
Abstract
Abstract
Background:
Inguinal hernia repair is the most common procedure in pediatric surgery. Suture techniques for laparoscopic inguinal hernia repair in children are easy to perform and popular with a low recurrence rate. The aim of this study was to evaluate the effect of laparoscopic preperitoneal injection of three-dimensional gel on closing of the inguinal hernia sac (IHS) in laboratory animals.
Materials and Methods:
With the animals under general anesthesia, we performed peritoneoscopy in 12 male Chinchilla rabbits weighing 1200–1400 g. The endoscope was introduced into the abdominal cavity, and bilateral deep inguinal rings were identified. A Tuohy needle with the injectable polymeric bulking agent DAM+™ (three-dimensional polyacrylamide gel with silver ions [Argiform® from Bioform®]) was introduced preperitoneally. The implant was then injected across the entire orifice of the deep inguinal rings and draped over the cord structures. After completion of bilateral repairs, the rabbits were extubated and observed in the animal laboratory. Then the second laparoscopy was performed 6 months later, and the deep inguinal rings were inspected.
Results:
The postoperative course was uneventful in all the animals. At the second laparoscopy no reopening of the entire orifice of the deep inguinal rings was noted. Accurate placement of the polymeric agent and adequate coverage of the vas deferens were accomplished in all the animals.
Conclusions:
This study demonstrates that the biopolymeric implant gives good postoperative results and a stable trend of closing the IHS in long-term follow-up. In conclusion, we hope that injectable polymeric bulking agents can be used for treatment of inguinal hernias of pediatric patients after additional animal and human research.
Introduction
The surgical principle in laparoscopic repair is to close the patent processus vaginalis at its neck like in the open repair. Different techniques of laparoscopic hernia repair have been developed, but there are two basic approaches—a purely intracorporeal ligation and laparoscopic-assisted extracorporeal ligation.
In the past, several new techniques using tissue adhesive agents in pediatric inguinal surgery were reported. Injection of 2-octyl-cyanoacrylate at the level of the internal inguinal ring in experimental models has show good results in terms of safety and efficacy of closing the orifice of the inguinal hernia sac (IHS). 5
The aim of our study was to evaluate the effect of laparoscopic preperitoneal injection of three-dimensional gel (DAM+™) (Bioform®) on closing the orifice of the IHS in laboratory animals.
Materials and Methods
DAM+ is three-dimensional polyacrylamide containing ions of silver. It comes in a sterile syringe with an 18-gauge×1½-inch needle. DAM+ is an atoxic, stable, nonresorbable sterile watery gel consisting of approximately 2.5% cross-linked polyacrylamide and nonpyrogenic water. The presence of silver ions in DAM+ contributes to low reactivity and reduces the risks of local inflammation. The permanent fillers (silicone oil and polyacrylamide gel) have been used in plastic and reconstructive surgery for many years: Silicone mainly in the United States and polyacrylamide gel in most countries outside the United States and Canada. In Russia, polyacrylamide hydrogel is the most popular biopolymeric implant and has been used widely in surgery for more than 10 years.
Because the inguinal canal of rabbits remains open and patent throughout life and the internal inguinal ring also is open and wide, rabbits were chosen for laboratory study. Twelve male Chinchilla rabbits weighing 1200–1400 g were used as model subjects. All animals had unrestricted access to food and water pre- and postoperatively. Experimental work was done according to the “Hospital Experimental Work State” and “Institutional Review Board” and was approved by our institution's ethical committee. After completion of the experiment all animals were alive.
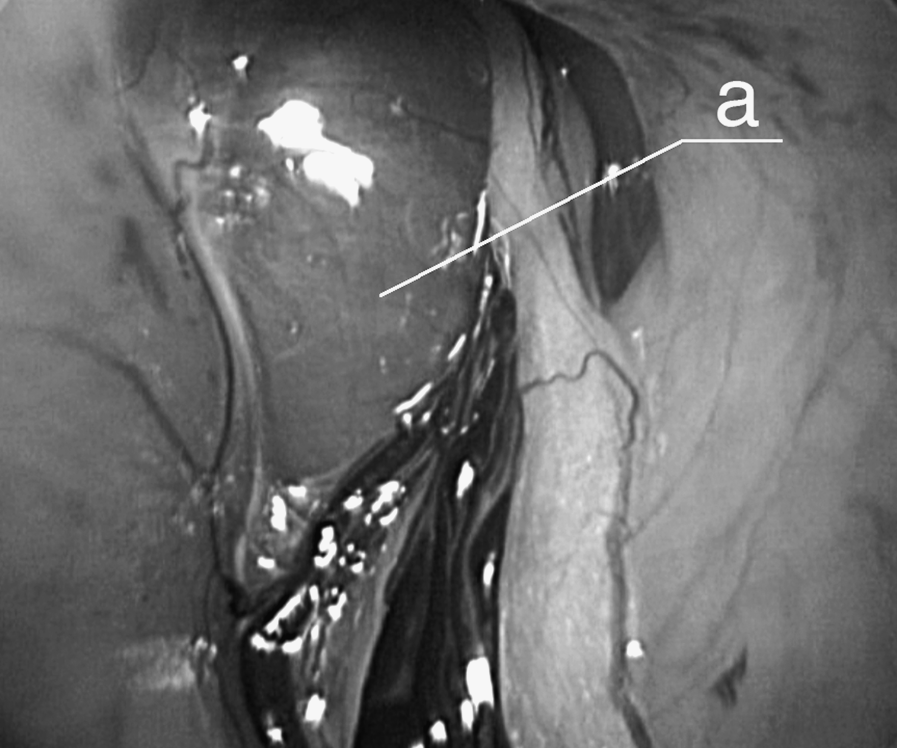
All animals were placed supine, and laparoscopy was done with the rabbit under general anesthesia. Acepromazine (0.25 mg/kg), midazolam (1 mg/kg), and meperidine (5 mg/kg) were administered intramuscularly as premedication. General anesthesia was induced with 5% isoflurane, using a tracheal tube, and maintained with 3%–4% isoflurane under manual ventilation. A 5-mm trocar was inserted in the epigastrium, and carbon dioxide was insufflated at a pressure of 4 mm Hg and flow rate of 1 L/min. A 5-mm laparoscope was introduced through the epigastric trocar, and bilateral internal inguinal rings were identified (Fig. 1). The Tuohy needle with injectable polymeric bulking agent DAM+ (three-dimensional polyacrylamide gel with silver ions [Argiform® from Bioform]) was introduced preperitoneally (Fig. 2). The 2.0 mL of implant was then injected across the entire orifice of the internal inguinal rings and draped over the cord structures (Fig. 3).
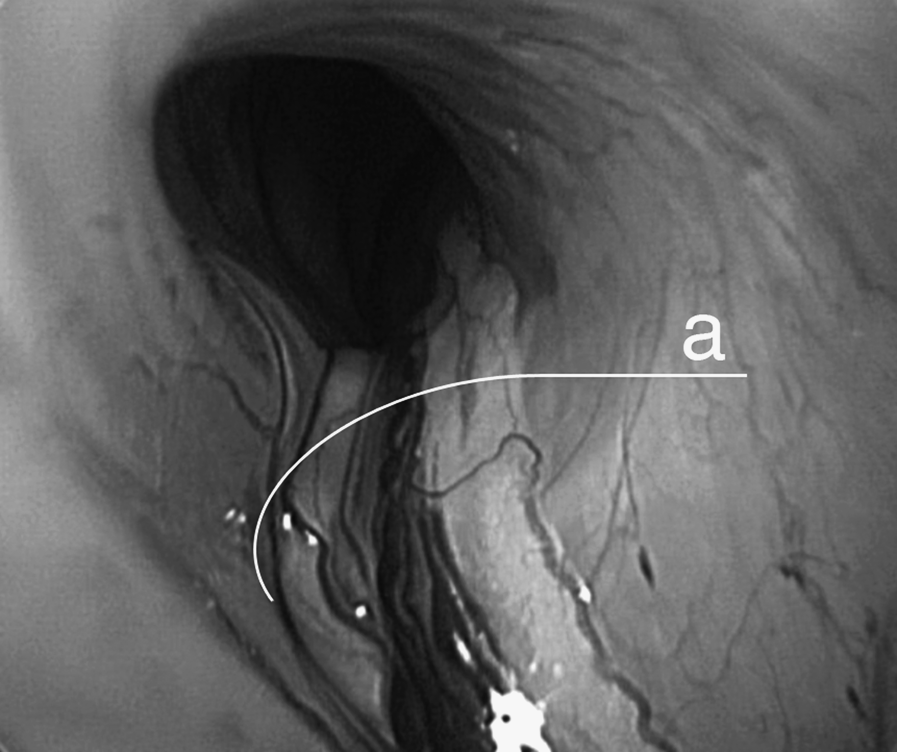
Laparoscopic view of the orifice of the inguinal hernia sac in a Chinchilla rabbit. The arrow (a) indicates the spermatic cord and vas deferens.

Tip of the Tuohy needle (a) before the gel implantation.
View of the inguinal hernia sac after the laparoscopic inguinal preperitoneal injection procedure with preperitoneal placement of the polymeric agent (a).
After injection of the bulking agent and closing of the orifice of the IHS, the rabbits were extubated and observed in the animal laboratory. A second laparoscopy was performed 6 months later using the same technique. At the second procedure the integrity of the closed internal inguinal rings and the presence of ring abscess, peritonitis, and adhesions were recorded.
Results
Mean operative time ranged from 10 to 12 min for bilateral hernia repair. Time required to inject DAM+ was less than 1 min. Postoperative recovery was rapid, and all animals returned to normal activity by 10–12 h after the procedure.
At the second laparoscopy integrity of the closed internal inguinal ring was present. No opening of the rings was observed. Accurate placement of the polymeric agent and adequate coverage of the vas deferens were accomplished in all the animals. Adhesions between the closed orifice of the IHS and the small bowel were absent in all 12 rabbits. There were no signs of peritonitis and abscess formation.
In the current study, histologic examination clearly showed that mild inflammation was localized within the IHS only adjacent to the gel, and there were no histopathologic changes detected around the vas deferens and spermatic vessels.
Discussion
Multiple techniques have been described for inguinal hernia repair in children. In traditional open repair, the inguinal canal must be opened, and the hernia sac is dissected from the spermatic cord; this procedure is associated with various postoperative complications such as recurrence, testicular atrophy, iatrogenic testicular fixation, and injury to the vas deferens or bladder, especially in cases of prematurity or low birth weight. 6 Several years of experience with transinguinal laparoscopy to study the contralateral side during open repair of inguinal hernias in children convinced us that transperitoneal endoscopic visualization of the internal ring with ligation or suturing is safe and simple. Standard laparoscopic inguinal hernia repair involves less dissection of the spermatic cord structures, but it requires using sutures to close the neck of the IHS, which has some risks of complications.7–9 Some concerns have been raised on whether the suture would compromise testicular vessels. To answer this question Schier et al. 10 evaluated 65 boys with unilateral and bilateral inguinal hernias who were treated laparoscopically. Using neuromonitoring (O2C; LEA Medizintechnik GmbH, Giessen, Germany), which combines light spectroscopy and laser Doppler technique, these authors showed that testicular perfusion is not influenced by the laparoscopic inguinal hernia repair using suture closure of the IHS.
There are two basic laparoscopic approaches: Intracorporeal suturing and a laparoscopic-assisted extracorporeal ligation. The first large series of intracorporeal repair was reported by Schier, 11 with primary closure of the peritoneum lateral to the cord with interrupted sutures. This technique was then modified to use a Z-suture closure rather than interrupted sutures. 12 In these series the recurrence rate was 2.6%, which is slightly higher than that seen with the open repair.
Other modifications include an N-suture instead of a purse-string suture 13 and the “flip-flap” hernioplasty, in which two folds of peritoneum are used to cover the inguinal ring. 14 This technique has an advantage of allowing the scrotum to drain, preventing postoperative hydroceles.
Intracorporeal techniques require closing the hernia opening by suturing within abdominal cavity, with the suture material tied intracorporeally and the knot remaining in the abdominal cavity. This procedure is not easily performed. Thus many techniques are directed at simplifying these difficulties. In 1995 Takehara et al. 15 introduced a new simplified method, known as laparoscopic percutaneous extraperitoneal close (LPEC). In 2006 they reported personal experience with a total of 972 LPECs performed in 711 children with recurrence rate of 0.73%, and no hydroceles or testicular atrophy occurred after surgery. 16 The authors concluded that the LPEC technique not has only cosmetics advantages, but also combines a low risk of injury to the spermatic duct and vessels.
On the other hand, in extracorporeal closure of the IHS with using the technique of subcutaneous endoscopically assisted ligation, a small stab wound is made over the inguinal ring, and a suture is passed through the abdominal wall behind the peritoneum. It is then directed around the internal ring, avoiding the vas deferens and vessels, and passed out the same stab wound. It is tied extracorporeally under laparoscopic visualization. Initial reports of this technique showed complications of 15.7% and a recurrence rate of 4.3%, which is higher than in the open or intracorporeal laparoscopic repairs. 4
Laparoscopic hernia surgery continues to evolve with new polymeric products allowing surgeons multiple choices in treating their patients. In 2004 Miyano et al. 5 published experimental work with injection of 2-octyl-cyanoacrylate (Dermabond®, Ethicon) into the right IHS under laparoscopic control. This technique is an innovative concept for the treatment of inguinal hernia because it uses tissue adhesives to close the hernia sac. This approach eliminates dissection of the spermatic cord and ligation of the IHS, thus virtually completely lowering the risks of injuries. 5 Later, in 2005, the same group of authors published an article comparing several types of tissue adhesives in the treatment of inguinal hernia. That experimental work has shown high efficiency of Dermabond for closing the IHS. An explanation of this efficiency is that this tissue agent is not absorbable. The other tissue adhesives are all absorbable and may have become ineffective within months. Comparing different tissue adhesives Kato et al. 17 have shown that laparoscopic injection of octylcyanoacrylate (Dermabond) was highly effective for closing the orifice of the IHS.
In our study we used the three-dimensional polyacrylamide DAM+ for closing the internal orifice of the IHS in experimental animals. This agent is used in clinical practice for endoprothesis of the soft tissues by increasing their volume. There are some articles with good results of using this gel in bronchial surgery for endoscopic treatment of bronchial fistulas and prophylaxis and treatment of primary insufficiency of the bronchial stump after pneumonectomy,18,19
In an experimental study it was shown that polyacrylamide gel had low reactivity with the surrounding tissue. Ions of silver in DAM+ contribute to this low reactivity and reduce the risks of local inflammation.
The polyacrylamide gel is hydrophilic and consists of a backbone of polyacrylamide to which water molecules are attached. These molecules are readily exchanged with those of surrounding host tissue. Over time macrophages enter the gel and are gradually replaced by a scaffold of thin connective tissue fibers. On microscopy the site of injection was invaded by macrophages and giant cells that were gradually replaced by a network of fibrous tissue. The development of the capsule was marked within 60 days after the injection.18–20 When this hydrogel was injected into the preperitoneal space, only the formation of a fine fibrocellular capsule was observed, with macrophageal infiltration, marked vascularity, and absence of any signs of local inflammation. At the second laparoscopy, a thin layer of fibrous connective tissue was occasionally present around the gel, but the thick fibrous capsule, as seen with silicone implants, was absent. No further histopathological reaction occurred outside the implant site, such as foreign body reaction. After implantation, no local or regional migration of the gel has been observed.
Our results has show that after 6 months of DAM+ injection, closing of the internal inguinal ring was observed with no reopening in all cases. The advantages of this technique are that there is no dissection of the spermatic cord and there is no ligation of the IHS. This is a preliminary result, and although our technique appears successful experimentally, we have concerns about (1) adhesive bowel obstruction, (2) hernia recurrence, and (3) postoperative hydrocele. Particular studies require investigating local tissue reaction and long-term follow-up after the gel injection.
This study demonstrated that the biopolymeric implant gives good postoperative results and a stable trend of closing the orifice of the IHS in long-term follow-up. In conclusion, we hope that injectable bulking agents can be used for treatment of inguinal hernias in pediatric patients after additional animal and human research.
Footnotes
Disclosure Statement
No competing financial interests exist.