
Abstract
Abstract
We performed bilateral robotic single-site partial nephrectomy on a 51-year-old man with bilateral renal tumors. Left partial nephrectomy without renal arterial clamping and right partial nephrectomy with a warm ischemic time of 29 minutes were performed through a single umbilical port and one additional port. The total operative time was 350 minutes including 238 minutes of robotic console time. There were no operative complications and no open conversions. Follow-up exams over a 12-month period showed no tumor recurrence. Our report shows the technical feasibility of bilateral robotic single-site partial nephrectomy.
Introduction
Patients and Methods
A 51-year-old man (body mass index, 22.96 kg/m2) presented with intermittent, painless gross hematuria. He had no specific medical or surgical history. His serum creatinine level was 0.9 mg/dL, and urinalysis findings were red blood cell count 20–25/high-power field (HPF) and white blood cell count 0–1/HPF. Abdominal computed tomography showed a 2.8-cm, well-enhanced round mass in the midpole of the right kidney and a 0.6-cm, hyperdense cystic mass with enhancement in the midpole of the left kidney (Fig. 1). After obtaining the informed consents of the patient and his family, bilateral robotic single-site partial nephrectomy was performed.
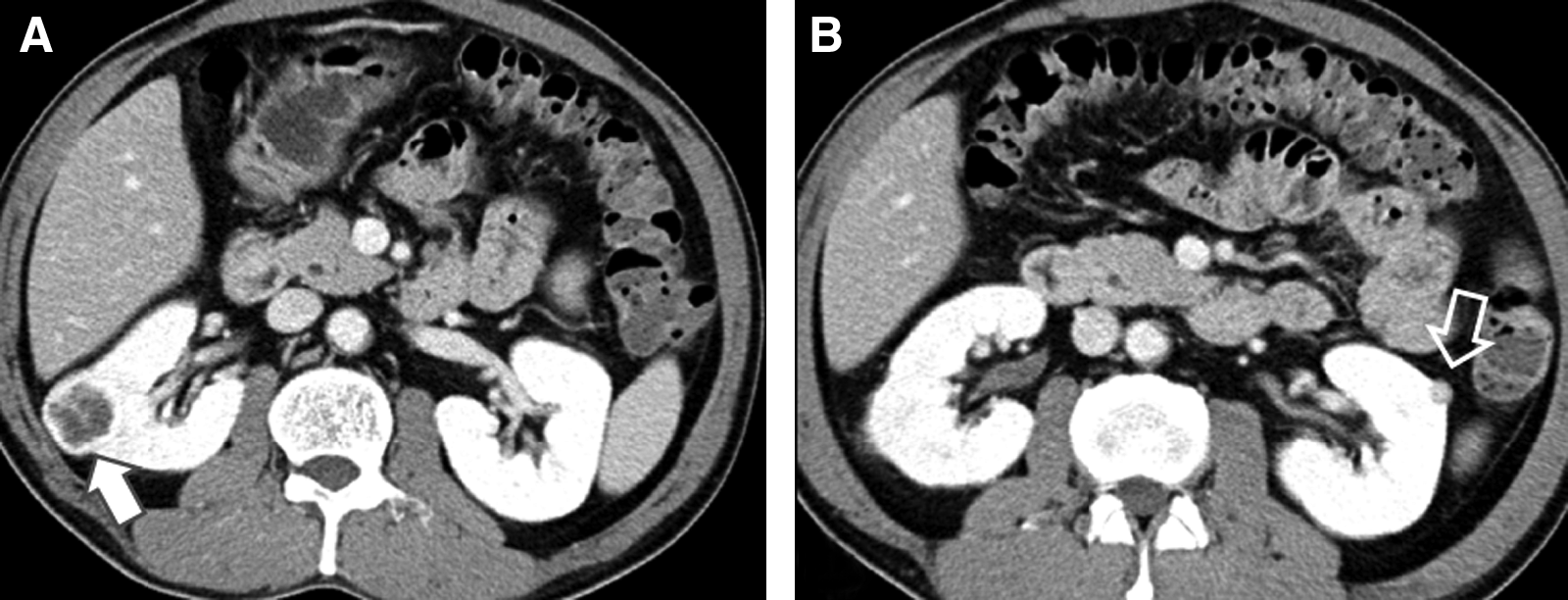
Abdominal computed tomography scan images.
The patient was positioned in a 70-degree lateral position with left-side elevation. Bilateral robotic single-site partial nephrectomy was performed transperitoneally. A homemade-port device was made by a size 6 surgical glove and a small-sized Alexis wound retractor (Applied Medical). An Alexis wound retractor was inserted in the peritoneal cavity through a 3-cm periumbilical incision, and it was rolled up. A surgical glove was attached into the wound retractor, and fingers of the glove were secured. Three trocars including an 11-mm trocar for the robotic camera and two 8-mm trocars for robotic arms, were inserted into the glove of the homemade-port and fixed using rubber bands (Fig. 2).
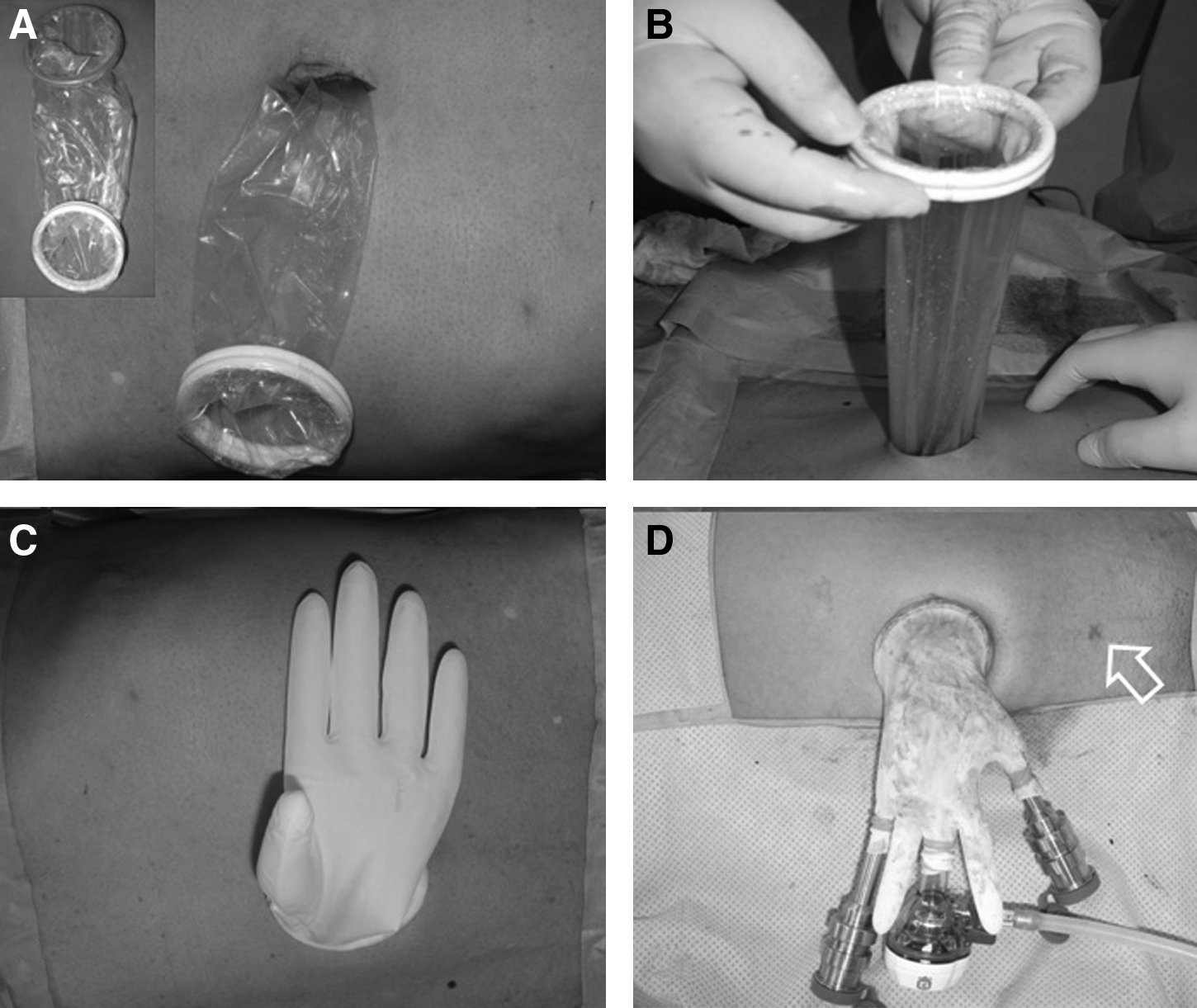
Development of the homemade-port device.
After carbon dioxide insufflation to maintain an intraperitoneal pressure of 14 mmHg, a 30-degree, 10-mm robotic camera with upward configuration and two robotic instruments of robotic arms were inserted into the peritoneal cavity through the port device. Additionally, an 11-mm trocar was inserted into the lower abdomen (Fig. 3). The operation was started with left partial nephrectomy. Robotic instruments including bipolar Maryland forceps, monopolar scissors, and needle drivers were used. The white line of Toldt was incised at the lateral border of the colon. After incising Gerota's fascia, the perirenal fat was dissected to identify the tumor. The renal mass with surrounding fat was identified on the midpole of the left kidney. The tumor was scored by electrocautery, although a 0.5-cm tumor margin was maintained. The renal artery was not clamped; because the tumor was small and exophytic. Robotic scissors was used to excise the tumor, and electric coagulation was used for hemostasis of the parenchymal bed. The renal parenchyma with capsule was sutured using Vicryl® 2-0 attached to Hem-o-lok® clips (Weck Closure Systems). A continuous suture was initiated from outside the renal parenchyma and continued to compress the renal parenchyma. Hem-o-lok clips were placed after each throw of the running suture. Finally, absorbable clips (Lapra-Ty®; Ethicon, Inc.) were applied instead of tying knots. After confirmation of hemostasis, a fibrin sealant (Tisseel®; Baxter AG) and a cellulose mesh (Surgicel®; Ethicon, Inc.) were placed on the suture sites, and a fascial suture using Vicryl 3-0 was performed. The excised specimen was entrapped into a laparoscopic pouch and stored in the operative field.
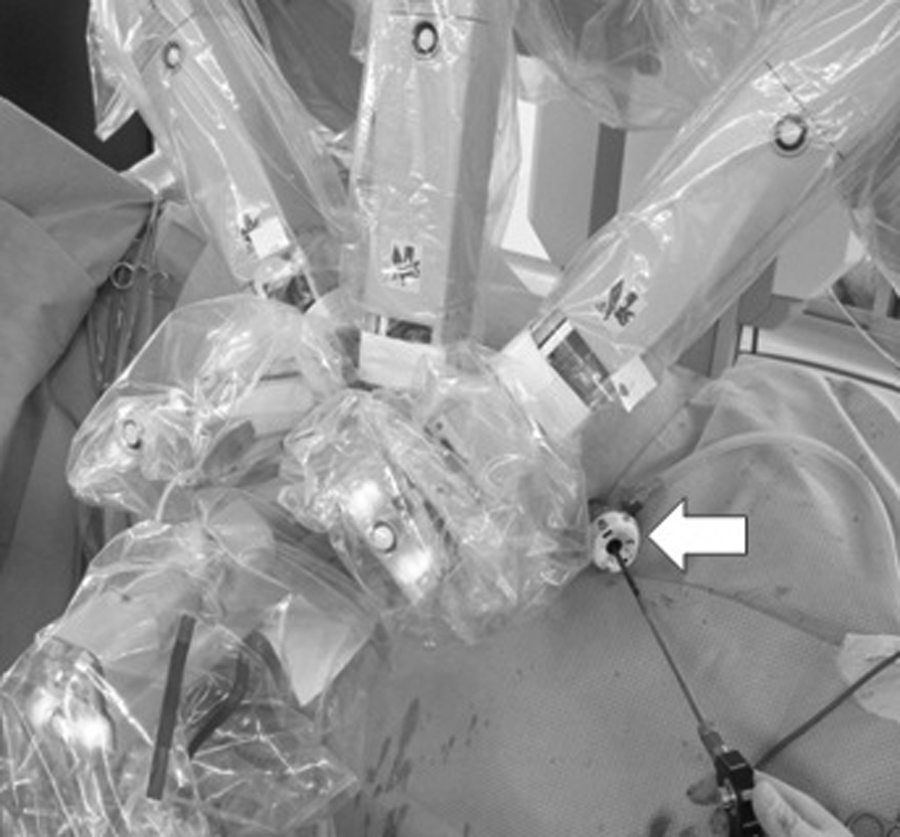
External views. A robotic camera and 2 robotic arms were attached into the homemade port and docked. An additional port for assistant (arrow) was placed in the lower abdomen.
After releasing the robotic arms, the patient was re-positioned in the 70-degree lateral position with right-side elevation. Right partial nephrectomy was performed, similar to left partial nephrectomy. However, the right renal artery was clamped with two laparoscopic bulldog clamps (Fig. 4). A diamond flex retractor was used to elevate the liver. The damaged renal pelvocalyceal system was repaired using absorbable Vicryl 3-0 sutures. Bleeding was controlled by electric coagulation, a fibrin sealant (Tisseel; Baxter AG), and a cellulose mesh. The renal parenchyma with capsule was sutured continuously using Vicryl 2-0 and 3-0, Hem-o-lok clips, and Lapra-Ty clips. After the procedure, the bulldog clamps were removed. A Jackson-Pratt drain was inserted in the operative field. After releasing the robotic arms, the excised specimens within the laparoscopic pouch were removed with the single-site device.
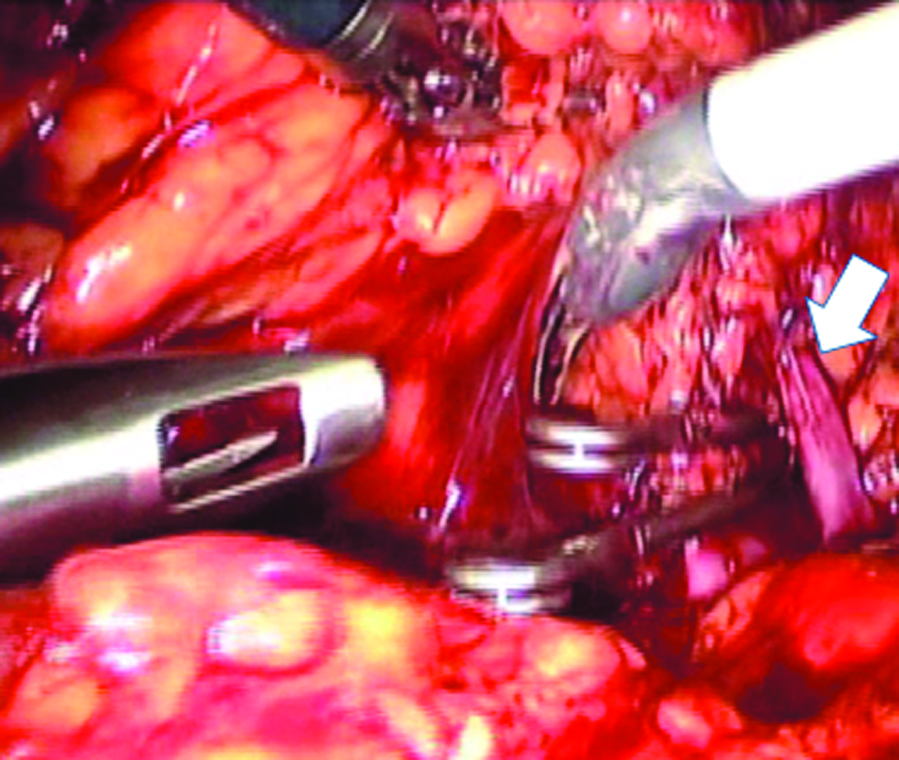
Operative views through a 30-degree robotic camera with upward configuration. The right renal artery was clamped with 2 laparoscopic bulldog clamps. The renal vein (arrow) was saved.
Results
The operation was completed successfully without open conversion. The operating time was 350 minutes, and the robotic console time was 238 minutes: 110 minutes for left and 128 minutes for right partial nephrectomy. The warm ischemic time of right partial nephrectomy was 29 minutes. The estimated blood loss was 522 mL. There was no need for transfusion, and no complications occurred. Postoperative pain control was achieved by patient control analgesia with morphine (40 mg) and ketorolac (150 mg) for 2 days. Postoperative initiation of ambulation and diet commenced after 1 day. The drain was removed on postoperative day 4. The length of hospital stay was 8 days.
Pathologic results showed a 0.8-cm sized angiomyolipoma in the left kidney and a 2.2-cm, clear cell type of RCC in the right kidney. Surgical margins were negative at both sites. The serum creatinine level on postoperative day 1 was 1.5 mg/dL; on postoperative day 7, 1.07 mg/dL; and at 3 months postoperation, 0.91 mg/dL. Follow-up exams, including abdominal computed tomography, showed no tumor recurrence over a 12-month period.
Discussion
LESS has gained popularity, because it requires a small incision that improves postoperative recovery and cosmesis.3–5 Recent studies have cumulative clinical experience with LESS renal surgery.6–8 However, this surgery requires significant skill and experience. Several articulating laparoscopic instruments are utilized. However, LESS's primary limitation remains manipulation of instruments, including loss of triangulation and frequent clashing of the instruments. To overcome these limitations, the da Vinci surgical system (Intuitive Surgical) was introduced to LESS.9,10
Robotic surgery has been widely adopted in the urologic field. Since it offers a magnified, three-dimensional view and fully articulating wristed instruments, surgeons can perform challenging operations. After introduction of robotic partial nephrectomy (RPN) by Gettman et al., 11 there have been advancements in the surgical technique, favorable operative results, and reports on intermediate-term outcomes.12,13 Particularly RPN is advantageous for treating complex tumors (endophytic, hilar, and multiple tumors). 14 However, long-term assessment of functional and oncological outcomes is needed before RPN becomes standard treatment for small renal tumors.
Robotic single-site surgery in urology started in 2008. Kaouk et al. 15 initially reported successful completion of robotic single-port transumbilical surgery in humans. A multichannel single port (R-port; Advanced Surgical Concepts) was inserted through a 2-cm umbilical incision into the abdomen. The port comprised one 12-mm port, two 5-mm ports, and an insufflation cannula. The da Vinci system was docked, and the camera along with a 5-mm robotic port was introduced through the single port. An additional 5-mm robotic port was placed adjacent to the single port but through the same incision. The remaining 5-mm port was used for the bedside assistant. They have recently reported their initial experiences with robotic single-site radical prostatectomy, dismembered pyeloplasty, radical nephrectomy, and partial nephrectomy.9,10 For the partial nephrectomy, they have completed 2 cases without conversions or complications. A multichannel gel port (Triport; Advanced Surgical Concepts, Bray, Co.) was used. Suction and irrigation were accomplished with a nasogastric tube placed through the available 5-mm channel of the Triport. They used pediatric 5-mm robotic instruments, including graspers, an electrocautery hook, and a harmonic scalpel, and a 30-degree robotic camera with upward configuration. Barret et al. 16 reported their experience with LESS robot-assisted radical prostatectomy in a human, which replicated standard extraperitoneal laparoscopic prostatectomy. They used two 8-mm robotic ports and a 12-mm port for the robotic camera into a 4-cm umbilical incision. An additional 5-mm port was placed in the right lower abdomen and used for suction, counter traction, and pelvic drainage.
According to these initial reports, robotic single-site surgery can reduce technical difficulty, the suturing procedure, in particular, which is accepted as an alternative for LESS to resolve the challenges currently faced by surgeons. However, this type of surgery remains in the early stages and requires additional technical development and before generalization is possible.
We report a case of bilateral robotic single-site partial nephrectomy. In our primitive experience, a 30-degree robotic camera was used in the upward configuration to easily view both robotic arms. However, the camera and robotic instruments clashed, resulting in awkward operative manipulations. Therefore, we attempted to place the robotic instruments in a nonparallel position. We needed an additional assistant trocar to insert bull-dog clamps, suture material, and Hem-o-lok clips. To reduce ischemic time, we used continuous sutures with the sliding-clip technique for the renal parenchyma and capsule. 17 In terms of single-site devices, we used a homemade device of surgical gloves.18,19 Although device fabrication is time consuming, the device itself was developed at a low cost and provided a broad range of movement, as it was extremely flexible.
Although we completed the bilateral robotic single-site partial nephrectomy, our experience is still primitive. We need to further explore other surgical instruments and operative techniques, such as using a 30-degree camera with downward configuration and using pediatric 5-mm robotic instruments. Long-term follow-up is also needed to confirm that the cancer is controlled.
Conclusions
Our initial experience showed that bilateral robotic single-site partial nephrectomy is technically feasible. However, long-term follow-up and technical development are required to assess whether the cancer is controlled and to facilitate a minimally invasive surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.