
Abstract
Abstract
Advancements in minimally invasive surgical techniques and instruments for neonates have allowed even the most complex neonatal procedures to be endoscopically approached. In 1999, the first successful thoracoscopic repair of an esophageal atresia (EA) was performed in a 2-month-old infant. One year later, the first totally thoracoscopic repair of an atresia with distal fistula (tracheo-esophageal fistula [TEF]) was realized in a newborn. Over the ensuing 10 years, this technique was used and modified by a single surgeon in 49 consecutive patients. Overall, 43 patients with TEF and 6 with pure EA were repaired by using a thoracoscopic approach. An additional 3 patients with H-type TEF were also thoracoscopically treated. Weight ranged from 1.2 to 3.8 kg. Operative time ranged from 50 to 120 minutes. In fact, 48 out of 49 were successfully completed thoracoscopically. There were 2 patients with leaks that resolved with conservative management. Thirty percent of patients required at least one dilatation, but this number dropped to less than 10% in the second half of the series. There were no deaths and no recurrent fistula. Thoracoscopic TEF repair has proved to be an effective and safe technique. Evolution of the technique has resulted in fewer complications while avoiding the significant short- and long-term morbidity associated with thoracotomy in neonates.
Introduction
Recent advancements in technique and instrumentation in pediatric endoscopic surgery have allowed significantly more complex and delicate procedures to be performed, even in small premature neonates. Over the last 15 years, the number and breadth of minimally invasive surgical (MIS) procedures performed in infants has dramatically increased.1–3 However, one procedure, successful ligation of a TEF with repair of the EA, has remained relatively elusive. In 1999, a stepping stone was laid when a successful thoracoscopic repair of a pure EA was completed in a 2-month-old male. 4 In 2000, we reported on the first successful repair of an EA with TEF in a newborn by using a completely thoracoscopic approach 5 and 2 years, we later reported on the first significant series. 6 These milestones allowed for a more widespread adoption of these techniques so that numerous pediatric surgical units around the world are now performing minimally invasive TEF repair. This article will review the technique as well as the authors' personal experience.
Methods
With IRB approval, a retrospective review of all patients undergoing thoracoscopic repair of EA/TEF in newborns at a single institution, by a single surgeon, was performed.
Data collected included the newborn's age and weight at the time of the procedure, operative time, number of days of mechanical ventilation, duration of total hospitalization, the number of patients with leak and/or stricture formation, and the number of patients requiring esophageal dilation. In addition, other data including the number of patients who required fundoplication, imperforate anus repair, aortopexy, duodenal atresia repair, and cardiac operations were reviewed. All complications and mortality were also recorded.
Technique
All babies with TEF underwent repair in the first 36 hours of life. An additional 6 patients with pure EA underwent delayed repair after initial placement of a gastrosotomy tube. Tracheal intubation without an attempt at single-lung ventilation was used in all but the first 2 cases. A left mainstem intubation was used in these two. Lung collapse was achieved by CO2 insufflation at a low flow and low pressure (1 L/min, pressure of 4–8 mmHg). All patients, after the first 2 cases, were placed in a modified prone position with the right side elevated by 30°–45° (Fig. 1). This allowed for gravity to retract the lung anteriorly, thus giving excellent exposure to the posterior mediastinum, without the need for a lung retractor. This position also allowed adequate exposure for trocar placement. The first 2 patients were placed in a standard lateral decubitus position. The room should be set up as in Figure 2.

The patient is positioned in a modified prone position with the left side elevated at approximately 30°. This gives access to the area between the anterior and posterior axillary lines for port placement while exposing the posterior mediastinum.
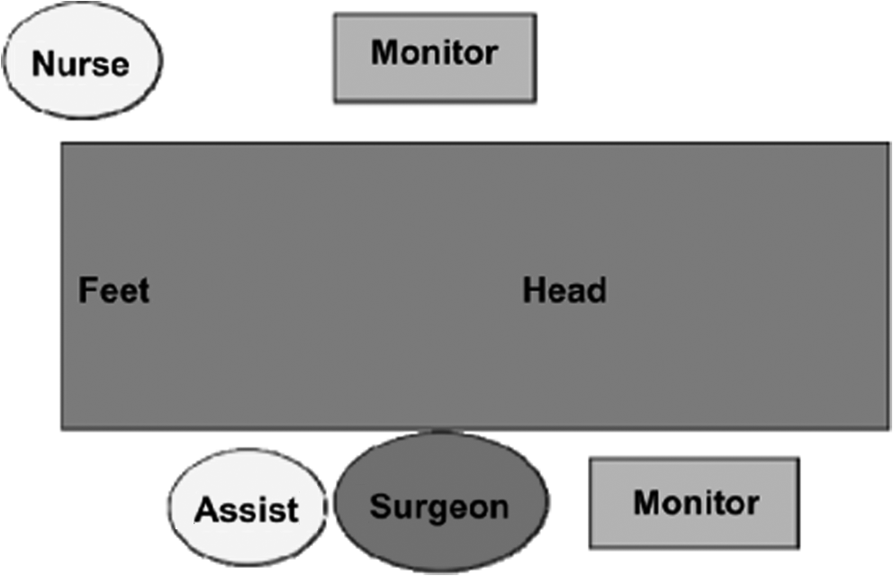
Standard room set-up for thoracoscopic tracheo-esophageal fistula (TEF) repair.
Three trocars were used for access to the thoracic cavity in all patients, and consisted of 2–3 mm and 1–5 mm port, or in slightly larger patients, a 1–3 mm, 1–4 mm, and 1–5 mm port. This depended on whether a 3 mm or 4 mm 30° telescope was used. The scope port was placed just posteriorly to the tip of the scapula, the right port in the axilla in the mid axillary line, and the left hand port was approximately in the fifth or sixth intercostal space behind the posterior axillary line (Fig. 3). As in the open technique, the initial step was to isolate and ligate the fistula. This was accomplished by the use of a 5 mm endoscopic clip in each case. Mobilization of the upper and lower segments was then performed. This was performed primarily with the use of a 3 mm hook cautery. On the upper pouch, the hook was used to separate the upper pouch from the surrounding adventitia. By hooking the tissues and then gently pulling on them while applying low-level cautery, the tissues are easily divided, and hemostasis is easily obtained. This technique is particularly useful in separating the esophagus from the membranous portion of the trachea. Blunt dissection well into the neck can also be achieved with the hook in the right hand, whereas a grasper in the left hand is used to pull the pouch inferiorly. Once adequate mobilization is obtained, then the anastomosis is completed with either 4-0 or 5-0 suture. In the first few cases, a braided permanent suture and extra-corporeal knots-tying techniques were used. With experience, the technique was changed to intra-corporeal suturing and an absorbable monofilament suture. A transanastomic tube and chest drain was used in all cases.

Port placement. Three mm ports are used for instruments, and the telescope and a single 5 mm port are used for introduction of the endoclip and suture.
Results
Forty-eight of 49 patients had their procedure successfully completed thoracoscopically. The mean age of the patients at the time of operation was 1 day, and the mean weight at operation was 2.4 kg, range 1.2–3.8 kg. The mean operative time (skin to skin) for the entire series was 75 minutes, range 50–120 minutes, and the mean days of mechanical ventilation were 2.4. A contrast study was obtained on postoperative day 3 in 1 patient, day 4 in 17 patients, and day 5 in 31 patients (Fig. 4). Two patients demonstrated a leak and were restudied at day 8 and 10, respectively. Both leaks spontaneously resolved. The mean duration of total hospitalization for patients with type 3 TEF was 14.7 days. Sixteen patients required at least one esophageal dilation, and 16 patients later required Nissen fundoplication for severe gastro-esophageal reflux.
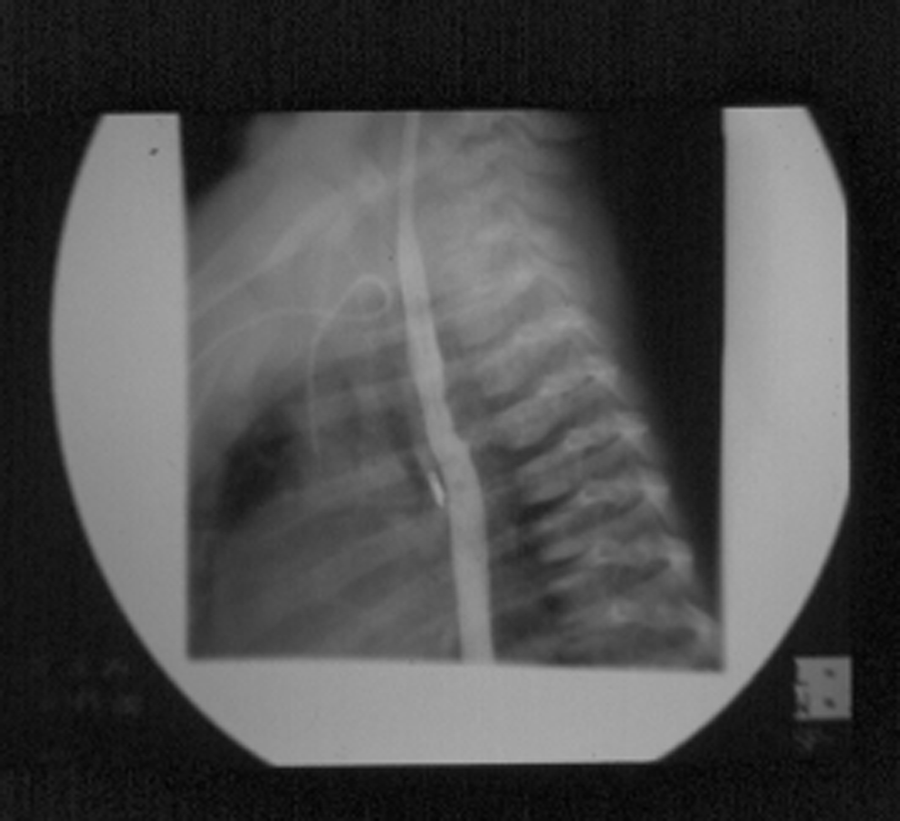
Contrast study on postoperative day number 4 showing a widely patent anastomosis and no leak.
Two patients were found to have a right aortic arch, and these were approached from the left chest. One of these patients had a tetralogy of Falot.
One patient underwent a staged repair. This was the patient weighing only 1.2 kg. The initial procedure consisted of only the thoracoscopic ligation of the fistula without division. A second procedure was performed when the patient weighed 2 kg to complete the anastomosis.
One patient underwent conversion from a thoracoscopic procedure to an open thoracotomy. In this case, the anastomosis had been successfully completed thoracoscopically. However, it was noted that the transanastomotic tube had not passed all the way into the stomach. Attempts to manipulate it further were unsuccessful, so the case was converted to rule out a false passage in the distal pouch. It turned out that the patient had a distal congenital stricture which was causing the obstruction. This was relatively easily dilated and traversed once the case was converted to open surgery.
A number of babies were found to have other significant anomalies. Four patients had high imperforate anus, 1 with a hydrometroculpos with ambiguous genitalia. In all cases after repair of the TEF, the patient was placed supine, and an exploratory laparoscopy and colostomy were performed. One baby had a duodenal atresia and underwent a laparoscopic duodenal atresia repair 2 days after the TEF repair. One patient underwent an aortopexy that was thoracoscopically done. Three patients required cardiac operations other than a ventricular or atrial septal defect repair.
Discussion
Thomas Gibson provides the first description of a baby with EA/TEF in 1703, 7 and Ladd and Leven performed the first successful staged repair of this lesion in 1939. 8 By 1965, a success rate of 80%–90% was achievable for repair of a type 3 TEF. 9
For the next 25 years, refinements in technique allowed improved survival even in relatively low-birth infants.10,11 However, there was still considerable morbidity associated with the operation with no major advances in surgical technique.
Recent advances in MIS in infants and children have allowed for a wide expansion of applications over the last decade. We first reported on our experience in infants less than 5 kg 1998 12 and recently reported on more than 600 cases in this weight and age range. 3 These studies clearly show that complex MIS procedures were not only possible but were associated with less morbidity than standard open techniques in neonates. In 2000, we performed the first thoracoscopic repair of a TEF with EA and since that time, it has been our standard approach in all cases. Previous studies have documented the long-term outcome of patients with EA and TEF, and the overall morbidity is significant, some related to the standard open thoracotomy.13–16 The benefits of performing a TEF by using minimally invasive techniques are obvious, but the technical hurdles are many, and a number of slight modifications have been made during the last decade to improve the technique and outcomes.
The greatest advantage to a thoracoscopic approach is avoiding a postero-lateral thoracotomy in a neonate. This has been shown to be associated with a high degree of scoliosis and shoulder girdle weakness later in development.17–20 Experience has also shown that the visualization and exposure obtained with an MIS approach is far superior to a standard thoracotomy. This actually makes identification and division of the fistula, as well as mobilization of the upper and lower pouches much easier. The only part of the procedure that is more technically demanding, compared with the standard open technique, is the suturing of the anastomosis. The small working space, often less than 2 square cms, requires advanced endoscopic and suturing skills, and these can be difficult skills to master. Once the surgeon has developed advanced endoscopic skills, then the surgical technique becomes quite straightforward.
Another obvious benefit is the improved cosmetic result, with most of these children having barely visible scars after 6–8 weeks (Fig. 5). Bianchi and others have advocated muscle sparing and or lateral thoracotomies, with various skin incisions to improve on these problems, but these incisions can be difficult to develop, offer more limited access, and still require spreading of the rib innerspace.21,22 Despite an improvement over a standard thoracotomy, there are still significant issues associated with these techniques and they may not eliminate the risk of scoliosis.

Skin incisions 1-month post-thoracoscopic TEF repair.
As already mentioned, a huge benefit of the thoracoscopic approach is the superior visualization of the anatomy and especially the fistula, and access to the upper and lower pouches. Since the fistula is visualized perpendicular to its insertion to the membranous trachea, the exact site for ligation can be easily identified; minimizing the residual pouch attached to the trachea. The use of the 5 mm titanium clips has proved to be simple and effective with no evidence of tracheal leak or recurrent fistula in this series. Others have reported migration of the clip into the trachea, but these reports are anecdotal. We find this approach to be the quickest way to gain control of and ligate the fistula, thus making the baby more stable for the anesthesiologist. However, suture ligation of the fistula is certainly an acceptable technique.
Another recognized advantage after the first case was the performance of the dissection and anastomosis in situ. Since the separation of the fistula and the upper pouch from the trachea was performed under direct magnified vision from a lateral approach, there was little manipulation or force applied to the trachea itself. This may help diminish the degree of tracheo-malacia that these children have postoperatively, 23 although 1 patient did require an aortopexy. In addition, the plane between the upper pouch and trachea was more obvious, thus making injury to the membranous wall of the trachea less likely.
One other possible advantage of performing the esophageal anastomosis thoracoscopically is that there may be less tension on the esophageal ends, thus allowing longer gaps to be brought together without tearing. This appeared to be the case in 1 patient with a trifurcation fistula and long gap, although he did develop an anastomotic stricture that required dilation. The 6 patients with long gap EA (greater than 3.5 vertebral bodies) were also brought together primarily without incident.
The major technical hurdle in this operation is the suturing of the anastomosis. The placement of the sutures and knot tying are technically demanding and initially relatively imprecise. In addition, as opposed to the open technique where the entire posterior row of sutures can be placed and then brought together to disperse the tension along multiple points during knot tying, this method places all the tension on one suture at a time. So far, this has not been a significant problem, but it could prove to be an issue in future cases. If necessary, then a number of sutures could be placed by using Roeder's knots so that the tension could be distributed over a number of sutures as they are gradually tightened.
To improve visualization during this portion of the operation, we have moved the scope port a bit more posteriorly, just behind the tip of the scapula, to give a more direct view of the esophageal ends. The left hand port has also been placed more posteriorly (closer to the spine as opposed to the mid axillary line) so that the right- and left-hand ports are at more of a 90° angle at the site of the anastomosis. This allows for more precise suturing. However, for this procedure to become more widely accepted, it may be necessary to develop a mechanical anastomotic device or self-knotting suture.
The rate of anastomotic narrowing requiring at least one dilatation in this series is 30% but was initially almost 50%, a figure much higher than our open experience. This may have been secondary to inadequate approximation of the mucosal ends or an insufficient opening being made in the upper pouch. We have modified the technique to eliminate both of these problems as well as switching to a monofilament absorbable suture. These changes seem to have resolved the problem with only 2 of the last 20 patients requiring dilatation.
In evaluating this current series, the patient characteristics are similar to other large reports in which open thoracotomy had been employed.20–24 Many of these reports are older series being published in the 1980s; but 2 more recent series were released in 1995, and another in 2001. In these reviews, the incidence of anastomotic leak ranged from 10% to 21%, much higher than the 4% in this series. The incidence of stricture development averaged 18% and is comparable to the overall group, although the incidence has dropped to 10% over the last 5 years.
The association of gastroesophageal reflux in patients with EA/TEF is well documented.
Two recent reviews have documented a 23% incidence of fundoplication in 125 patients with EA/TEF and a 100% fundoplication rate in another series of 21 patients.24,25
The incidence of patients and the percentage requiring fundoplication varied in other studies from 15% to 32.2% and is also comparable to the 32% in this series. Variations in the decision to proceed with fundoplication are likely due to surgeon preference in the management of GERD, and less likely to have anything to do with the technique of repair.
The technical and physiologic hurdles to accomplish a thoracoscopic repair are many, and they will require continued advances before this surgery becomes commonplace.
However, a recent survey performed by the author of members of IPEG and the pediatric list server yielded 105 responses (Rothenberg, State of the art of TEF repair in newborns, IPEG Congress, Hawaii 2010; Pers. Comm). This showed that more than 65 centers were attempting thoracoscopic repair of TEF and that half of these consider a thoracoscopic approach their first choice. Thus, there has been a fairly high adoption rate for this technically demanding procedure in a relatively short time. However, more work needs to be done to improve the ability to perform this complex reconstruction without a thoracotomy. This 10 year series lays further groundwork for supporting this technique in an attempt to minimize surgical morbidity in even the smallest pediatric patients.
Footnotes
Disclosure Statement
No competing financial interests exist.