
Abstract
Abstract
Background:
Superior mesenteric artery (SMA) syndrome, also known as Wilkie's syndrome, is a rare condition characterized by vascular compression of the duodenum that leads to intestinal obstruction. While there have been a few recent case reports of laparoscopic duodenojejunostomy performed as an option for surgical treatment, the role of the da Vinci® robot in superior mesenteric syndrome has been underestimated. The authors report a robotic Roux-en-Y duodenojejunostomy for the treatment of SMA syndrome.
Materials and Methods:
A 39-year-old man with a history of Amyotrophic lateral sclerosis presented with an upper gastrointestinal obstruction with distended abdomen. A computed tomography scan showed a transition in the third portion of the duodenum where the SMA vessels crossed over, with a decompressed jejunum. He was identified as a candidate for a duodenojejunostomy. The da Vinci Surgical System was used to mobilize the colon and duodenum, and a Roux-en-Y duodenojejunostomy was performed with hand-sewn anastomosis.
Results:
There were no intraoperative complications. The blood loss was minimal and operative time was 120 minutes. The postoperative course was uneventful with resolution of intestinal obstruction.
Conclusion:
Robotic Roux-en-Y duodenojejunostomy as a surgical option for treatment of SMA syndrome is safe, feasible, and a valid alternative to open surgery with the added benefits of a minimally invasive approach.
Introduction
When conservative management fails, duodenojejunostomy is considered the surgical treatment of choice for SMA syndrome.6–8 However, because it is a rare condition, only a few cases of laparoscopic duodenojejunostomy and a case with robot assistance have been reported to date.9–12 The advantages of performing the operation using a minimally invasive approach are clear and include fewer wound complications, quicker return of bowel function, less pain than the open operation, and a quicker recovery to normal activities for the patient.6,13
Herein, the authors describe the operative technique for a Roux-en-Y duodenojejunostomy using the da Vinci Surgical System® in a patient with an external compression of the duodenum by the SMA.
Materials and Methods
A 39-year-old man with a history of amyotrophic lateral sclerosis presented with upper gastrointestinal obstruction with distended abdomen and vomiting, and was unable to tolerate oral intake. He was treated with bowel rest and nasogastric decompression. A computed tomography (CT) scan of the abdomen and pelvis showed a transition in the third portion of the duodenum where the SMA vessels cross over, with a decompressed jejunum (Fig. 1). An esophagogastroduodenoscopy (EGD) failed to show any intraluminal pathology that would account for the patient's symptoms. The patient consented to a robot-assisted duodenojejunostomy.
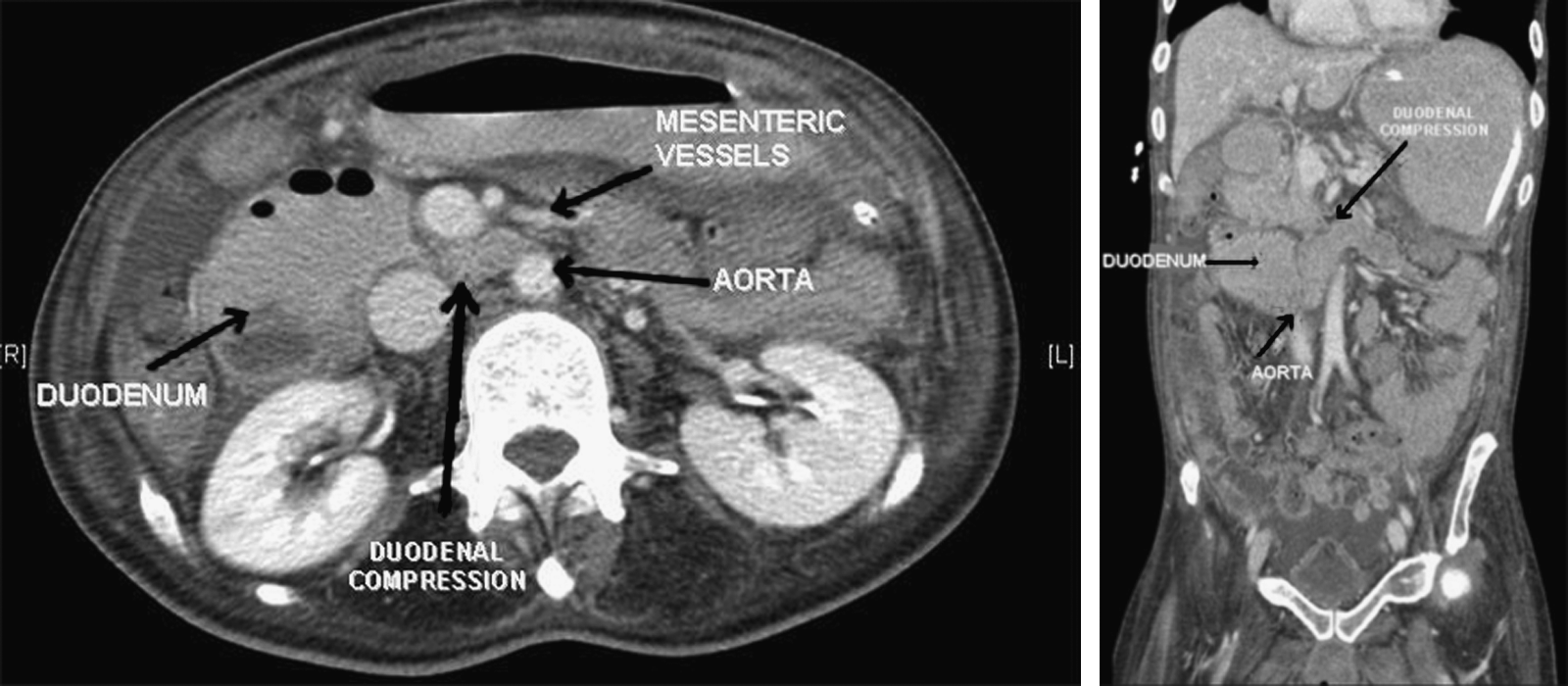
Computed tomography scan of abdomen and pelvis.
The patient was positioned supine in split leg slight reverse Trendelenburg position with arms comfortably tucked to the sides. This allowed the assistant surgeon to stand in between the patient's legs while the robot was docked from the head of the patient. A Veress needle was placed to achieve pneumoperitoneum and the trocars were inserted. The first trocar with a camera port was placed just right of the umbilicus (Fig. 2). An 8-mm robotic trocar was then inserted in the right middle abdomen at the midclavicular line and a second 8-mm trocar in the right middle abdomen at the lateral clavicular line. A third 8-mm trocar was then inserted in the left middle abdomen at the left midclavicular line. A laparoscopic trocar was placed in between the right robotic trocar and the camera port as the first assistant's port. The robot was docked cranially and the robotic arms were attached to the robotic trocars.
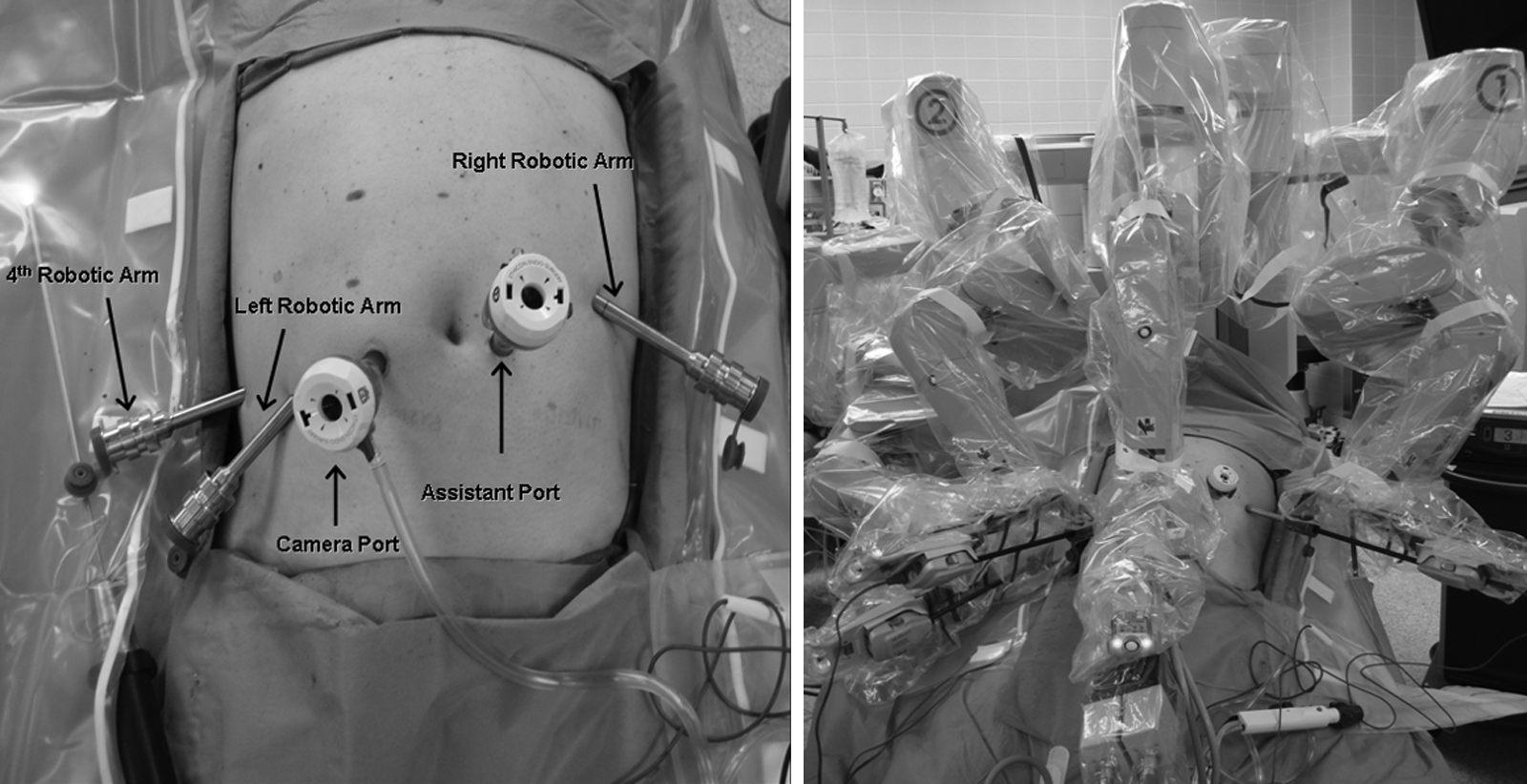
Trocars positioning.
The procedure began with a diagnostic laparoscopy (Fig. 3A). Using a bipolar grasper as the left-hand instrument and a monopolar hook as the right-hand instrument, we mobilized the hepatic flexure and the transverse colon. As a result of the distal duodenal obstruction, the proximal duodenum and the stomach were both dilated significantly. After mobilization of the transverse colon, the dissection began by delineating the duodenum. A Kocher maneuver was then performed to assess any mass effect from the duodenum or pancreas that could account for the patient's symptoms (Fig. 3B). This was initiated by cranially retracting the gallbladder using the robotic fourth arm instrument equipped with Cadiere forceps. The first portion of the duodenum was dissected following the C-shaped curve of the second and third portions of the duodenum. The mesocolon was retracted cranially and the ligament of Treitz was identified. A normal-sized jejunum was confirmed. An Endo GIA™ (Covidien, Norwalk, CT) was used to transect the jejunum, bypassing ∼50 cm of it. A jejunojejunostomy anastomosis was created using the Endo GIA. The common enterotomy was closed using a hand-sewn double-layered technique (Fig. 3C). The Roux limb was brought out antecolic and laid out near the first portion of the duodenum. A hand-sewn double-layered duodenojejunostomy anastomosis was then created using a 3-0 Polydioxanone (II suture) and polypropylene suture (Fig. 3D). The robot was undocked and the fascial defects and wound were closed.
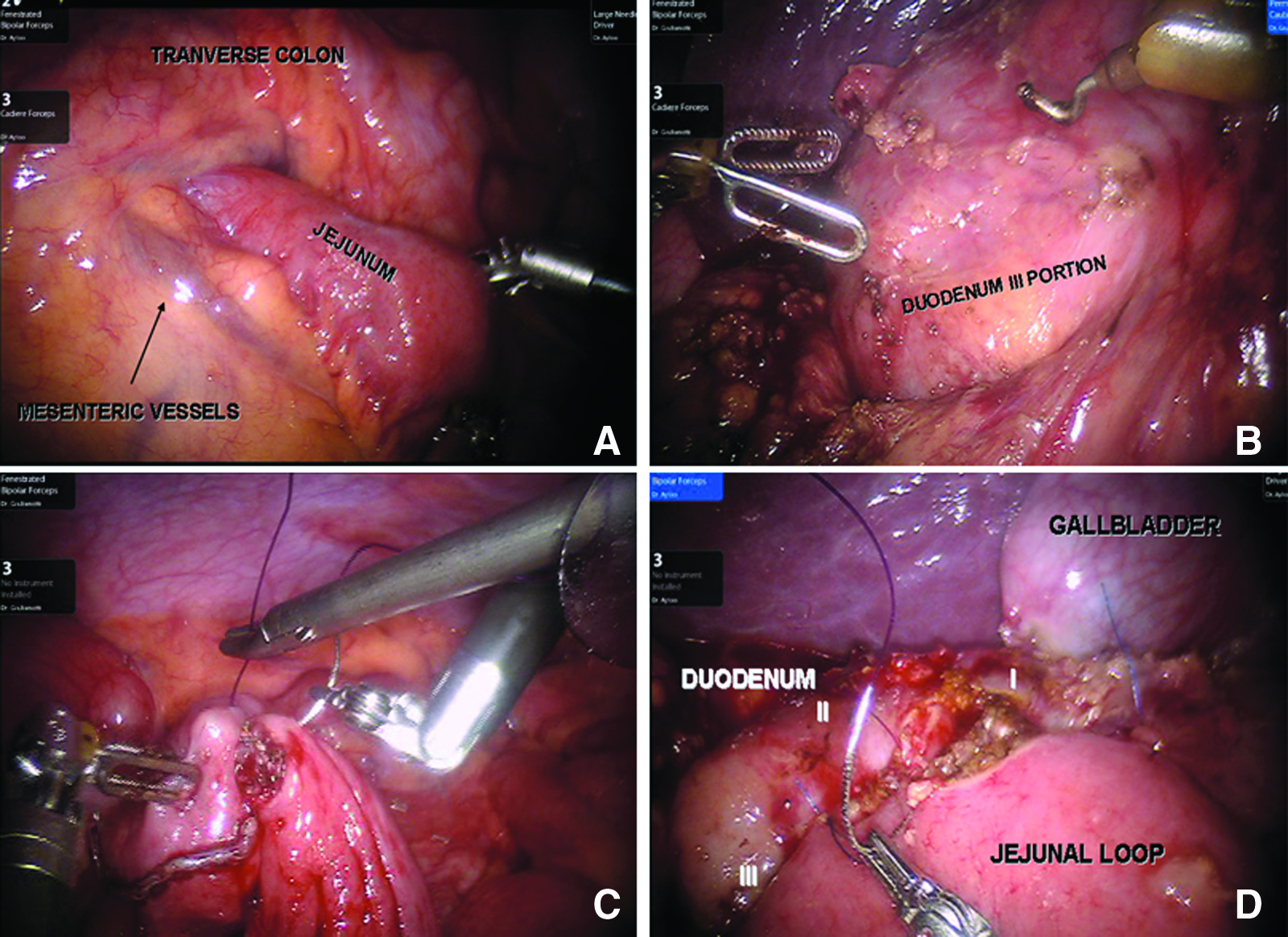
Robot-assisted duodenojejunostomy. Observation of superior mesenteric vessels crossing over duodenum with a decompressed jejunum
Results
The operative time was 120 minutes with minimal blood loss. Follow-up upper gastrointestinal (UGI) contrast study showed contrast passing freely through the duodenojejunostomy without gastrointestinal (GI) leak. The patient was started on peroral (PO) diet and tolerated well postoperatively.
Discussion
Von Rokitansky first described SMA syndrome in 1861. 14 It is a rare disorder with an incidence of 0.013%–0.3%. 1 It is more common in young women and symptoms are typical of upper gastrointestinal obstruction, including vomiting, epigastric pain, postprandial abdominal pain, esophageal reflux, esophagitis, and weight loss. Risk factors that have attributed to SMA syndrome include severe weight loss due to cancer or burns, eating disorders, spinal deformity, trauma, or surgery on the spine along with prolonged supine position with flaccid abdomen.2,4–6 The classical diagnostic criteria are a dilated proximal duodenum and an aortomesenteric angle of <20° with the aortomesenteric distance reduced to 8 mm. 9 The aortomesenteric angle usually ranges between 38° and 65° with an aorta-SMA distance of 13–34 mm. 2 Typical findings on CT scan include a dilated proximal duodenum with external compression of the third portion of the duodenum by the SMA vessels, and a collapsed jejunum.
Treatment options for SMA syndrome involve medical management using tube feedings to increase both weight and the mesenteric fat pad. 7 If symptoms persist, surgical options for treatment can include less accepted methods of severing the ligament of Treitz or a gastrojejunostomy. More acceptable standards of care have been proposed, including a duodenojejunostomy bypass, proposed by Wilkie et al. in the largest series on 75 patients. 1 This procedure has traditionally been performed in an open approach, with only a few laparoscopic cases reported and 1 case performed in entirety with robotic assistance recently.12,15 The advantages of the laparoscopic approach are less pain, early recuperation, better cosmesis, and lower rate of incisional hernia, in addition to other cardiopulmonary benefits to the patient.
Butter et al 12 recently reported the treatment of a patient with SMA syndrome by a hand-sewn robotic duodenojejunostomy side-to-side anastomosis with good result. Herein, we describe a Roux-en-Y duodenojejunostomy performed robotically as a surgical treatment option for SMA syndrome. For this procedure, we found it best to set up the trocars in the same way as they are set up for a pancreatic operation. This is done in the event that intraoperative findings of duodenal or head of pancreas lesions appear, accounting for the patient's symptoms. It is also prudent to explore these areas at the beginning of the operation. The next step involves mobilization of the hepatic flexure and transverse colon, followed by Kocherization of the duodenum. Here, the advantage of using the robotic system 16 is the use of the fourth arm for elevation of the liver and gallbladder. The utility of a monopolar hook with the Endowrist® provides the surgeon with better ergonomics. Additionally, 3D vision with magnification provides enhanced observation to mobilize the distorted and dilated duodenum.
The mesocolon is retracted cranially using the fourth arm of the robot and exposing the ligament of Treitz. With the jejunum at normal size, the jejunojejunostomy anastomosis was created and the common enterotomy hand-sewn closed. This anastomosis usually falls in the left middle abdomen, which could be challenging to suture in a standard laparoscopic approach. With the higher degree of freedom allowed by robotic instruments, this can be precisely and comfortably performed with good ergonomics. Even though creating a Roux-en-Y might be time consuming with an additional anastomosis, it constitutes a more physiological reconstruction avoiding blind loop syndrome. Additionally, the second portion of the duodenum can be reached easily decreasing the tension on the duodenojejununostomy or avoiding jejunal loop twisting.
The final step of the operation is creation of the duodenojejunostomy. This can be performed using either a hand-sewn technique or a stapler. The location of the anastomosis on the duodenum is ergonomically limiting, depending on the trocar position. This is where the best utility of the robotic system can be seen, where the anastomosis can be positioned at an optimal position and the jejunum can be properly aligned to the duodenum with the creation of a hand-sewn anastomosis using precise reproducible placement of sutures.
Conclusion
Robotic Roux-en-Y duodenojejunostomy is feasible and safe. The added benefit of a fourth arm for retraction, exposure, and better observation in a distorted anatomy setting, combined with instruments that offer higher degrees of freedom, allows for precise, reproducible suturing and dissection. This, in addition to other benefits of minimally invasive surgery, makes this technique an option worthy of further investigation for the treatment of SMA syndrome.
Footnotes
Disclosure Statement
No competing financial interests exist.