
Abstract
Abstract
Purpose:
Rectal neuroendocrine (carcinoid) tumors smaller than 1 cm without lymph node metastasis and confined within the submucosal layer (stage T1aN0) can be treated using endoscopic resection. The present study was aimed to assess the safety and efficacy of endoscopic submucosal dissection (ESD) for T1aN0 carcinoid tumors.
Patients and Methods:
A total of 35 consecutive patients with a T1aN0 rectal carcinoid tumor were enrolled between March 2007 and December 2009. The study evaluated the histologically complete resection rate, procedure time, complications, and short-term oncological outcomes.
Results:
The mean patient age was 49.0 years (range, 32–74 years), and there were 25 men and 10 women. The mean procedure time was 35.6 minutes (range, 7–82 minutes). All neoplasms were removed in one piece, and the histologically complete resection rate was 74.3% (26 cases including 5 cases showing no residual tumor). No post-ESD bleeding was observed. Abdominal computed tomography scans showed a perforation in 1 patient only, but that perforation was not associated with any peritonitis symptoms, and the patient was discharged on postprocedure day 3. One patient underwent radical surgery after ESD because of angiolymphatic invasion and positive resection margins, and the final pathology revealed no residual tumor or lymph node metastasis. No patient showed local recurrence or distant metastasis during a median follow-up of 25 months (range, 12–43 months).
Conclusions:
ESD is feasible and safe for treating T1aN0 rectal carcinoid tumors. Further studies are required to accurately determine long-term oncological outcomes.
Introduction
T0, no evidence of primary tumor; T1, tumor invades lamina propria or submucosa and size ≤2 cm in greatest dimension; T1a, tumor size <1 cm in greatest dimension; T1b, tumor size 1–2 cm in greatest dimension; T2, tumor invades muscularis propria or size >2 cm with invasion of lamina propria or submucosa; T3, tumor invades through the muscularis propria into the subserosa or into nonperitonealized pericolic or perirectal tissues; T4, tumor invades peritoneum or other organs; N0, no regional lymph node metastasis; N1, regional lymph node metastasis; M0, no distant metastasis; M1, distant metastasis.
Endoscopic submucosal dissection (ESD) was developed to allow dissection directly along the submucosal layer for gastric epithelial neoplasms and was recently introduced for en bloc resection of colorectal neoplasms. 8 Although ESD has been reported to improve the rate of successful en bloc resection in early-stage rectal carcinoids, it is not free of complications.9,10
The present study evaluated the safety and efficacy of ESD when used to treat T1aN0 carcinoid tumors. The study examined a range of parameters, including procedure time, complications, histologically complete resection rate, local recurrence, and distant metastasis.
Materials and Methods
Patients
Between March 2007 and December 2009, 35 consecutive patients with a rectal carcinoid tumor underwent ESD at the National Cancer Center in Korea (Goyang, Korea). The study only included submucosal tumors that were <1 cm in diameter and that had been shown to be carcinoid tumors in pathology tests. Excluded were patients with suspected lymph node or distant metastases according to endoscopic ultrasound, computed tomography (CT), or magnetic resonance imaging. The study was approved by the Institutional Review Board of the National Cancer Center, which deemed that informed consent was not required, because the study was retrospective.
Endoscopy technique
ESD was carried out using a single-channel colonoscope (CF-H260AL; Olympus Optical Co., Tokyo, Japan) and a high-frequency generator with an automatically controlled system (Erbotom ICC200 or VIO 300D; ERBE, Tuebingen, Germany). A transparent cap was attached to the tip of the endoscope to provide a constant view and to give countertraction for submucosal dissection. To make a submucosal cushion, a glycerol mixture solution (10% glycerin and 5% fructose in 0.9% saline [CEROL®] with small amount of indigo carmine and epinephrine) was injected into the submucosal layer as many times as required until the target mucosa with the lesion was sufficiently raised from the muscle layer. The mucosa was then incised with a needle knife or a flex knife (KD-630L; Olympus Optical Co.) and the submucosal connective tissue just beneath the lesion was dissected using a flex knife alone or in combination with a hook knife (KD-620LR; Olympus Optical Co.) (Fig. 1). To facilitate visualization of the dissecting tissue plane or detachment from the rectal wall, the patient's position was changed. Procedure time was defined as the time interval between tumor visualization and completion of resection.
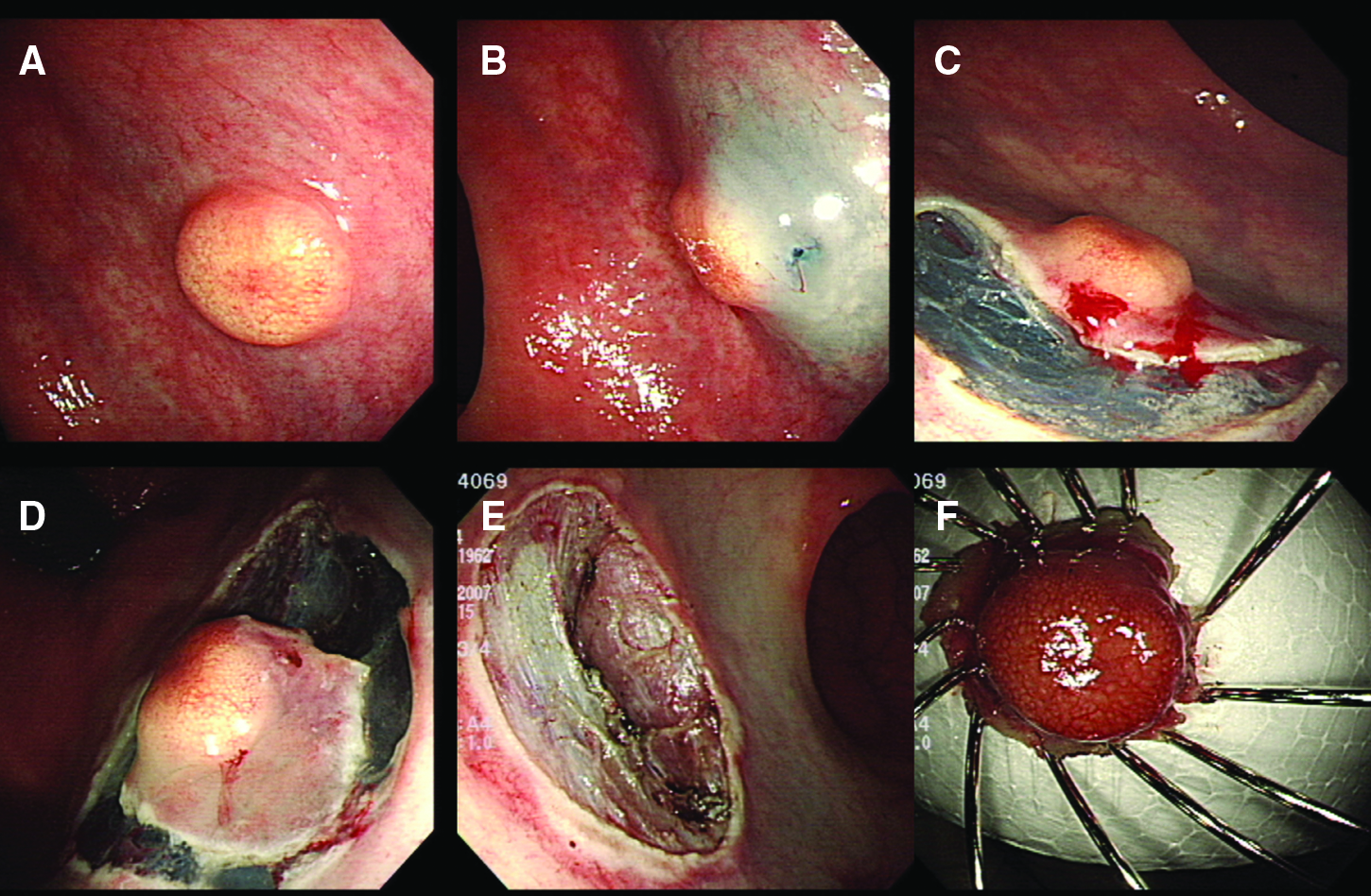
Endoscopic submucosal dissection of a rectal carcinoid tumor.
Evaluation of complete resection and complications
Endoscopically complete resection was defined as a one-piece resection without gross remnant tumor. All resected specimens were stained with hematoxylin and eosin to confirm the histology diagnosis. A histologically complete resection was defined as when the lateral and deep margins of a specimen were free of tumor tissue. Tumor size, depth of invasion, and angiolymphatic involvement were assessed.
Procedure-related bleeding after ESD was defined as bleeding that required transfusion or hemostatic intervention or as bleeding that caused the hemoglobin level to fall by 2 g/dL. Perforation was classified as endoscopically observed rectal wall penetration, or a perforation detected after endoscopy according to abdominal plain X-ray or CT; a patient with suspicious abdominal symptoms took an abdominal X-ray and CT was indicated when plain X-rays were inconclusive.
Follow-up
All patients, except those who had undergone radical surgery, underwent a sigmoidoscopy at 3 and 12 months postprocedure and annually thereafter. Patients with an endoscopically complete resection but histologically positive resection margin were followed up more frequently, with sigmoidoscopy every 3 months postprocedure for the first year. Biopsy of the postprocedure scar was performed for any suspected recurrent or remnant tumor. Patients underwent abdominopelvic CT scans and chest X-rays every year to monitor for any metastasis.
Results
Patient characteristics
The mean patient age was 49 years (range, 32–74 years), and the male-to-female ratio was 5:2 (Table 2). Thirty of the 35 patients underwent ESD following a screening colonoscopy and had no specific abdominal symptoms. Of the remaining 5 patients, 1 had a positive fecal occult blood test result, 1 had epigastric pain, and 3 had anal bleeding. Pathology tests resulted in 15 patients being diagnosed with a carcinoid tumor before ESD. The remaining 20 patients had suspected carcinoid tumors based on endoscopic features and were referred to our clinic without histological confirmation. Five patients had another malignancy; 2 had breast cancer (stage IIB and unknown stage), and 1 each had a stage I thyroid cancer, a stage III common bile duct cancer, and a stage II intrahepatic cholangiocarcinoma. The last 2 patients experienced their primary cancer recurrence in 17 and 14 months, respectively, and were excluded from the follow-up analysis.
ESD outcomes
The distance of the tumor from the anal verge was 7.1±1.8 cm (mean±standard deviation) (Table 3). The mean endoscopic and pathologic tumor diameters were 5.4±1.6 mm and 4.7±2.0 mm, respectively. No carcinoid tumors invaded beyond the submucosal layer, and all tumors were removed in en bloc resection (100%). The histologically complete resection rate was 74.3% (26 cases including 5 cases showing no residual tumor); of the nine specimens with tumor-involved resection margins, the deep margin was involved in six, the lateral in two, and both in one specimen. The mean procedure time was 35.6±16.5 minutes (range, 7–82 minutes), and the mean length of stay in hospital was 3.0±0.7 days (range, 2–5 days).
Complications
No post-ESD bleeding was observed. The abdominal CT of 1 patient showed a pneumoperitoneum and pneumoretroperitoneum on postprocedure day 1. However, that patient showed no symptoms or signs of peritonitis and was discharged on postprocedure day 3 without the need for further endoscopic or surgical intervention.
Follow-up and rescue treatment
One patient underwent radical surgery after ESD because of angiolymphatic invasion and positive resection margins. Pathology tests on the specimen revealed that there was no residual tumor or lymph node metastasis. The other 8 patients with a histologically positive resection margin were considered to have had an endoscopically complete resection and were monitored with postprocedure sigmoidoscopy and biopsy (if required).
The median follow-up period was 25 months (range, 12–43) in 26 patients who did not have other intra-abdominal malignancies and who came to the clinic regularly. None of those 26 patients showed local recurrence or distant metastasis (Fig. 2).
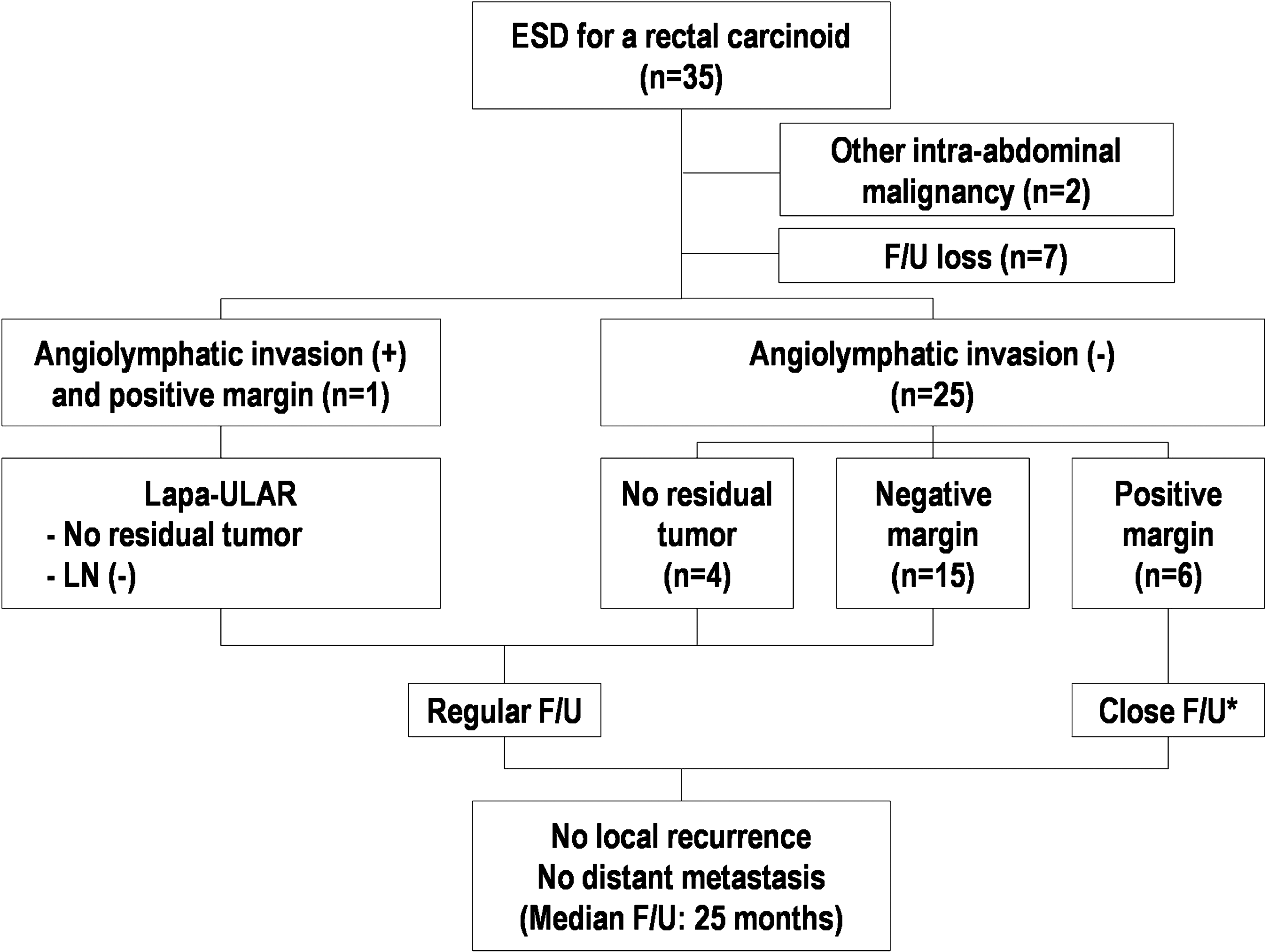
A flow chart detailing the follow-up events. ESD, endoscopic submucosal dissection; Lapa-ULAR, laparoscopic ultra-low anterior resection; LN, lymph node involvement; F/U, follow-up. *Sigmoidoscopy every 3 months.
Discussion
This study evaluated the safety and efficacy of ESD for the treatment of T1aN0 rectal carcinoid tumors. Although carcinoid tumors have been widely thought of as benign, Modlin et al. found that 12.9% of all patients with carcinoids had evident metastasis at the time of diagnosis. 11 In addition, Soga found that metastasis rates were similar for gastrointestinal carcinomas and gastrointestinal carcinoids. 2 The American Joint Committee on Cancer recently added a staging system for neuroendocrine tumors (gastric, small bowel, colonic, rectal, and ampulla of Vater carcinoid tumors) in the seventh edition. 1
Rectal carcinoids have a better prognosis than carcinoids at other gastrointestinal sites, and the all-site 5-year survival rate for submucosal carcinoids is 87% when compared with 98.3% for carcinoids in the rectum after curative resection.2,3 The detection of rectal carcinoids has increased with the greater awareness by clinicians and pathologists and with the more sophisticated diagnostic tools, and more than half of all carcinoid tumors in the rectum are incidentally diagnosed at an early stage. 12
In the present study, 85.7% of carcinoids were detected in asymptomatic patients in screening colonoscopies. This relatively high detection rate reflects that the present study only included patients with rectal carcinoids smaller than 1 cm. The mean patient age of 49 years was within the range of 48–52 years mentioned in the Surveillance, Epidemiology and End Results (SEER) data 11 and is similar to the 51.3 years stated in a Japanese study. 2
The preponderance of males in the present study population was similar to that reported by Soga, 2 but differed from the SEER data, which reported a ratio of 1.05–1.11. These differences may reflect differences in the ethnicity of the patients in the respective studies.
The present study found that 5 (14.3%) of the 35 patients had another malignancy. Coexisting noncarcinoid tumors and multicentricity are features of patients with carcinoid tumors, which indicates the requirement for a meticulous evaluation during diagnosis and treatment. 3 The present findings are consistent with the SEER data (1992–1999) showing that 13.1% of rectal carcinoids were associated with other (noncarcinoid) neoplasms.
The present study only included carcinoid tumors less than 1 cm. Regardless of size, if the neoplasm had high-risk features of evident muscular invasion or suspected lymph node involvement, radical surgery (low anterior resection with total mesorectal excision or abdomino-perineal resection) was recommended. Previous studies have shown that T1aN0 rectal carcinoid tumors <1 cm in size and located within the submucosa without metastasis can be managed using local endoscopic or transanal resection. 13 As for rectal carcinoids of T1bN0 (the same as T1aN0 except sized between 1 and 2 cm), there is no consensus in the literature concerning the appropriate therapy. 14 Previous reports have presented different size indications for rectal carcinoid endoscopic resection: ≤10 mm (Ishii et al. 15 and Yamaguchi et al. 10 ), <16 mm (Park et al. 16 ), and <20 mm (Kwaan et al. 14 ).
The procedure time is longer for ESD than EMR because of the greater technical complexity.9,16,17 However, several studies have shown encouraging results after ESD for rectal carcinoid tumors (Table 4). In our study, the mean procedure time was 35.6 minutes, which was longer than for other recent studies but was tolerable for patients. We found that the ESD procedure took longer in patients who had a history of biopsy before the ESD (27.5 vs. 45.8 minutes, p=0.001). However, the histologically complete resection rate was not affected by a previous biopsy (70% vs. 80%, p=0.700). Previous studies have discussed the effect of biopsy on the nonlifting sign in submucosal invasive colorectal carcinoma due to mechanical stimulation and submucosal fibrosis. 18 Carcinoid tumors invade the submucosal layer and behave like submucosal colorectal carcinomas endoscopically; therefore, a previous biopsy may result in submucosal fibrosis and prolong the procedure.
Only 1 present patient experienced a perforation, and it was subclinical and no post-ESD bleeding was detected. Previous studies on patients with rectal carcinoids reported a 0%–9% bleeding rate and a 0%–5% perforation rate (Table 4).10,14–17 However, all of those patients were treated using endoscopic hemostasis or metal clipping and none required surgical intervention.
As carcinoid tumor is a malignant disease, our chief concern was complete resection of the tumor. The histologically complete resection rate was 74.3% (26/35), which is lower than our rate for endoscopic submucosal resection with cap aspiration technique (85.7% [36/42]). 19 However, the current ESD pathologically complete resection rate was better than the rate for EMR reported in other studies that compared these two methods. Lee et al. 17 and Park et al. 16 showed superior outcomes for ESD compared with EMR (histologically complete resection rates: 82.6% vs. 64.3%, and 90.3% vs. 71.0%, respectively). These findings indicate that ESD results in a higher en bloc resection rate, but that other methods can be applied in selected cases with good results.
In the present study, the follow-up strategy for patients with an endoscopically complete resection without other risk factors was close follow-up with no rescue surgery. This strategy is similar to that reported in other studies which showed no local recurrence or metastasis.14,16,17 To date, such studies have involved a small number of patients and short follow-up periods, and therefore, we cannot yet conclude whether endoscopically complete resection can replace histologically complete resection as a criterion for safety.
In conclusion, ESD was found to be safe and feasible for treating T1aN0 rectal carcinoid tumors. However, firm conclusions regarding oncological outcomes after ESD require large-scale studies with long-term follow-ups.
Footnotes
Acknowledgment
This work was supported by a National Cancer Center Research Grant (Grant NCC-0910520).
Disclosure Statement
No competing financial interests exist.