
Abstract
Abstract
Background:
Much has been published on the role of mechanical bowel preparation (MBP) in open colorectal resection; however, the current study shows little evidence on the use of MBP prior to laparoscopic colorectal resections. In contrast to open procedures, MBP could influence the diameter of the bowel and thus the exposure of the surgical field in laparoscopy. This study aimed to assess the current practice of Dutch laparoscopic surgeons regarding MBP prior to colorectal resections.
Methods:
In January 2010, members of the Dutch Association for Endoscopic Surgery were invited to fill out an online questionnaire investigating whether MBP is prescribed prior to laparoscopic colorectal surgery, and which considerations are taken into account when choosing or omitting MBP.
Results:
The 82 (49%) returned questionnaires showed that 20% of respondents prescribe MBP prior to colonic resections, while 63% prescribe MBP prior to rectal resections. The most common reasons for giving MBP were the construction of a protective ileostoma (22%), improvement of the surgical field exposure (16%), and “other reasons” specified by free text (21%). The three most common reasons for conversion were inadequate surgical field exposure (88%), locally advanced tumor (68%), and adhesions (29%). Concerning the question which stages of the operation are influenced by MBP, 29% of respondents believed that the diameter of the small bowel was influenced by MBP, 29% indicated that the exposure of the surgical field was influenced by MBP, and 52% did not believe that any of the stages of the operation were influenced by MBP.
Conclusion:
The results of this questionnaire indicate that the implementation of MBP in laparoscopic colorectal surgery is based on individual preferences in the Netherlands. This emphasizes the need of new studies investigating the role of MBP on surgical field exposure in colorectal laparoscopic surgery.
Introduction
Thorough mechanical cleansing of the bowel has long been considered essential prior to colorectal operations.5–7 It was believed that an empty bowel would diminish the risk of anastomotic leakage and septic complications. However, during the last decade, several studies have been conducted investigating the use of mechanical bowel preparation (MBP). Most recent randomized controlled trials and meta-analyses uniformly conclude that there is no advantage of MBP prior to colorectal resections, finding equal or lower rates of anastomotic leakage and septic complications in patients without MBP compared with patients with preoperative MBP.8–17 However, these studies have not included patients operated by means of minimally invasive techniques, and therefore this conclusion cannot be extrapolated to laparoscopic surgery. Logically, one does not expect the effect of MBP on anastomotic leakage and other septic complications to be different between patients with a laparoscopic or open approach. However, the effect of bowel preparation on the volume of the bowel, and thus on exposure, could play an important role in the course of the laparoscopic intervention itself. Contradictory opinions are found in literature concerning this subject,12,16,18 and very few studies have investigated the role of MBP prior to laparoscopic interventions.19,20 To evaluate the current practice among Dutch laparoscopic gastrointestinal surgeons, we performed a questionnaire survey. The aim of this questionnaire was to investigate whether MBP is prescribed prior to laparoscopic colorectal surgery, and which considerations are taken into account when choosing or omitting MBP.
Materials and Methods
The Dutch Society for Endoscopic Surgery (NVEC, Nederlandse Vereniging Endscopische Chirurgie) was contacted and asked to participate in the study by sharing their members' contact information. In January 2010, members from the NVEC were invited by e-mail to fill out an online questionnaire on MBP prior to laparoscopic procedures. The target group of this study comprised surgeons performing laparoscopic colorectal surgery. The answers were automatically submitted online at the end of the questionnaire. After 2 weeks, the questionnaire was again sent to the members who had not yet responded.
The questionnaire consisted of 10 questions: 4 open and 6 multiple-choice questions. Of these 6 multiple-choice questions, 4 could be answered with “other” and specified with free text. Answers specified by free text were reviewed for validity (i.e., not just one letter or incoherent text).
Surgeons were asked whether they use MBP for laparoscopic procedures, what type of MBP they use, for what reason they use it, and what aspects of the procedure could be influenced by MBP. Because of the interest of this study in surgical field exposure, major reasons for conversion were asked, as well as the degree of Trendelenburg positioning of the patient.
Table 1 shows a summarized version of the questionnaire. Results are presented as percentages or medians with interquartile ranges.
Results
The NVEC has 247 members. Fifty-three surgeons not performing general surgery or gastrointestinal surgery were not contacted (mostly gynecologists, urologists, and thoracic surgeons). The online survey was sent to the remaining 194 members. Thirty-five members did not receive it due to incorrect e-mail addresses (defined as e-mails that could not be delivered due to errors in the address or nonexisting addresses), or responded that they did not perform gastrointestinal surgery. Of the 169 laparoscopic surgeons who received the online survey, only 82 responded (49%). In 84.1% of respondents, lower gastrointestinal surgery was included in their field of interest, while 15.9% indicated that their field of interest was upper gastrointestinal surgery. The median quantity of colorectal resections performed per month was 5.3–7
Twenty percent of respondents declared to give MBP prior to laparoscopic colorectal resections, while 63% of respondents declared to give MBP prior to laparoscopic rectal resections. The distribution of the different types of MBP can be found in Figures 1 and 2. The median percentage Trendelenburg positioning of the patient was 30 degrees (26.5–42.5 degrees).
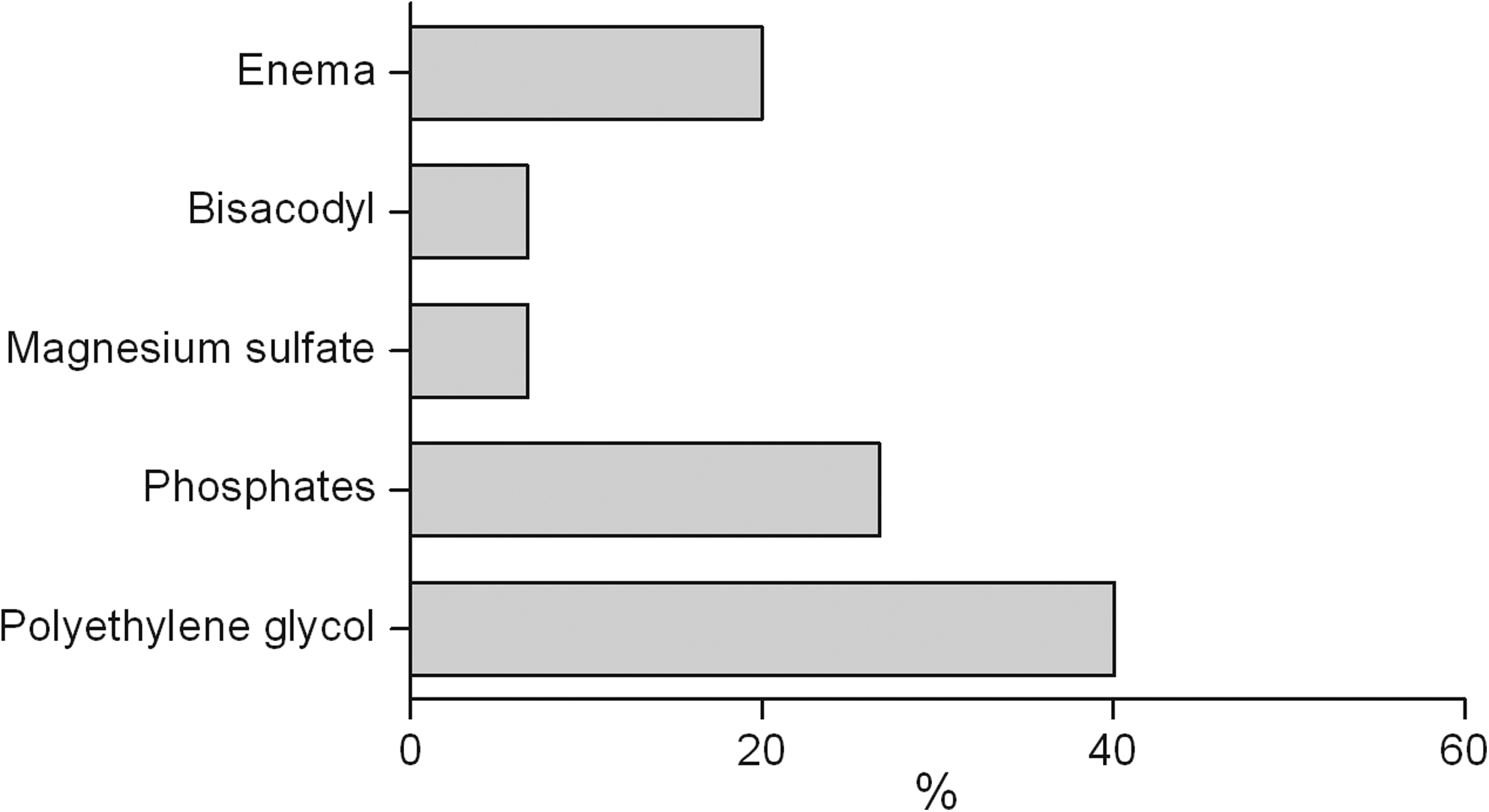
Mechanical bowel preparation (MBP) used prior to colonic resection.
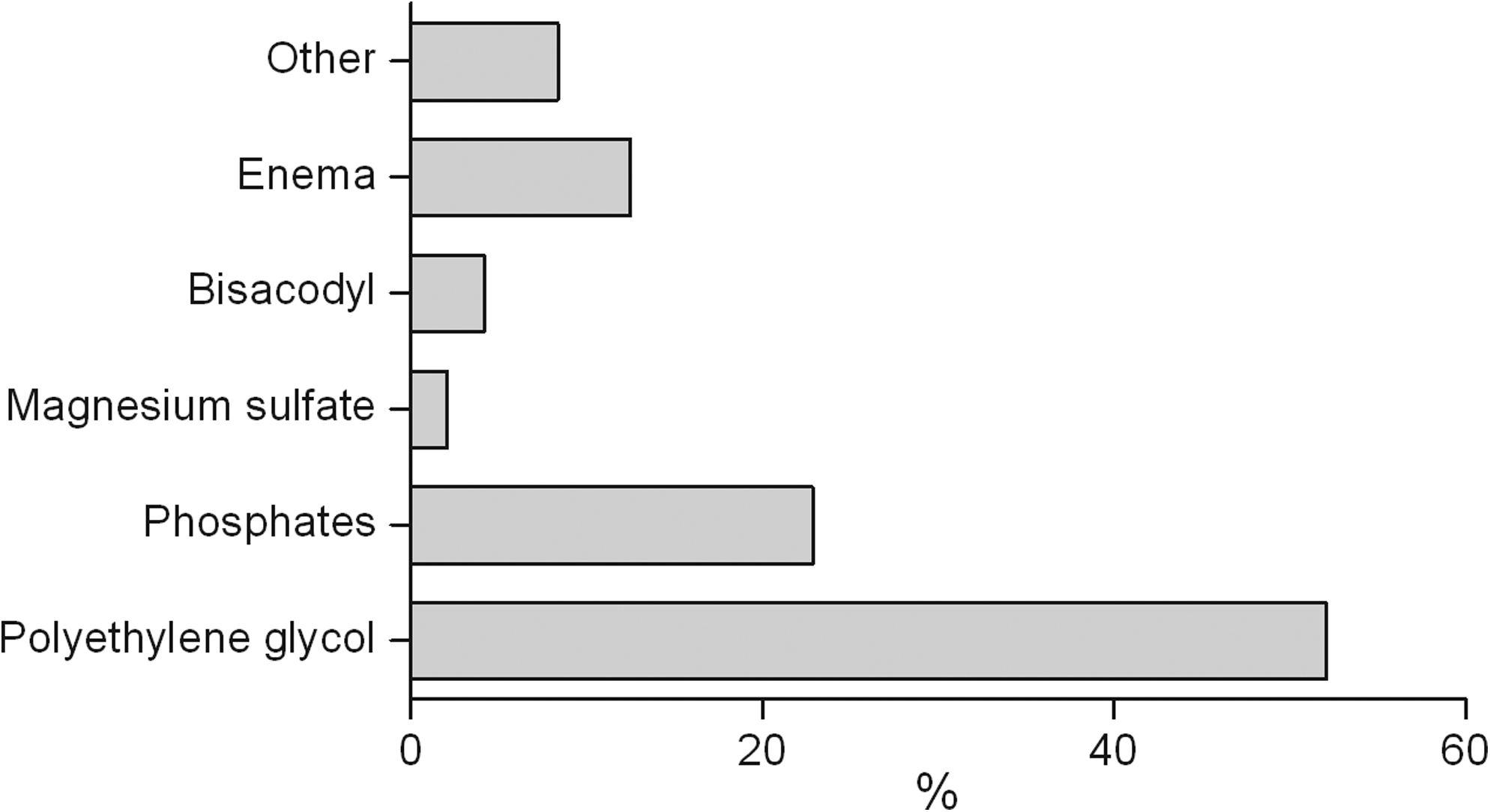
MBP used prior to rectal resection.
Of the 63% of respondents giving MBP, the most common reasons for giving MBP are shown in Figure 3. The construction of a protective ileostoma, not intending to leave a “filled” colon, was the most frequent answer (22%), followed by “other reasons” and free text (21%), and improvement of the surgical field exposure (16%). The two most frequent text when choosing “other reasons” was (1) better handling of the bowel when it is empty and (2) easier introduction of the stapler. The three most common reasons for conversion were inadequate surgical field exposure (88%), locally advanced tumor (68%), and adhesions (29%) (Fig. 4). Concerning the question which stages of the operation are influenced by MBP, 52% of respondents believed that MBP does not influence any stage of the operation. Twenty-nine percent of respondents thought that the diameter of the small bowel was influenced by MBP, and 29% indicated that the exposure of the surgical field was influenced by MBP (Fig. 5).
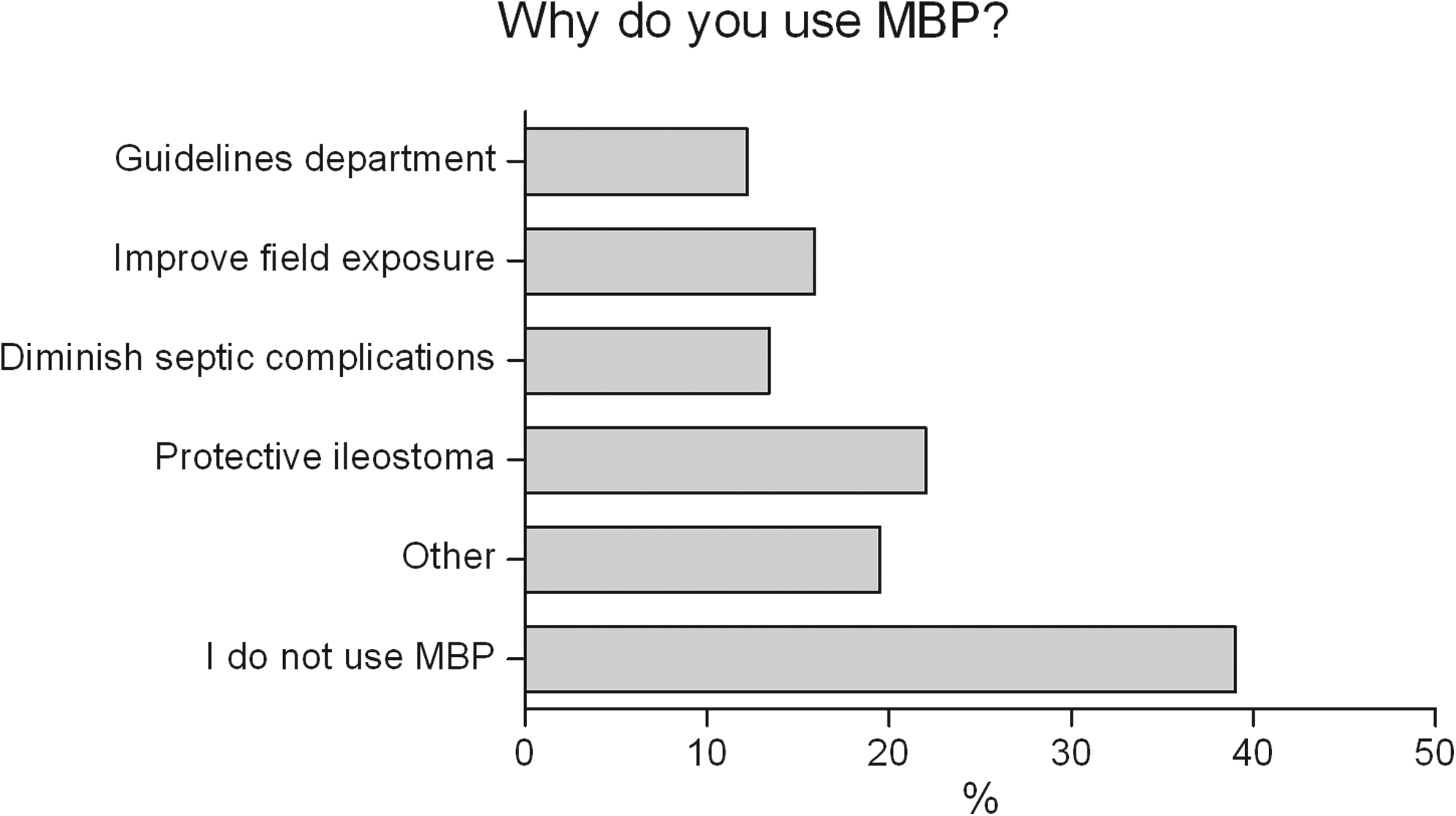
Reasons for giving MBP.
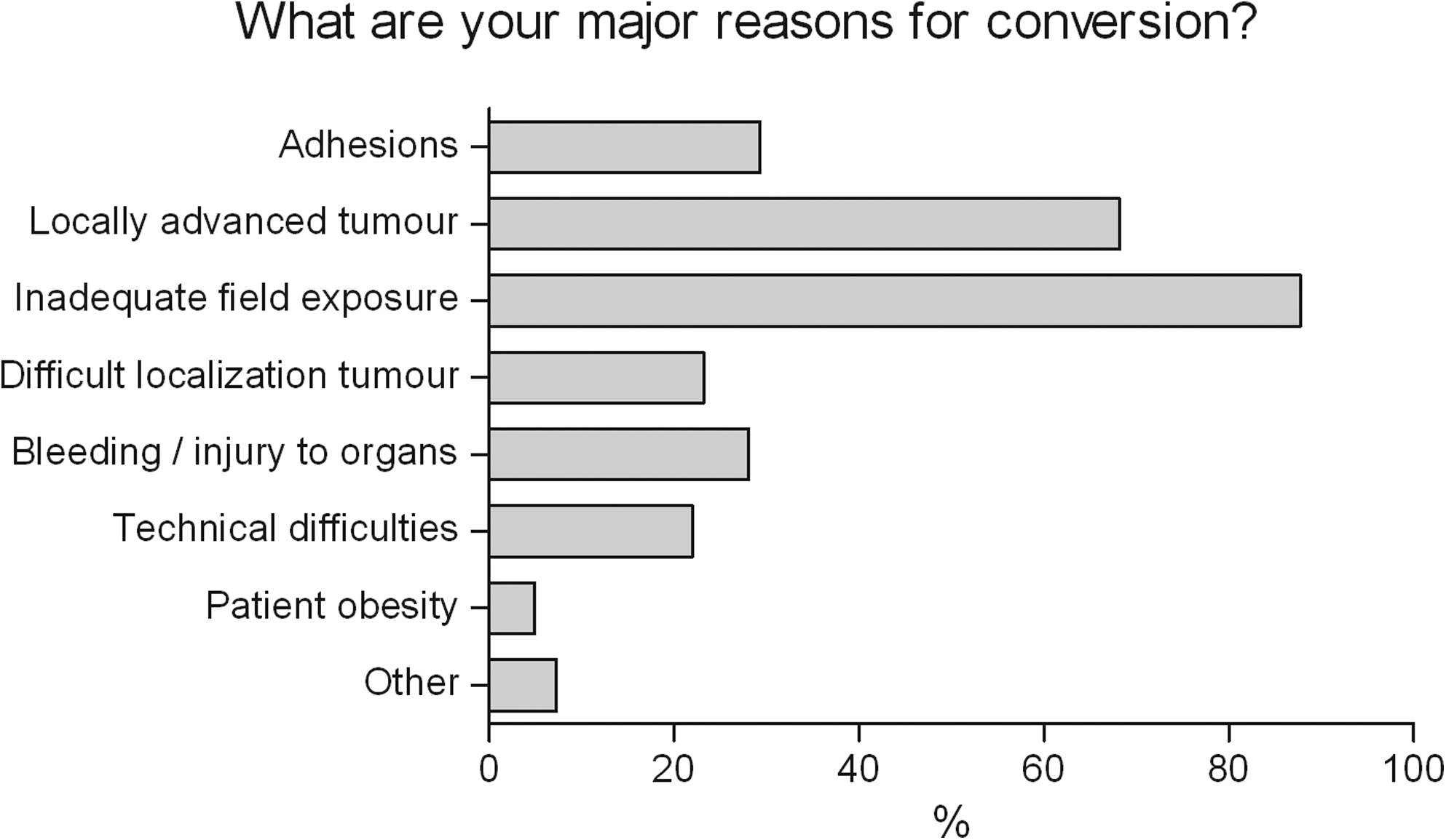
Reasons for conversion from laparoscopic to open approach.
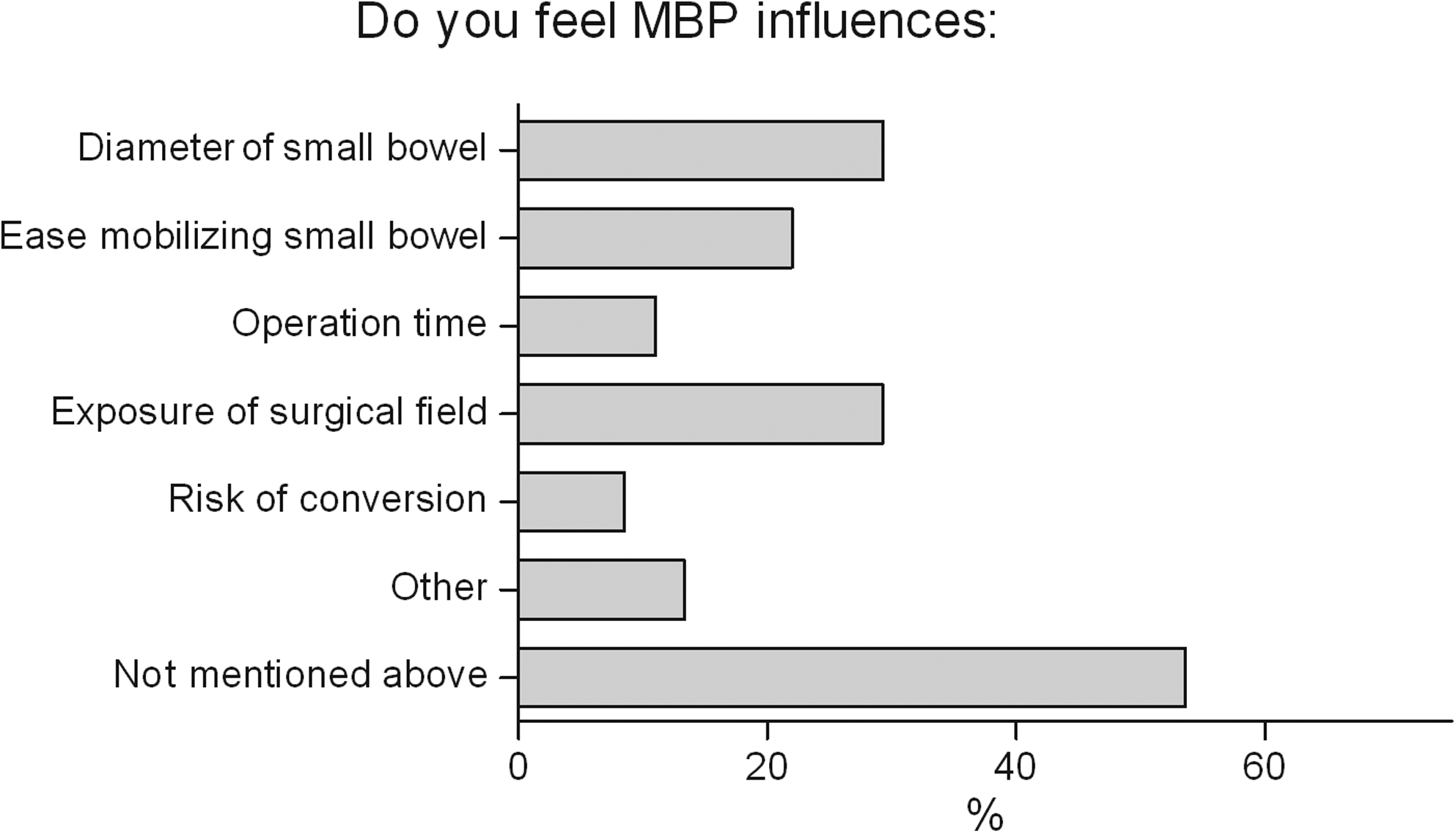
Influence of MBP on different stages of the operation.
Discussion
Due to strong evidence that MBP does not lower the risk of anastomotic leakage and other septic complications in elective colorectal surgery,8–17 its standardized use has been abandoned in many centers. However, no studies regarding MBP have yet been conducted focusing on patients operated by means of minimally invasive techniques. In the Netherlands, nowadays, a significant part of colorectal resections are performed through laparoscopy, and the improved short-term results (less postoperative pain, earlier recovery of bowel function, less blood loss, and shorter hospital stay) and similar disease-free survival rates have resulted in the important increase of laparoscopic procedures.1–4
In our opinion the results of studies on MBP and infectious complications can also be applied to laparoscopic surgery; however, the effect of MBP on the volume of the bowel and its competition with the insufflated CO2 influencing exposure could play an important role in the course of the laparoscopic intervention itself. Evidence-based guidelines concerning this issue are lacking, and contradictory opinions are found in literature concerning this subject. Guenaga et al. 12 mention in their Cochrane review that it has been argued that it is easier to perform laparoscopic surgery if the bowel contains solid matter in order to use gravity to obtain better overview. Slim et al. 16 state in a meta-analysis that MBP usually results in dilated bowel which could hamper laparoscopic vision and make mobilization of the intestines more difficult. Cheung et al. 18 have described their results of a questionnaire on the technique of laparoscopic total mesorectal excision. They find that most surgeons apply MBP routinely for different reasons, and that reduction of intestinal volume to facilitate laparoscopic exposure appears to be a specific incentive.
Two studies in literature evaluated the effect of MBP on exposure in gynecologic laparoscopy. In the first study, performed by Muzii et al., 19 patients were randomized between preoperative MBP (90 mL sodium phosphate) and no MBP; the endpoint was the appropriateness of the surgical field as judged by the surgeon on a scale going from poor to excellent in five steps. No advantage of MBP on the evaluation of the surgical field could be demonstrated. 19 Another randomized trial, performed by Yang et al., 21 divided patients into two groups. The first group received MBP through oral sodium phosphate solution; the second group received only a sodium phosphate enema. Assessment of the quality of the surgical field and bowel characteristics was performed using a surgeon questionnaire with Likert and visual analog scales. No significant differences were observed between the two groups in evaluation of the surgical field, bowel handling, degree of bowel preparation, or surgical difficulty. 21
The results of this questionnaire show that bowel preparation is still frequently used in laparoscopic colorectal procedures in the Netherlands, mostly in rectal resection. Sixteen percent of respondents prescribe MBP prior to surgery in order to improve surgical field exposure; on the other hand, inadequate surgical field exposure was by far the most common reason for conversion (88%). Almost a third of the respondents felt that MBP might influence the diameter of the small bowel and the exposure. This can be placed in either a positive or a negative perspective since some feel that MBP results in an emptied bowel and some feel that MBP results in a bowel filled with liquid or gas bowel contents. 22
The most important limitation of this questionnaire is the response rate of 49%. A low response rate to questionnaires is a well-known problem, and to make the chances of response as high as possible we sent an online questionnaire by e-mail, made it as short as possible (10 questions), and with automatic sending of the results at the end of the questionnaire. Another limitation is the fact that ideally all Dutch surgeons performing laparoscopic gastrointestinal procedures should have been contacted, however from a practical point of view that is not feasible. We have chosen to send this questionnaire through the Dutch Association of Endoscopic Surgery since that provided us an e-mail list of Dutch surgeons with particular interest for laparoscopic surgery.
A different questionnaire was performed by Wells et al., 23 amongst 110 members of the Society of Gynecologic Oncologists of Canada to assess the practice pattern and beliefs on MBP. The results show that half of the respondents routinely use MBP for gynecologic oncologic surgery (laparotomy and laparoscopy). The most common reasons for using MBP were to decrease the risk of anastomotic leak and to improve visualization.
To present, no evidence exists on the role of MBP on the diameter of the bowel and exposure in colorectal laparoscopy. To achieve optimal exposure in laparoscopic colorectal surgery, the small bowel has to be mobilized cranially. Several aspects can influence the ease of mobilizing the small bowel: the degree of muscle relaxation and Trendelenburg position, the thickness of the omentum and mesocolon of the small bowel (related to body mass index), and the diameter of the small bowel. The first aspect is in the hands of both surgeon and anesthetist; the second aspect is patient dependent and cannot be influenced. Concerning the diameter and contents of the small bowel and the ease in which it can be mobilized, only little is known. Whether a completely emptied bowel is preferable over normal stool contents in order to use gravity remains an unanswered question until now. Further, it is questionable whether MBP can achieve a complete emptied bowel at all, or whether it will result in a more voluminous small bowel due to inadequate bowel cleansing and liquid or gas bowel contents. 22 The latter could also be influenced by the type of MBP being administrated and patient compliance.
The scarce quantity of studies regarding the subject of MBP in laparoscopy indicates the following: (1) Questionnaires regarding MBP indicate that a number of laparoscopic surgeons use MBP with the aim to improve surgical field exposure (Wells et al. 23 ). (2) Randomized studies on MBP in gynecologic laparoscopy seem to conclude that there is no amelioration of surgical field exposure with MBP. The difficulty in these studies is the outcome measure, which is the evaluation of the surgical field using a surgeon questionnaire.19,21
In conclusion, the results of this questionnaire show that the indication of MBP in laparoscopic colorectal surgery is undefined in the Netherlands. A review of literature shows that the influence of MBP on diameter of the bowel and thus laparoscopic vision is not clear. Studies investigating the role of MBP on intestinal volume and surgical field exposure in colorectal laparoscopic surgery are necessary.
Footnotes
Disclosure Statement
No competing financial interests exist.