
Abstract
Abstract
Background:
Incidentally detected early gallbladder cancer (IDEGB) is an early carcinoma first diagnosed on microscopic examination after a cholecystectomy for symptomatic benign gallbladder disease. After diagnosis of IDEGB it is often necessary a completion of treatment by a second tailored revision procedure. Despite early reports contraindicating laparoscopic approach because of high risk of neoplastic seeding, recent data seem to demonstrate that this approach per se does not influence clinical outcomes. We refer our experience in revision surgery by a totally laparoscopic approach that includes hepatic resection, lymphadenectomy, and port-sites excision.
Methods:
From January 2006 to March 2008, four patients with IDEGB were carried out to revision procedure by a totally laparoscopic approach. The mean operative time of procedure has been 162 minutes, whereas blood loss has been <100 mL (mean 85.1±23.3 mL). The postoperative course has been uneventful in all patients and perioperative mortality (within 40 days from intervention) 0. Hospital stay has been, respectively, 4, 5, 5, and 6 days (mean 5 days). During follow-up, at the last fluorine-18-labeled fluordesoxyglucose–positron emission tomography (FDG-PET) scan examination, respectively, 4, 3, and—for 2 patients—2 years after revision laparoscopic procedure, pathologic FDG accumulation was not reported.
Conclusions:
Totally laparoscopic revision surgery for IDEGC seems to be a legitimate procedure, and, in our experience, reports satisfactory clinical outcomes in terms of perioperative and middle term oncological results. Larger and prospective studies are needed to support definitively oncological safety of this approach.
Introduction
When IDEGB is diagnosed after a laparoscopic procedure, it is often necessary a completion of treatment by a second revision procedure. Data from the literature recommend a tailored approach, based on parameters of pT category of TNM stadiation. Despite early reports contraindicating laparoscopic approach because of high risk of neoplastic seeding, recent data seem to demonstrate that this approach per se does not influence clinical outcomes.
In this article we refer our experience in revision surgery for IDEGB by a totally laparoscopic approach that includes hepatic resection, lymphadenectomy, and port-sites excision (PSE).
Materials and Methods
From January 2006 to March 2008, four patients were admitted at General and Hepato-Pancreato-Biliary Surgery of Loreto Nuovo Hospital after histological diagnosis of unexpected cancer of gallbladder removed by laparoscopy followed to a preoperative diagnosis of symptomatic lithiasis.
All patients were female and were hospitalized in our Unit for management of supposed residual disease; three had diagnosis of adenocarcinoma of gallbladder staged pT1b and one pTis.
Blood tests, including CEA, CA19.9, CA15.3, and CA125 levels, came within the normal range; in all patients, ultrasonography, contrast-enhanced spiral computed tomography, magnetic resonance cholangiopancreatography, and whole-body fluorine-18-labeled fluordesoxyglucose positron emission tomography (FDG-PET) scan were negative for liver and/or body metastasis.
In particular, bile and pus spillage in abdomen caused by gallbladder perforation was reported in the operative note of first intervention of pTis patient. Moreover, microscopic examination described “a well differentiated neoplastic proliferation, with papillar architecture on epithelial coating and moderate/severe level of dysplasia.” Before our assessment, the patient was readmitted to previous Institution for suspect lump on abdominal wall in correspondence of right 10-mm port-site 3 months after cholecystectomy. Excision of parietal neoplasm was carried out and microscopic examination referred a diagnosis of wound metastasis from papillar adenocarcinoma.
Proposed reintervention was laparoscopic resection of hepatic bed, lymphadenectomy N1 with PSE 5 (Fig. 1). According with others,4,6–8 resection of biliary tract was not provided because infiltration of cystic duct was not present.
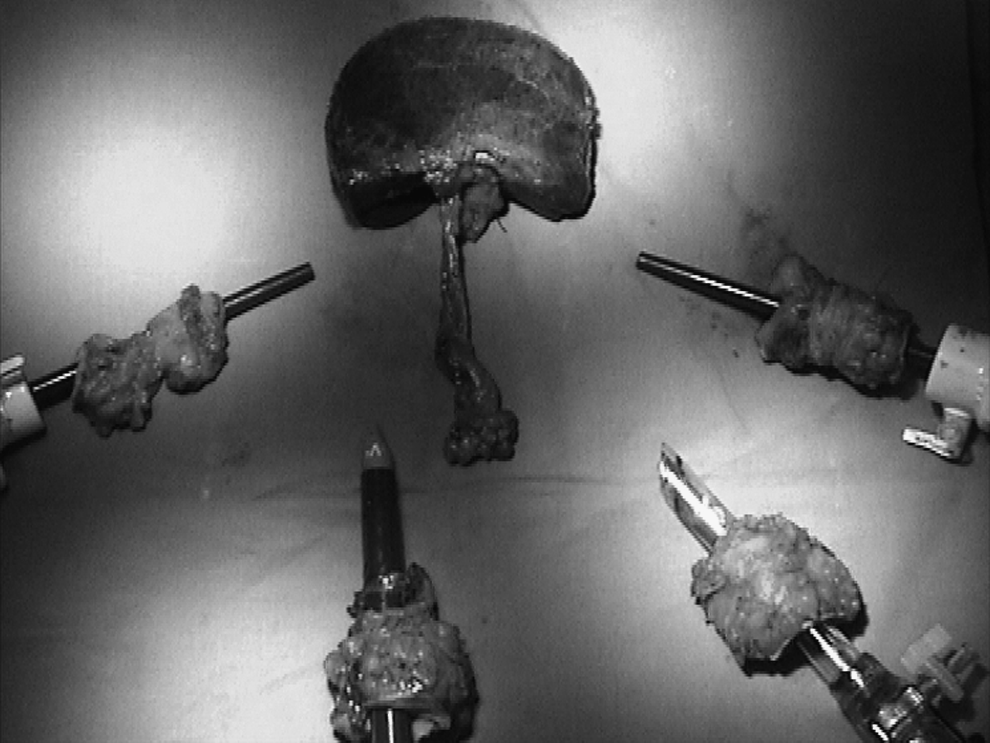
Liver specimen and port-sites.
Surgical technique
The patient under general anesthesia was placed in the supine position with a moderate left-lateral decubitus, and in reverse Trendelenburg position to prevent the risk of gas embolism. The primary surgeon was positioned between the patient's legs, with one assistant on each side.
With an open technique, continuous carbon dioxide pneumoperitoneum was induced at a pressure of 12 mmHg. We used a four-trocar configuration. A 12-mm port at the umbilicus housed a 30° videocamera. Another trocar was positioned in the paraxiphoid region, and two other trocars were located under direct vision in a semicircular line, with the concavity facing the right subcostal margin. These last two trocars also carried a 5- to 12-mm port to allow an easy change of the instruments, to provide the opportunity to use a harmonic scalpel (UltraCision®; Ethicon Endosurgery) or a vessel-sealing device (Ligasure; Covidien) with both the right and left hands and to facilitate the introduction of endostaplers if necessary.
A diagnostic and staging procedure was performed and the liver was examined using laparoscopic ultrasonography (B&K Medical; Laparoscopic surgical transducer 8666) to detect presence of possible neoplastic tissue, residual to first intervention or developed after laparoscopic procedure.
Peritoneal adhesions corresponding to cutaneous scar of port-sites were excised first in order to staging disease.
Laparoscopic Pringle maneuver was prepared, but there was no need to perform it as previously referred. 9
Resection of gallbladder fossa (Fig. 2) was carried out in all reoperated patients under repeated ultrasound control to know the vascular intrahepatic map and ensure oncologically correct deep margins.

Laparoscopic hepatic resection.
Laparoscopic lymphadenectomy of hepatoduodenal ligament was performed. At the end of hepatic procedure, PSE was performed by a cutaneous elliptical incision around the trocars, about 2 cm in diameter, and removal of a complete cylinder of abdominal wall from the skin to the peritoneum.
Results
The mean operative time of procedure has been 162 minutes, whereas blood loss has been <100 mL (mean 85.1±23.3 mL). The postoperative course has been uneventful in all patients and perioperative mortality (within 30 days from intervention) nil. Hospital stay has been, respectively, 4, 5, 5, and 6 days (mean 5 days). Microscopic examination of specimens was negative for all patients except for that previously undergone to parietal metastasectomy. In previously operated port-site, a centimetric focus of adenocarcinoma cells was detected.
All nodes were negative to neoplastic invasion.
Length of follow-up was, respectively, 51, 42, and 30 months for initially staged T1b patient, and 25 for Tis patient. Besides a 6-month CT scan, annual whole-body FDG-PET scan was taken to identify neoplastic foci undetectable to conventional CT scan. At the last FDG-PET scan examination, respectively, 4, 3, and, for 2 patients, 2 years after revision laparoscopic procedure, pathologic FDG accumulation was not reported.
Discussion
We referred our procedure of completion surgery in 4 patients with an incidentally detected gallbladder cancer diagnosed first on microscopic examination after a cholecystectomy for symptomatic benign gallbladder disease by a totally laparoscopic approach.
Historically, gallbladder cancer has ever been a taboo for laparoscopic surgeon because of former and isolated literary reports referring an early onset of widespread peritoneal carcinomatosis or port-sites metastasis after laparoscopic cholecystectomies in patients with unexpected cancer of gallbladder.1,10–12
Some investigators remarked a permissive effect of CO2 pneumoperitoneum on peritoneal neoplastic seeding and the physical influence of intraabdominal pressure on cells diffusion based on experimental animal models.13–16
Conversely, some authors verified in multivariate analysis that, despite findings from experimental models, laparoscopic approach per se does not influence prognosis in IDECG. Surgical complications such as gallbladder perforation or bile spillage in abdomen that can result more frequently in mininvasive approach, as in the most recent single-incision laparoscopic surgery technique (SILS) where gallbladder is frequently suspended by a straight-needle sutures passed through the abdominal wall, could be the effective element determining neoplastic seeding. 17
Suzuki et al. 18 in a study on bile spillage documented association between gallbladder perforation and port-sites/peritoneal recurrences. Sarli et al. 19 verified that gallbladder perforation during laparoscopic cholecystectomy worsens prognosis of disease, increasing incidence of port-sites/peritoneal recurrence. Paolucci et al. 20 first compared data from open and laparoscopic cholecystectomies in a study on German registry that included 245 patients and reported that, in cases of IDECG, incidence of abdominal wall recurrences was very similar (7% versus 5.1%) and overall incidence of recurrences was slightly higher after open cholecystectomy (31% versus 27%). This study concluded that access approach, open or laparoscopic, not seems to influence prognosis of an IDEGC.
Wakai et al. 21 reported that incidence of port-sites/peritoneal recurrence was significantly higher in patients with gallbladder perforation (3/7, 43%) than in those without (0/21, 0%). In a multi-institutional series from Japan, Ouchi et al. 22 also demonstrated that gallbladder perforation during open or laparoscopic removal is associated directly to a significantly lower survival rate.
Goetze and Paolucci 23 reported that for 5-year survival T2 staged gallbladder tumors, no significant differences are seen between laparoscopic treatment, open treatment, and intraoperative conversion in patients undergone to a revision surgical procedure.
These findings lead to consider, as is occurred for surgery of colon, liver, stomach, and pancreas, that laparoscopic approach to IDEGC should be a safe practice in an oncologic viewpoint, if surgical complications do not occur. Further, this has been our theoretical and rational base to a totally laparoscopic approach to the revision procedure for IDEGC, performed in patients without gallbladder, therefore with no risk of spillage and seeding.
On the other hand, recently, some authors24–27 presented feasibility and safety of intentional laparoscopic treatment of early-stage gallbladder cancer diagnosed preoperatively without evidence of liver invasion with resection en bloc of gallbladder and hepatic parenchyma.
According many authors,21–22 we usually treat very early tumors (Tis and T1a) with simple cholecystectomy alone; tumors invading muscle layer (T1b) with cholecystectomy extended to hepatic bed or associated to segmentectomy of S4b and S5, lymphadenectomy, and PSE.
In our series, hepatic resection was performed in 1 patient with carcinoma in situ (Tis), but evidence of seeding on a port-site could appear an overtreatment. Even if distant port-sites metastasis and local parenchymal extensions are not strictly correlated, we considered wall seeding as an unfavorable biological behavior of disease; therefore, we carried out a more extensive procedure to remove potential undetectable micrometastasis.
In our practice we translated our technical findings learned during our experience in laparoscopic surgery of liver, 28 performing all therapeutic items of revision surgery as in traditional approach.
Magnitude of procedure, in terms of number of excised nodes and integrity of specimens, seems not to differ between open and laparoscopic approach.
Conclusions
Our study reports satisfactory outcomes in terms of perioperative and middle term oncological results for mininvasive procedure of completion treatment of IDEGC. This approach seems to propose well-known advantages of laparoscopy, providing all oncological items of traditional approach. Larger and prospective studies are needed to support definitively the safety of this procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.