
Abstract
Abstract
Since the awakening of single-port laparoscopy and culdolaparoscopy and with the increased interest in minilaparoscopy-assisted natural orifice surgery and pure natural orifice peritoneoscopy, laparoscopists are in pursuit of techniques with less percutaneous assistance. We made a rein using a 6-cm straight cutting edge needle in a 2–0 nylon suture with a large clip tied near the end as stoppage. We are also presenting an optional technique of placing the 6-cm straight needle backward, when the diameter of the cannula does not allow the parallel passage of the needle holder. The rein is simple, inexpensive, and easy to assemble, and may solve some problems of traction and triangulation without additional ports.
Introduction
Surgical Technique
Our experiment was conducted with simulators. We used a laparoscopic trainer (Lap trainer with Simuvision; Simualb Corp.). The rein is a 2–0 nylon suture that is 75 cm in length with a 6-cm straight cutting edge needle (Ethilon; Ethicon), and for the stoppage we used a large Hem-o-lok clip (Weck) placed in a clothes pin fashion and secured it with three knots near the end of the rein leaving a tail of 1 to 1.5 cm between the stoppage and the end of the suture 5 (Fig. 1).
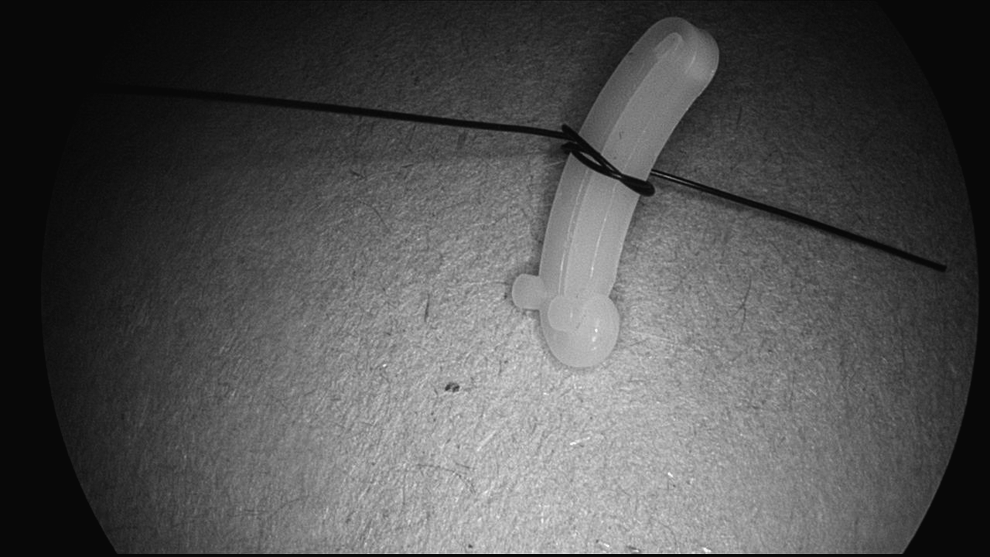
The Hem-o-lok stoppage.
The following step is used in threaded ports when the lumen of the cannula does not fit the needle and holder in parallel. The needle is grasped at the sharp end with a needle holder and is introduced into the 5-mm cannula. With this maneuver, the Back End Enters First (BEEF) in the abdominal cavity while holding the sharp end of the needle (Fig. 2).
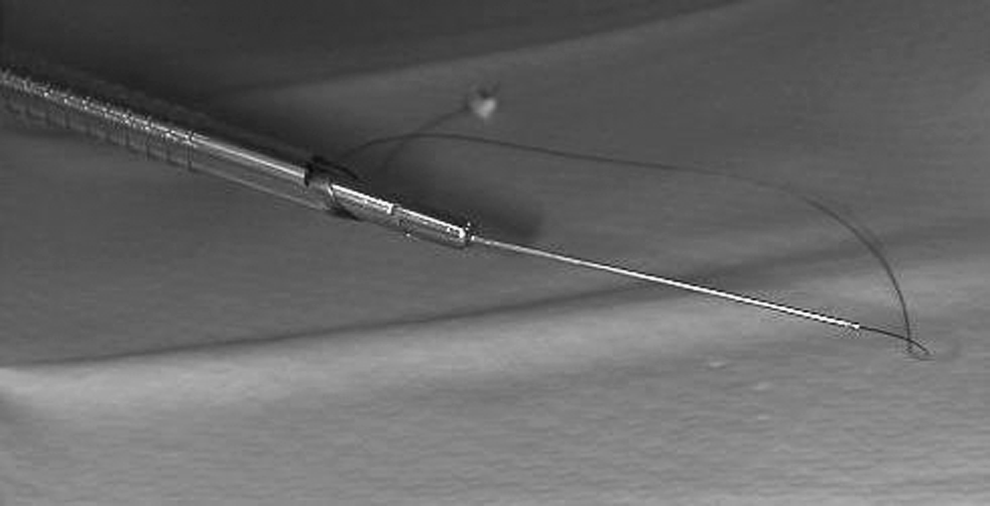
The blunt end enters first.
The next steps are the same for the customary parallel introduction and the BEEF.
The needle is brought to a safe area to reposition the needle holder. The needle is passed through the designated target and is re-grasped. The needle is placed perpendicular to the parietal peritoneum for percutaneous extraction. The needle is pushed through the full thickness of the abdominal wall and grasped outside the skin with a Kelly clamp. The needle holder is removed to allow for the passage of the stoppage.
As the extraction continues pulling the rein out of the skin, the stoppage will enter the cannula. Occasionally, the Hem-o-lok may have to be manually aligned at the entrance of the port; some port models need a valve opening for the passage of the Hem-o-lok in and out. As we continue to pull, the Hem-o-lok reaches its target. The rein is held as a marionette with a Kelly clamp at a distance of 10 to 15 cm from the skin. The rein is cut above the clamp and the needle end is disposed. For removal, the spring end of the Hem-o-lok was grabbed and withdrawn completely.
We were able to maneuver a BEEF with the sharp end of the needle protected at all times until a safe repositioning area was reached. The Hem-o-lok stoppage performed well, providing strong traction and triangulation.
Discussion
Dr. Davila designed a rein that consists of a 2–0 polypropylene suture with a 6-cm straight needle that has a silastic embolus of a small syringe plunge tied near the end. The rein was successfully used in transvaginal cholecystectomies in Mexico. 5
Dr. Tsin modified the rein for its use in the United States. The silastic embolus was changed for a large Hem-o-lok clip (Weck). 5 The length of the rein could be shorter than 75 cm when it is used in laparoscopy and single-port laparoscopy.
Dr. Davila et al. introduced the rein via a 16-mm port using a customary approach of grasping the suture 2 cm from the needle and pushing the holder and the needle through the cannula. The needle holder leads the way into the abdominal cavity followed by the needle. The needle is brought to a safe area to reposition the needle holder. 5
Not all 5-mm cannulas are the same (Fig. 3). Most 5-mm ports are suitable for the customary needle introduction, including threaded ports with a slightly larger outer diameter. Placing the needle via the 5-mm cannula is more challenging when the lumen of the cannula does not fit a 5-mm needle holder and the needle in parallel. The surgeon must check beforehand for a parallel passage and choose to either change to a different 5-mm port that is fit for a customary placement, change to a narrow needle holder, or use BEEF as an alternative introduction method. Planning ahead avoids changing or re-inserting ports during surgery. The narrow needle holder is used until the needle reaches the safe reposition area. This is followed by a change for a larger diameter instrument that gives the strength needed to push the needle through the full thickness of the abdominal wall.
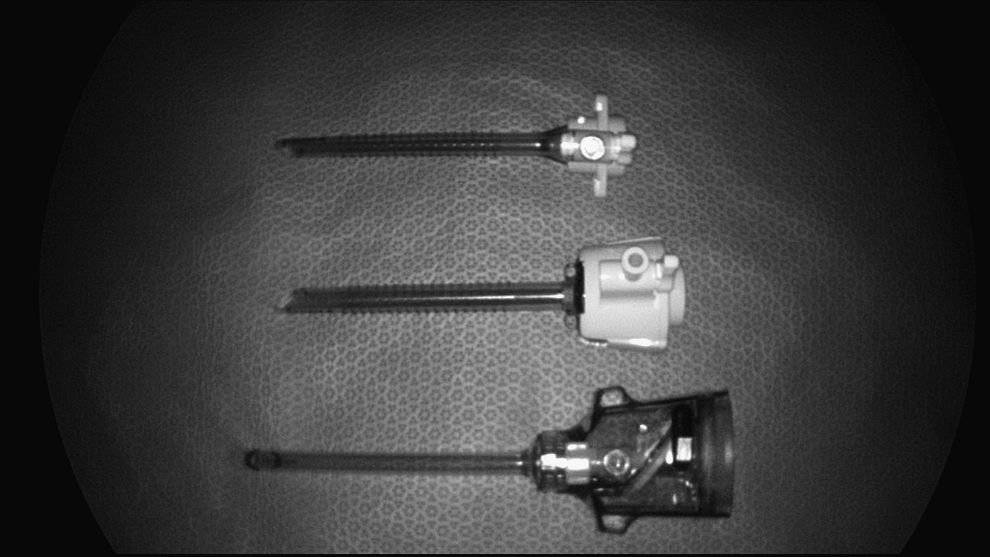
Five-millimeter cannulas. The one on the top does not fit a parallel passage of needle and holder.
The rein has a stoppage, a percutaneous exit, and a marionette string, and the traction is done directly to the stoppage and indirectly to the target. The leash is different: it has no stoppage, it uses a percutaneous needle entrance and exit, it has two marionette strings, and the traction is directly to the target.1,4 The tensile strength of the 2–0 nylon is 4.2 kg and the knot strength is 2.4 kg; therefore, the limitation of traction is in the texture of the target with the possibility of tearing.
Urologist laparoscopists had developed ingenious ways to place the Hem-o-lok for aid in suturing and studied the traction force capabilities and limitations. 6 Further, the rein could be used in laparoscopy instead of the leash, 4 the hitch, 7 or marionette leashes. 1
Triangulation and strong traction are sometimes difficult to achieve in laparoscopy without additional ports and are often difficult in single-port laparoscopy8,9 and natural orifice transluminal endoscopic surgery. 5 We developed a simple, inexpensive, and easy-to-assemble laparoscopic rein that may solve some of the above-mentioned difficulties using a less percutaneous assistance. The feasibility and reproducibility of these methods is encouraging. However, a large number of operations are needed to prove the benefits of these surgical proposals.
Footnotes
Acknowledgments
To the nurses and technical personnel of the operating room and the endoscopy suite that participated in and helped us with this simulation.
Disclosure Statement
No competing financial interests exist.