalad for dissection along the presacral avascular plane (arrow). This retraction develops a completely unobstructed “empty pelvis” view at the operating site.
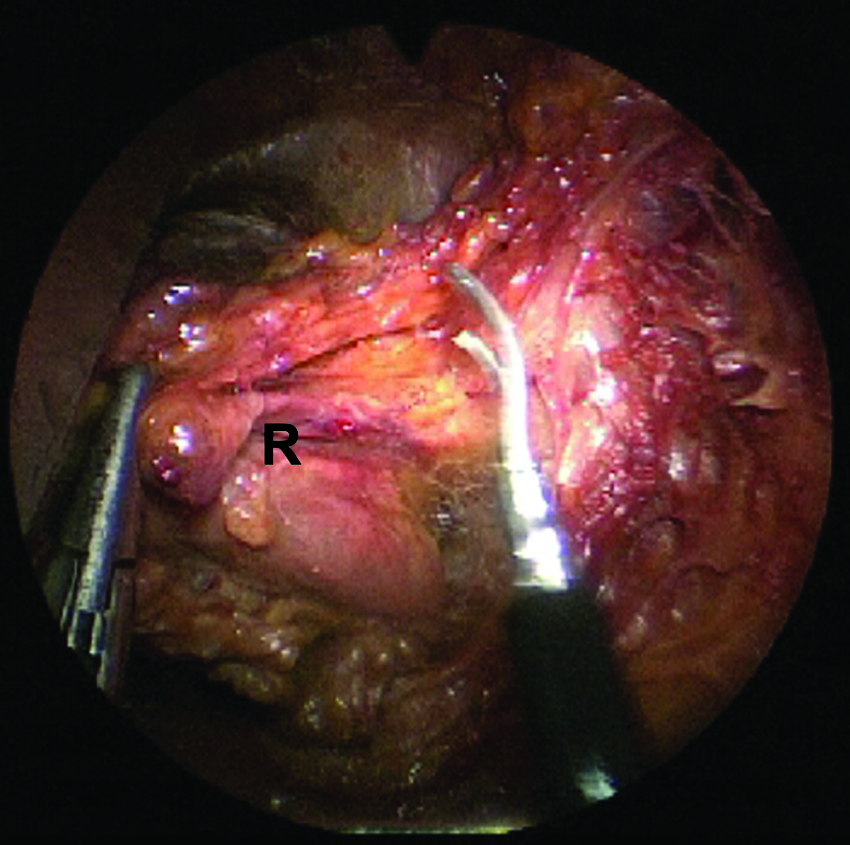
The circumferential mobilization of the lower rectum (R). The rectum was retracted toward right for dissection along the left lateral side. Please note that the avascular dissection plane already developed anteriorly and postero-laterally.
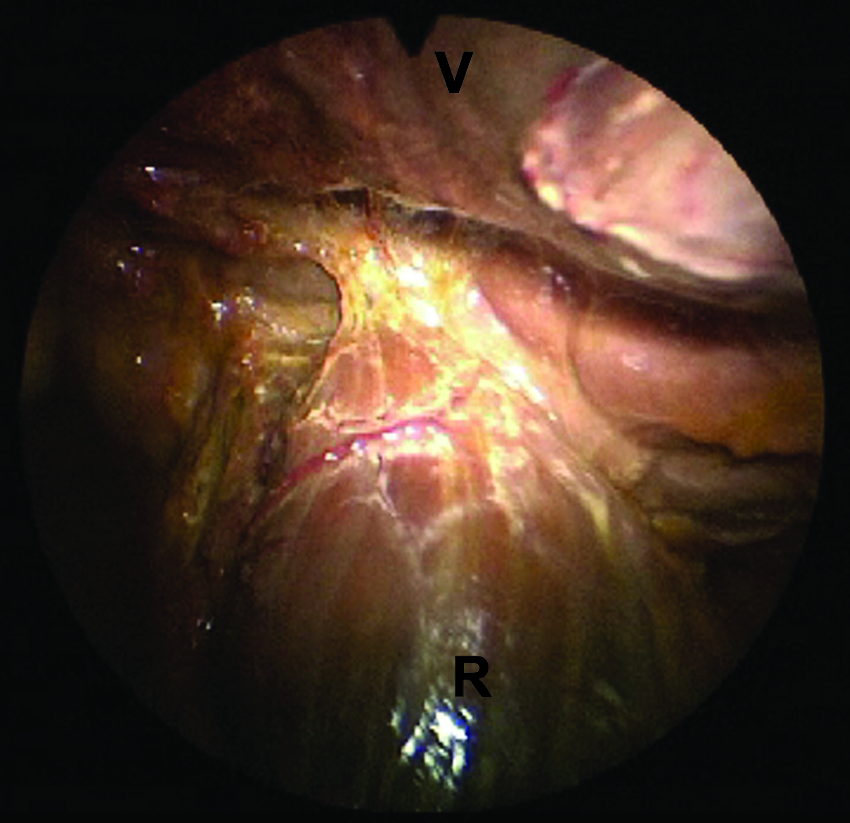
The anterior dissection along the Denonvillers's fascia. Distension of the peri-rectal space with gas facilitated good visualization and meticulous dissection along the fascial plane. R, anterior surface of the rectum; V, posterior vaginal wall.
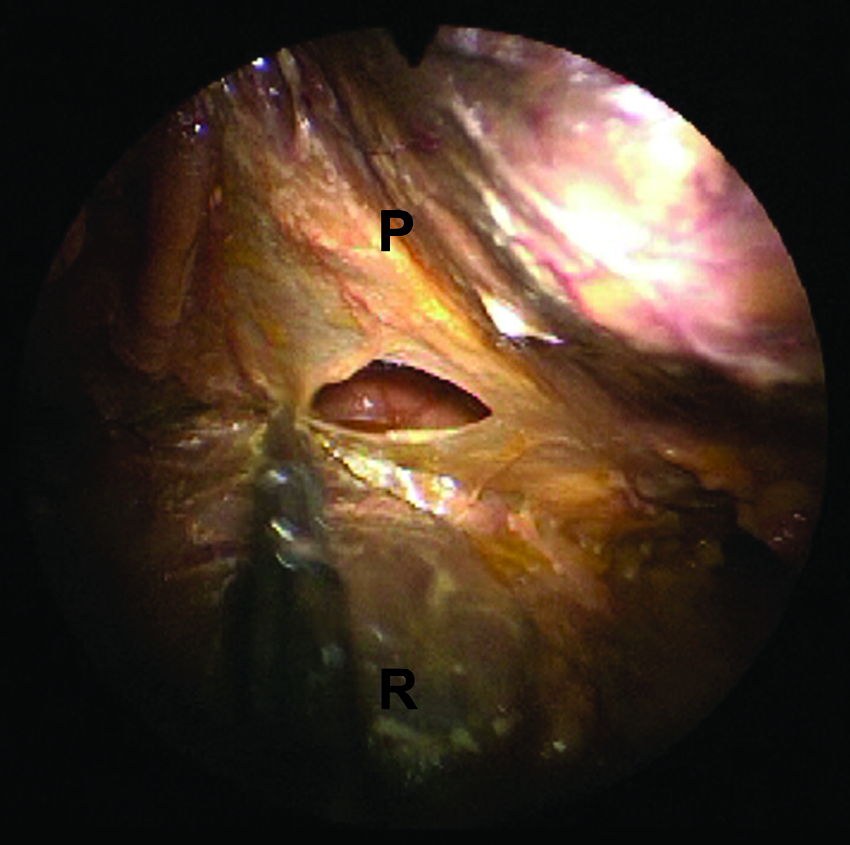
The peritoneum is divided anteriorly to enter into the abdominal cavity. P, peritoneum; R, anterior surface of the rectal wall.
The patient was positioned in steep head-down. The small bowel loops were placed in the upper abdomen. The anatomical orientations for the pelvic structures were made. Further mobilization of the rectum was made from below upward following the surgical plane already developed posteriorly and on both the sides. The ureter on the left side was identified (Fig. 7). The iliac vessels, the aorta, and the inferior mesenteric artery were visualized. The inferior mesenteric artery was skeletanized near its origin and divided between the clips (Fig. 8). The inferior mesenteric vein was clipped and divided supero-lateral to the artery. The left colon was mobilized up to the lower third of the descending colon.
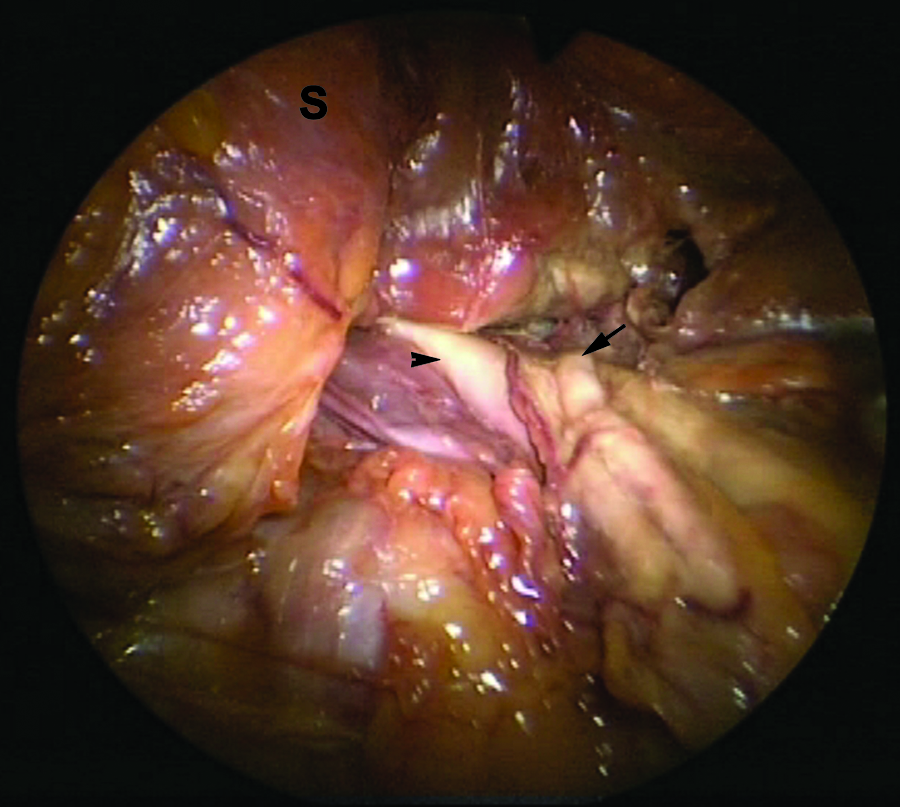
The left ureter is seen crossing over the iliac vessels. S, the sigmoid colon being mobilized and retracted toward the midline, the left ureter (arrow) and the common iliac artery (arrowhead) are seen.
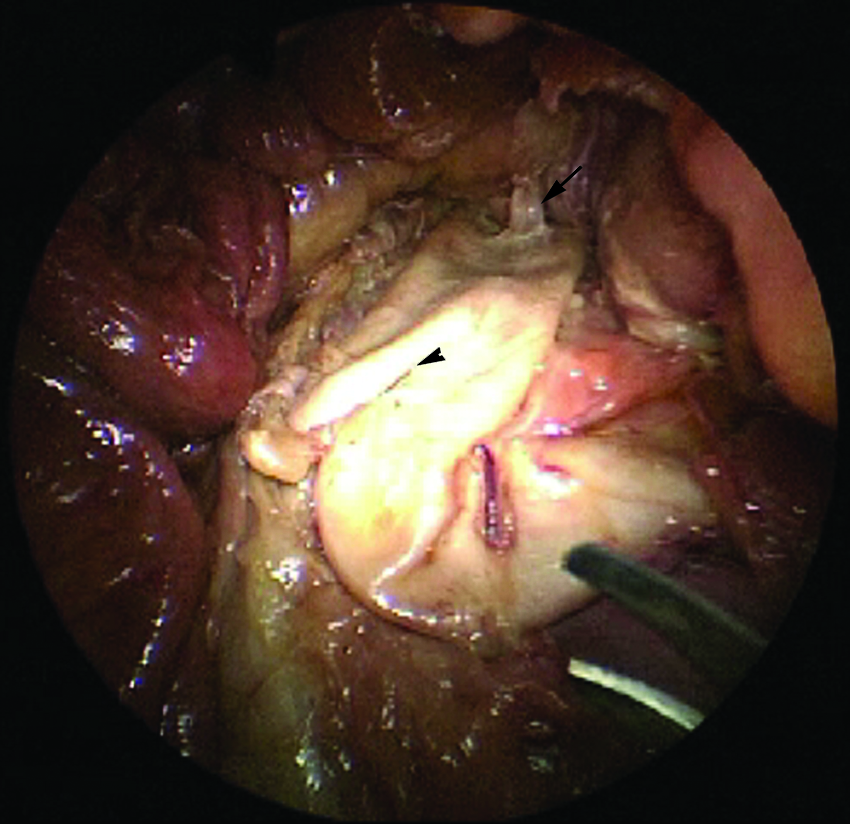
The inferior mesenteric artery (arrow) is skeletanized till its origin from the aorta. The site of bifurcation of the aorta is indicated with an arrowhead.
In the female patient, the fallopian tube and the ovary on the left side were seen.
The mobilized specimen was brought out through the anus (Fig. 9). The specimen was divided close to the anus. The anvil of the stapler was tied with a thread. It was inserted into the colon and secured by a purse-string suture. The cut edge of the rectal stump was sewn by a purse-string suture under direct vision and tied to the rod of the anvil. The anvil was mated to the stapler by pulling the thread already tied to it. An audible click marked the completion of the process. The stapler was fired to complete the low colorectal anastomosis.

The specimen (the rectum and the sigmoid colon) is removed through the anus.
In the other case, where the rectum was divided 7 cm from the dentate line, the transected proximal end of the colon was re-inserted into the pelvis. The TEM system was re-introduced. An end-to-end endolumenal hand-sutured colorectal anastomosis was attempted.
Results
Transanal rectosigmoid resection was performed in three alcohol-glycerol preserved well-built human cadavers (M:F 2:1). In 2 cases, the rectal lumen was closed at 2 cm above the dentate line; and in 1 case, it was closed 8 cm above the dentate line. The average operating time was 190 minutes. The average specimen length was 23 cm, with en-bloc mesorectal tissue. There was no spillage of fecal content during dissection or injury to the resected specimen. The postprocedure laparotomy revealed completeness of mesorectal resection and no inadvertent injury to other intra-abdominal organs. The doughnuts of the two stapled colorectal anastomosis were complete. Direct inspection and digital palpation of the anastomotic line revealed no defect.
The hand-sutured colorectal anastomosis could not be completed due to the poor tissue quality of the post mortem bowel.
The new steerable instruments provided better accessibility to the operating field, which was difficult to access with the regular TEM instruments. The gas distended perirectal tissue and the “empty pelvis” situation of the operating site facilitated identification of the surgical plane and the meticulous dissection along it.
Discussion
In the context of NOTES, feasibility of transanal radical sigmoid resection was first shown on human cadavers by Whiteford et al. 7 They divided the rectum at the level of the upper rectal fold and could mobilize sigmoid colon through the transanal route. However, due to the shorter length of TEM instruments, they could reach up to the first hemorrhoidal artery. Fajardo et al. showed in a multimedia article the feasibility of colorectal resection by using TEM system and a hand port with a long reticulating instrument. 9 Recently, Sylla et al., after a series of animal experiments, 8 reported the first clinical case of transanal rectal resection for a case of rectal cancer. 10 Although Sylla et al. used laparoscopic assistance, three abdominal ports in total for retraction and visualization, the endoscopic dissection of the rectum and mesorectum was achieved entirely through the transanal access with TEM platform. 10
We developed the technique for transanal rectosigmoid resection and colorectal anastomosis on an experimental model in a realistic anatomical situation. The TEM has been in clinical practice for almost three decades now. This extensive clinical evidence and the results of our experimental study made us believe that transanal colorectal surgery is feasible and may provide a better access route for colorectal resection. This cadaver experiment substantiated this belief one step further.
We would like to highlight the advantages of TEM based transanal access for colorectal surgery.
1. Definition of distal safety margin: TEM based transanal access, being an endolumenal procedure, safety margin distal to the tumor can be precisely defined. The precise determination of the distal safety margin is likely to influence the sphincter preservation and oncological clearance, especially in the context of low rectal lesion. 2. Precise mesorectal resection: The gas-distended perirectal space, magnified view, and the “empty pelvis” situation of the operating site are likely to enhance the safety and precision of mesorectal resection. 3. Lack of access-related abdominal wall trauma: TEM based transanal access eliminates the abdominal wall trauma for port placement as well as for specimen removal. 4. Vertical transection of the rectum: The transection of the rectum in laparoscopic colorectal surgery with the present staple technology is often oblique and long. The long division line is a known risk factor for anastomotic leakage.
15
During the transanal access, the rectal division is perpendicular to the long axis of the bowel and avoids the oblique division. 5. Single-port surgery: Transanal colorectal resection, being based on TEM platform, is a single-port surgery. 6. Solo-surgery platform: Transanal colorectal resection bears promise for solo surgery.
Complete segmental rectal resection and end-to-end rectal anastomosis by TEM was reported way back in 1988. 16 Recently, we standardized the technique for endolumenal end-to-end hand-sutured colorectal anastomosis and demonstrated its feasibility and safety in an experimental set up. 14 In the present cadaver experiment, although we failed to complete the hand-sutured colorectal anastomosis, this was purely due to the poor quality of the post mortem bowel, which was not holding the sutures. We believe, that after proper training, endolumenal anastomosis with TEM would not be a difficult issue.
However, the results of this study should be interpreted cautiously regarding the clinical applicability of the technique. The experiments were performed on human cadavers; there are certain indigenous limitations of a cadaver model. The cadaver does not bleed, and the intestinal tissue of the cadaver is not comparable to that of a patient. There was no tumor inside the rectum. Presence of a tumor in situ might influence the “empty pelvis” view at the dissection site. Moreover, the splenic flexure was not mobilized, which is often a fundamental point for rectum and sigmoid resection.
There are certain limitations to the transanal access for colorectal surgery
1. Bacterial contamination: By closing the rectal lumen, we could avoid the tumor cell seedlings and minimize the fecal spillage from the proximal colon. However, the distal rectal stump was always open, and the colon was lying open in the pelvis for hand-sutured anastomosis. This increases the possible bacterial contamination. However, during open colorectal anastomosis, both the colon and the rectum are deliberately kept open inside the abdomen; also, the opening of the rectal lumen to the peritoneal cavity during regular TEM procedure does not increase the infective complications in postoperative period.5,6 Thus, the clinical significance of this transient bacterial contamination may not be relevant. Nevertheless, compared with laparoscopic colorectal surgery, this bacterial contamination will stay as a disadvantage of the transanal technique, at least in its present form.
2. Demanding procedure: TEM is technically a demanding procedure. The new steerable instruments are even more demanding to handle and needs dedicated training and skills to use them.
3. Limited indications: Large tumors or colon with very fatty mesocolon may not be possibly removed through the anus. Thus, the indications for the technique will be limited to small- or medium-sized tumors only.
Conclusions
In conclusion, the transanal access is a promising option for colorectal resection. Transanal access provides a precise definition of the safety margin, good view of the pelvis for meticulous mesorectal resection, and reduces the abdominal wall trauma. These advantages may enhance the outcome of colorectal resection. However, certain aspects such as prevention of bacterial contamination need evaluation, and only further clinical studies can substantiate these findings.
Footnotes
Acknowledgments
The first author acknowledges the MIO, Verein zur Forderung schonender OP Verfahren, Munich, Germany, from which he received a scholarship to pursue his doctoral studies in Germany. All the authors pay tribute to their deceased co-worker Professor G.F. Buess, who initiated this project and participated in the experiment. They also thank Ms. Lilo Mailander, M.A., Director, Training Center for Minimal Invasive Surgery, and Professor Bernhard Hirt, Department of Clinical Anatomy, University Hospital Tuebingen, for their logistical support to carry out the experiments.
Disclosure Statement
No competing financial interests exist.