
Abstract
Abstract
Background/Purpose:
Congenital duodenal obstruction (CDO) is traditionally managed via laparotomy. Laparoscopy has been suggested as an alternative; however, few series have described this in neonatal CDO. We report our series of CDO repaired laparoscopically compared to laparotomy.
Methods:
After Institutional Review Board approval, a retrospective review was performed on patients with CDO who were presented between October 2001 and July 2010. Duodenal obstruction was managed laparoscopically (LAP) or via an open approach (OPEN) based on the surgeon's choice. Data were analyzed by intention to treat and were expressed as median±range.
Results:
Twenty-two neonates underwent laparoscopy and 36 had a traditional laparotomy for management of CDO. Associated diseases included Down's syndrome (n=26), congenital heart disease (n=29), and malrotation (n=16). Median age was 4 days (range: 1–310) for LAP and 3 days (range: 0–166) for OPEN (P=.04). Gestational age and weight were similar (P=.335 and .378). The CDO was due to atresia (n=32), web (n=16), and annular pancreas (n=10). Median operative time for LAP was 116 minutes with a range of 73–164 while median time for OPEN was 103 minutes with a range of 71–220 (P=.013). There was no difference in time to full feedings (P=.69) or postoperative length of stay (P=.682). Ventilation time was 2 days with a range of 0–149 for LAP and ventilation time was 4 days with a range of 0–9 for OPEN (P=.02). Complication rates between the groups were similar.
Conclusion:
In the hands of a skilled surgeon, laparoscopy appears to be a safe and effective technique in managing CDO in neonates. In this retrospective study, laparoscopic management of CDO appeared to allow a shorter postoperative ventilator requirement with similar length of stay and time to full feedings. Operative time was slightly longer in the LAP group. Formal prospective trials are recommended to validate these findings.
Introduction
Laparoscopic repair of CDO has been reported, but it is limited to a few case reports and small case series.7–10 The first reported laparoscopic repair of a duodenal atresia was by Bax et al. in 2001. 7 In 2002, Gluer et al. 8 described the first case of annular pancreas and malrotation repaired laparoscopically. They performed a duodenoduodenostomy and a Ladd's procedure successfully in a 3450 g newborn. 8 Since these case reports, only a few small series of laparoscopic duodenoduodenostomy for duodenal obstruction have been reported.9,11
The aim of this report is to review our series of patients who underwent laparoscopic exploration for CDO and to compare their outcomes with patients who were treated via an open technique.
Materials and Methods
After obtaining Institutional Review Board approval, we reviewed charts of pediatric patients who were presented to Children's Healthcare of Atlanta at Egleston with duodenal obstruction between October 2001 and July 2010. During the period of time studied, cases of duodenal obstruction were either explored laparoscopically or via an open technique based on the surgeon's choice. Data were analyzed based on intention to treat and were expressed as median±range.
Laparoscopic technique
Through an umbilical stab incision, a Veress needle was used to insufflate the abdomen to a pressure of 12 mmHg. The 3-mm camera port was placed in the umbilicus, and two additional 3-mm ports were placed on the right side of the abdomen (Fig. 1). The camera is then moved to the mid-clavicular port site. Occasionally, a fourth, left-sided port was placed to facilitate retraction. A transabdominal stay suture was placed through the falciform ligament for retraction. Similar stay sutures were placed in the proximal and distal duodenum at the level of obstruction, and a proximal duodenotomy was made. If a web was present, it was excised and a duodenoplasty was performed with interrupted sutures. Otherwise, a duodenoduodenostomy was performed. The backwall was closed with running suture and the anterior wall was closed with interrupted sutures. In all cases, the anastomosis was checked by insufflating the stomach with air. The large and small bowels were checked for pathology including additional webs or atresias. If malrotation was present, then a Ladd's procedure was performed.
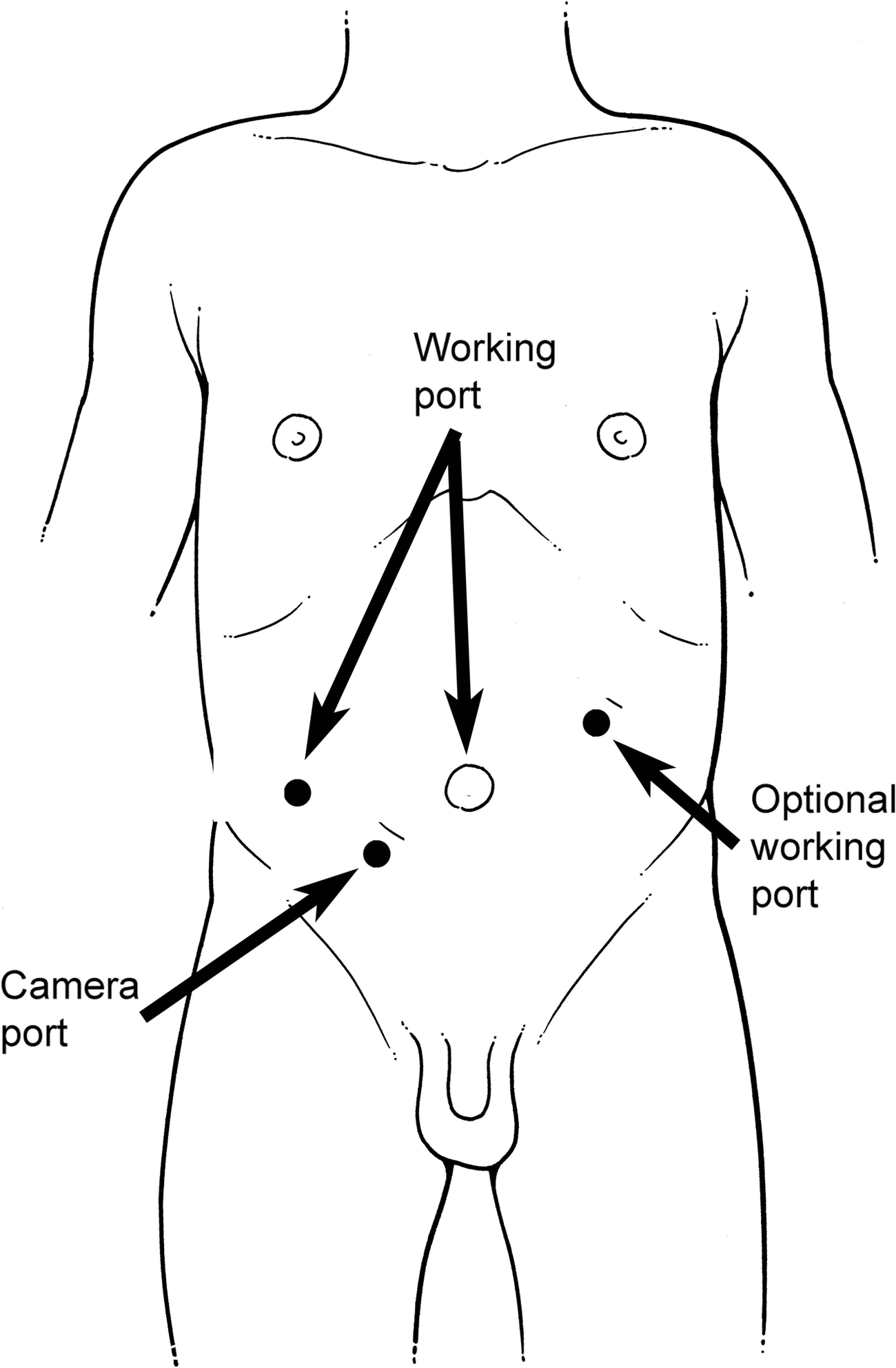
Port placement for repair of CDO.
Results
There were 30 males and 28 females who underwent exploration for duodenal obstruction during this 9-year time period. Ten males and 12 females were in the LAP group. Their median age was 4 days (range: 1 days–10 months) and 3 days (range: 0 days–5 months) for the LAP group and OPEN group, respectively (P=.04). Median weight was 2.5 kg (range: 1.6–8.5 kg) for LAP and 2.4 kg (range: 1.1–9.6 kg) for OPEN (P=.378). The median gestational age was 37 weeks (range: 33–39 weeks) for LAP and 36 weeks (range: 30–41 weeks) for OPEN (P=.335). Six of the LAP patients and 14 of the OPEN were premature. Twenty-six had Down's syndrome (LAP: n=12, OPEN: n=14), 28 patients had congenital heart disease (LAP: n=8, OPEN: n=20), 16 patients had malrotation (LAP: n=8, OPEN: n=8) (Table 1).
Defined as less than 36 week estimated gestational age.
Of the 58 patients who were presented with CDO, 38% were attempted laparoscopically with a 73.7% success rate. Fifty-five percent of the LAP cases were performed by a single surgeon within the practice. The remaining 45% LAP cases were distributed between 4 other surgeons within the practice. Laparoscopic repair included duodenoduodenostomy (n=13), and duodenoplasty (n=3). Five LAP patients had a concomitant laparoscopic Ladd's procedure performed. Six patients were converted to open exploration because of unclear anatomy. Five of the patients who were converted from LAP to OPEN had duodenoduodenostomy and 1 had a duodenojejunostomy. This patient also had “apple peel” jejunal atresia, which was resected and repaired. OPEN repair included duodenoduodenostomy (n=29), duodenojejunostomy (n=2), and duodenoduodenoplasty (n=5).
Average operative time for LAP was 123 minutes with a median of 116 minutes (range: 73–164 minutes). OPEN operative time was 110 minutes with a median of 103.5 minutes (range: 71–220 minutes) (P=.013). Postoperatively, LAP patients remained intubated for 2 days (range: 0–149 days) whereas OPEN patients were intubated for 4 days (range: 0–9 days). Narcotic usage for LAP patients was 3 days (range: 0–148 days) versus 4 days (range: 0–12 days) for OPEN (P=.079). Within the LAP group, the average length of stay was 31.8 days, with a median of 20 days (range: 4–149 days). For OPEN, the average length of stay was 25.6 days with a median of 19 days (range: 6–79 days) (P=.682) (Table 2).
P<.05.
Concomitant procedures during CDO repair were not uncommon. Fifty percent of the patients had an additional procedure(s) during their original operation (n=29). These included Ladd's procedure (n=16), central line placement (n=6), tracheoesophageal fistula repair (n=2), and others (n=10). Twelve of the LAP patients (55%) had additional procedures during their CDO repair. Of the LAP converted to OPEN subgroup, 5 required additional procedures (83%).
Rate of complications between the two groups was similar. Four LAP patients had post-op ileus lasting greater than 20 days. Bacteremia was identified in 1 LAP patient and another had post-op respiratory distress requiring reintubation. There was one death in the LAP group. This patient had Down's, duodenal and jejunal atresia and his operation was converted from LAP to open due to unclear anatomy. The death was from sepsis, almost 5 months after the initial operation. There were no anastomotic complications in the patients who underwent laparoscopic repair. One successful LAP case had to return to the operating room 9 days post-op for a missed malrotation. This was identified on an upper gastrointestinal series after the baby had persistent bilious emesis. At the second operation, the child had an open exploratory laparotomy and Ladd's procedure. The remainder of the patient's hospital course was uneventful. Within the OPEN group, 10 patients had post-op ileus greater than 20 days. One had bacteremia and meningitis. Another suffered from cardiac arrest, but was successfully resuscitated and was discharged from the hospital after a 58-day hospitalization. One patient in the OPEN group required repeat operation after he was found to have free air on an abdominal X-ray 7 days post-op. At repeat laparotomy, anastomotic breakdown was identified. The anastomosis was then revised, and the patient's remaining hospital course was uneventful.
Discussion
The indications for pediatric laparoscopy have increased markedly over the last decade as improved video equipment, smaller instruments, and more experienced surgeons have pushed minimally invasive surgical techniques into the neonatal population. The repair of CDO is a more recent indication.
One of the major advantages of laparoscopy in managing duodenal obstruction is visibility. The lack of bowel distention, which is inherent to a proximal bowel obstruction, was the main factor for visibility. A technical maneuver, placing a transabdominal traction suture through the falciform ligament, was used to facilitate our visibility. This technique eliminated the need for a fourth trocar required for a liver retractor in all but one of the laparoscopic cases.
Clearly there are many variables which may explain the findings we have identified in this study. Administration of pain medication and advancement of feeds are to subject to nursing and physician bias. As is frequently the case, many of the infants underwent multiple procedures during their initial operation. The incidence of multiple procedures during LAP cases was the same as OPEN; however, it is impossible to account for the amount of time spent or the impact of concomitant procedures on measured outcomes. The lack of defined selection criteria for LAP or OPEN is another weakness of a retrospective study of this nature. While the incidence of comorbidities including Trisomy 21 and malrotation was similar between the two groups, it is plausible that surgeon selection played a role in outcomes. Perhaps healthier babies were selected for LAP. Factors which frequently pushed the surgeon to perform the operation OPEN included increased abdominal distention, questionable anatomy, hemodynamic instability, and surgeon's level of comfort with complex laparoscopy.
Even with these understood biases, it is worth noting that outcomes between the two groups were similar. Time spent on the ventilator appeared to be less in the LAP group in addition to an apparent lower narcotic requirement. Median operative time was 13 minutes longer in the LAP group; however, given the technically advanced nature of this relatively new operation this time difference seems reasonable. The benefit of cosmetic outcome for LAP is difficult to argue against OPEN.
In this study, 28% of all patients with CDO had a rotational anomaly found on exploration. If not specifically evaluated, it is feasible that a malrotation could be missed, either laparoscopically or during an open procedure. Given its high incidence, we feel that it is imperative that the surgeon evaluate for malrotation in all babies who present with a proximal obstruction. This can be accomplished intraoperatively.
While we cannot say definitely that laparoscopy is better, our study supports laparoscopy as a safe, first-line approach to duodenal obstruction. Moreover, patients can be managed laparoscopically, even if they require other procedures, such as Ladd's procedures. Laparoscopy certainly has a role in the management of CDO, even in small premature infants with other concomitant surgical diseases.
Footnotes
Disclosure Statement
No competing financial interests exist.