
Abstract
Abstract
Background:
Several ventilatory strategies have been introduced to minimize the respiratory and hemodynamic effects of carbon dioxide pneumoperitoneum during laparoscopic surgery. The purpose of this study was to compare the effects of pressure-controlled ventilation (PCV) with that of volume-controlled ventilation (VCV) on the ventilatory and hemodynamic parameters in children undergoing laparoscopic appendectomy.
Methods:
Thirty-four children undergoing laparoscopic appendectomy were randomly allocated to receive mechanical ventilation using either VCV (n=17) or PCV (n=17) mode. Positive end-expiratory pressure (PEEP) 5 cm H2O was applied to all patients. Hemodynamic and ventilatory parameters were measured 10 minutes before pneumoperitoneum (T1) and 30 minutes after pneumoperitoneum (T2).
Results:
Peak and mean airway pressures were significantly increased at T2 from T1 in both groups. Mean airway pressure was significantly higher in the PCV group compared with that in the VCV group. Dynamic compliance was significantly higher in the PCV group than in the VCV group at T2, although it was decreased at T2 from T1 in both groups. Mean blood pressure was significantly increased at T2 from T1 in both groups without intergroup difference. During the study period, SpO2 remained constant without intergroup or within-group differences.
Conclusion:
During laparoscopy, mean airway pressure and dynamic compliance were significantly higher during PCV with 5 cm H2O PEEP compared with that in VCV with 5 cm H2O PEEP. And, as there were no differences in other ventilatory parameters and oxygen saturation, both VCV and PCV can be used safely in children undergoing laparoscopic surgery.
Introduction
The respiratory and hemodynamic effects of pressure-controlled ventilation (PCV) and volume-controlled ventilation (VCV) during CO2 pneumoperitoneum have been studied in adult patients but their results remain controversial.4,5 PCV is used in the management of patients with elevated peak airway pressure, and elevated Ppeak during VCV is the most prominent change of ventilatory parameters in children under pneumoperitoneum. 2 Up to date, the effects of different ventilatory strategies on ventilatory parameters in pediatric laparoscopy have not been assessed. Therefore, the purpose of this study was to compare the effects of PCV and VCV on the ventilatory and hemodynamic parameters in children undergoing laparoscopic appendectomy.
Methods
This study was approved by the institutional review board and informed parental consent was obtained from all patients. Thirty-four children, American Society of Anesthesiologists physical status I or II, aged 3–14 years undergoing laparoscopic appendectomy due to acute appendicitis were prospectively enrolled in the study. Patients with cardiorespiratory disease history or upper respiratory infection symptom were excluded from the study. Patients were randomly allocated to receive mechanical ventilation using either VCV (n=17) or PCV (n=17) mode using computer-generated randomization list generated by a statistician in a sealed envelope.
On arrival in the operating room, patients were monitored with standard anesthetic monitors. Anesthetic management and intraoperative care were standardized. After premedication with intravascular glycopyrrolate 4 μg/kg, anesthesia was induced with propofol 2.5 mg/kg and alfentanil 10 μg/kg and maintained with sevoflurane 1.5–3.0 vol% and air and oxygen (FIO2=0.6). Intubation of the trachea was facilitated with rocuronium 0.6 mg/kg.
All patients were ventilated with an S/5 Avance anesthetic machine (GE Healthcare, Madison, WI). In all patients, the inspiratory:expiratory ratio was 1:2 and end-expiratory pressure was maintained at 5 cm H2O throughout the procedure. After induction of anesthesia, tidal volume (VT) and Ppeak were initially set to deliver a tidal volume (VT) of 8 mL/kg in the VCV and PCV groups, respectively. Then, Ppeak was reset after pneumoperitoneum to match the initial expired VT in the PCV group. The respiratory rate (RR) was adjusted to maintain an end-tidal carbon dioxide tension between 32 and 38 mmHg, apart from ventilation mode. Ppeak, Pmean, RR, VT, and minute ventilation were recorded at 10 minutes before pneumoperitoneum (T1) and 30 minutes after pneumoperitoneum (T2). Dynamic compliance of the respiratory system was calculated as VT/(Ppeak – positive end-expiratory pressure [PEEP]).
A standard operative technique was used. With this technique, CO2 pneumoperitoneum was created with a closed Veress needle technique maintaining a 12 mmHg intra-abdominal pressure. After abdominal insufflation, patients were placed in a 15° Trendelenburg position. Laparoscopic appendectomy was performed through two ports of 10 mm and two of 5 mm in the standard position with the legs closed.
Sample size was calculated based on a previous study. 2 To detect a mean difference±standard deviation in lung compliance of 8±6.3 L/cm H2O with an alpha error of 0.5 and power of 90%, 14 patients were required in each group. To compensate for a dropout rate of 20%, 17 patients in each group were included in this study.
Statistical analyses were performed using the SAS software (version 6.12; SAS Institute, Cary, NC). Data are expressed as mean±standard deviation, median (IQR [range]), or number of patients. The distribution of data was determined using Kolmogorov–Smirnov analysis. Statistical analysis was performed using t-test. A P value of .05 was considered statistically significant.
Results
There were no significant differences in patient characteristics between two groups (Table 1). Hemodynamic parameters are summarized in Table 2. Mean arterial pressure was significantly increased at T2 from T1 in both groups without intergroup differences. Heart rate was not significantly changed in both groups during the study period.
Values are mean±standard deviation, median (interquartile range), or number of patients. There were no significant differences between the two groups.
VCV group: volume-controlled ventilation with external positive end-expiratory pressure (PEEP)=5 cm H2O; PCV group: pressure-controlled ventilation with PEEP=5 cm H2O.
Values are mean±SD.
P<0.05, compared with T1 value within the group.
T1, 10 minutes before pneumoperitoneum; T2, 30 minutes after pneumoperitoneum; SBP, systolic blood pressure; MBP, mean blood pressure; DBP, diastolic blood pressure; HR, heart rate.
Ventilatory parameters and oxygen saturation are displayed in Figure 1. Minute ventilation and end-tidal carbon dioxide tension were significantly increased at T2 from T1 in both groups without intergroup differences. Ppeak and Pmean were significantly increased at T2 from T1 in both groups. During the study period, Pmean was significant higher in the PCV group than in the VCV group, whereas Ppeak was comparable between the groups. Dynamic compliance in the PCV group was significantly higher than that in the VCV group at T2, although it was significantly decreased at T2 from T1 in both groups. During the study period, SpO2 remained constant without intergroup or within-group differences. No patient had desaturation (SpO2 <96%).
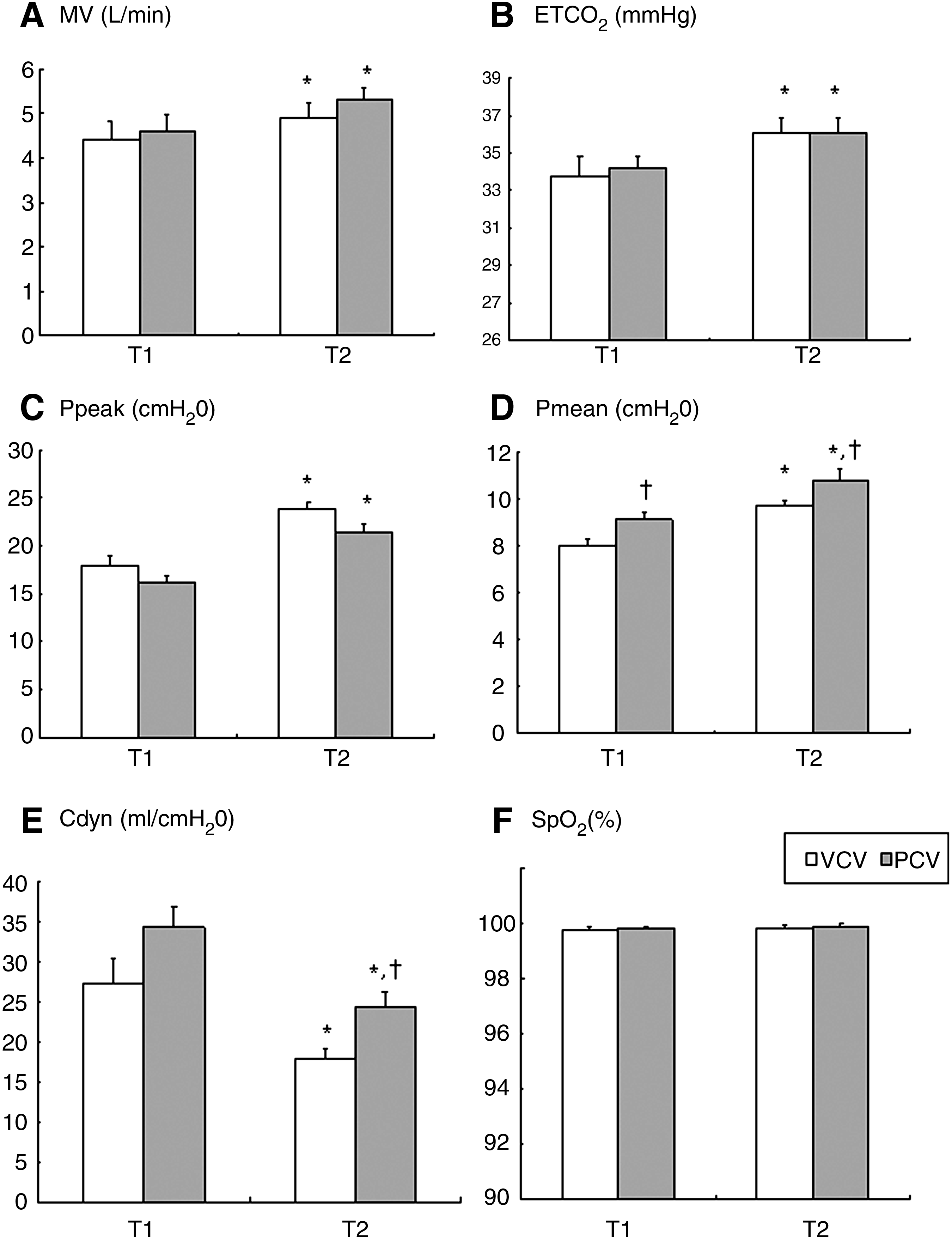
Airway pressure and dynamic compliance during laparoscopic appendectomy in children. Error bar displays standard error. VCV group: volume-controlled ventilation with external positive end-expiratory pressure (PEEP)=5 cm H2O; PCV group: pressure-controlled ventilation with PEEP=5 cm H2O. T1: 10 minutes before pneumoperitoneum; T2: 30 minutes after pneumoperitoneum.
Discussion
This study demonstrated that Pmean and Cdyn were significantly higher with PCV with 5 cm H2O PEEP compared with that with VCV with 5 cm H2O PEEP in children during laparoscopic appendectomy under CO2 pneumoperitoneum. No other differences of ventilatory parameters and oxygen saturation between PCV and VCV could be noted.
Unlike VCV, PCV uses a decelerating flow, which tends to compensate for any potential reduction in ventilation caused by pressure limitation. 6 As a result, PCV has different gas distribution, and its fast VT delivery depends on the pressure limitation and the chest compliance. In the PCV mode, alveoli with short time constant may be initially overinflated but a more homogeneous distribution of the VT in all the ventilated alveoli follows, reducing the amount of atelectasis by an improved alveolar recruitment. 7 In this study, the Cdyn after CO2 insufflation was higher in the PCV group compared with that in the VCV group and this result was of interest, because it may be associated with a change in gas distribution. 8 Balick-Weber et al. 5 has also demonstrated that Cdyn significantly improved after switching from VCV to PCV in adult patients with pneumoperitoneum. However, they suggested that there was no short-term beneficial effect of PCV compared with VCV during laparoscopy. 5
Reduced compliance impedes adequate pulmonary gas exchange and pneumoperitoneum may promote collapse of dependent lung regions during anesthesia. The functional residual capacity (FRC) is low in children. During laparoscopy, FRC decreases further because of a variety of factors including diaphragmatic displacement, reduction in chest wall dimension and muscular tone, as well as changes in the intrathoracic blood volume. If FRC falls below closing capacity, small airways collapse, resulting in atelectasis, pulmonary shunting, and hypoxemia.
9
In this study, a PEEP of 5 cm H2O was applied to all patients to prevent alveolar collapse from increased intra-abdominal pressure as has been suggested by Pighin et al.
10
They emphasized the use of sufficient level of PEEP during laparoscopy in children, because alveolar collapse increases venous admixture and oxygen desaturation more rapidly occurs in children.
10
In our patients, peripheral oxygenation did not deteriorate as indicated by stable Sp
In this study, Pmean was significantly higher in PCV than in VCV during the study period. Such a result was not surprising. In fact, using a decelerating flow waveform could result in a higher Pmean according to the mathematical models.11,12 A previous study reported that increases in Pmean appeared to be directly related to increases in oxygenation. 13 However, as the low Pmean had been generated during our study, positive effect of elevated Pmean on oxygenation seems to be clinically insignificant. The previous study has reported that no significant improvement of arterial oxygenation could be noted after switching from VCV to PCV in adults undergoing laparoscopy. 5
The most prominent changes of ventilatory parameters during pneumoperitoneum in children have been reported as the significant increases in peak airway pressure with simultaneous decrease in lung compliance. 1 Wedgewood and Doyle 1 reported 28% decrease in the lung compliance after head down tilt and CO2 insufflation during VCV, which is consistent with the results of this study. Their result was comparable to our results. In this study, Cdyn decreased by 29% in the VCV group and 25% in the PCV group after head down tilt and CO2 insufflation.
Beside its effect on the lung mechanics, pneumoperitoneum may influence cardiac performance through transmission of the intra-abdominal pressure to the intrathoracic cavity. Huettemann and collegues 3 have demonstrated a significant decrease in septal wall motion and fractional shortening with an intra-abdominal pressure of 12 mmHg under VCV with 5 cm PEEP in children. They suspected nonuniform transmission of the increased intrathoracic pressure to the left ventricle as the most likely cause but other factors such as lung compliance, ventricular function and filling status were also considered. As the dynamic compliance was lower during VCV in this study, PCV may have some beneficial effect on left ventricular wall motion during pneumoperitoneum. However, further study is needed to elucidate the effect of ventilatory mode on left ventricle wall motion during pneumoperitoneum in children. One of the limitations of this study is the age range of patients included in this study. The age ranged from 3 to 14 years, which is too large to apply the result of this study to small children. Further study excluding adolescent patients would have given more valuable information on the optimal ventilation mode during laparoscopy in small children.
Conclusions
During laparoscopy, mean airway pressure and dynamic compliance were significantly higher during PCV with 5 cm H2O PEEP compared with that in VCV with 5 cm H2O PEEP. As there were no differences in other ventilatory parameters and oxygen saturation, both VCV and PCV can be used safely in children undergoing laparoscopic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.