
Abstract
Abstract
Aim:
This study aimed to develop a novel procedure for treating long-gap pure esophageal atresia. This procedure, which entails the combined use of laparoscopy and natural orifice translumenal endoscopic surgery (NOTES), would enable primary repair without cervical and thoracic incisions and prevent postoperative gastroesophageal reflux disease (GERD).
Methods:
Nonsurvival experiments were conducted in 9 pigs to study the technical feasibility. The procedure comprised the following: (1) creation of the disease model by laparoscopic resection of the lower esophagus; (2) laparoscopic fundoplication, complete mobilization of the stomach, and enlargement of the esophageal hiatus; (3) formation of a peroral transesophageal entry site into either the postmediastinum or the right thoracic cavity followed by fashioning a tunnel to the peritoneal cavity; (4) gastric pull-up by using both laparoscopy and NOTES; (5) esophagoesophageal anastomosis using BraceBar™, a prototype of the double T-bar suturing device (Olympus Medical Systems Co., Tokyo, Japan).
Results:
Laparoscopic procedures were performed without complications. The postmediastinal tunnel was successfully created three times with a complication of pleural injury. However, gastric pull-up via this route could not be completed due to porcine anatomical reasons. Gastric pull-up through the right thoracic route was achieved five times in six attempts. Two disorientations and a hemorrhagic death occurred during the procedures.
Conclusions:
This study showed that combined use of laparoscopy and NOTES enabled gastric pull-up without cervical and thoracic incisions. Our method has the potential of lowering the incidence of GERD and enabling primary repair of this disease.
Introduction
We conceived a novel procedure that entails the combined use of laparoscopic and natural orifice translumenal endoscopic surgery (NOTES) approaches. This procedure enables primary repair without cervical and thoracic incision and would improve patients' quality of life. The aim of this study was to present early results of a series of acute animal experiments studying the technical feasibility of the procedure for long-gap pure esophageal atresia.
Materials and Methods
The protocol for this study was approved by the Animal Care and Use Committee of The University of Tokyo and Japan NOTES. Nonsurvival experiments were conducted in 9 pigs weighing approximately 40 kg. The animals were fasted from solid food for 24 hours before the procedures but were allowed full access to water. All procedures were performed under general anesthesia with a tracheotomy tube and mechanical ventilation. Chest tubes were inserted into both thoracic cavities to prevent tension pneumothorax during surgery. The pigs were placed in the prone position.
The concept of the novel procedure was based on partial gastric transposition described by Scharli. 9 Fundoplication was added to Scharli's operation; furthermore, we planned to perform the procedure by the combined use of laparoscopic and NOTES approaches. The details of the procedures were improved step by step throughout the experiments. After trial and error, we finally established the following techniques.
Laparoscopic approach
Port location
A laparoscopic operation preceded the NOTES approach. A 12-mm port was inserted for a 10-mm flexible scope at the center of the abdomen. Carbon dioxide pneumoperitoneum was created at 8 mmHg. Then, 5-mm and 12-mm trocars were placed in the right and left lateral positions, respectively, of the first trocar as working ports. A 12-mm trocar as a liver retractor was introduced just below the costal margin, and a 5-mm trocar for traction of the stomach was placed in the left upper or lower quadrant.
First, the abdominal esophagus was incised at the 5-cm proximal site from the cardia using an Endo-GIA™ (Covidien Japan, Tokyo, Japan) since this procedure was developed for treating patients with esophageal atresia. Then, the stomach was mobilized completely along the lesser and greater curvatures, taking care not to injure the vascular arcades. The short gastric vessels and the left gastric artery and vein were divided using laparoscopic coagulating shears, SonoSurg™ (Olympus Medical Systems Co., Tokyo, Japan). The blood supply of the stomach and distal esophagus was provided by the right gastric artery and the right gastroepiploic artery. After performing Nissen fundoplication, anchor sutures, which were used to pull up the stomach, were fixed at the stump of the distal esophagus. Finally, a gastric pull-up route was created after enlargement of the hiatus by dissecting both the crura. We had two options: a postmediastinal route and right thoracic route. In the case of the postmediastinal route, blunt dissection was performed through the hiatus. The right pleura mediastinalis was opened when the right thoracic route was selected.
NOTES approach
A cap-fitted single-channel endoscope (GIF-Q260J; Olympus Medical Systems Co.) was introduced perorally into the esophagus and an overtube was placed into the esophagus. Pulsation of the aortic arch was observed at the ventral part of the middle esophagus, and saline was injected into the submucosal layer at the dorsal part of the upper esophagus. An esophageal mucosal incision from the 3 O'clock to 7 O'clock position was created; then, a small hole was made in the muscle layer using a needle knife. The position of the small hole was quite important: the 6 O'clock position in the case of the postmediastinal route and the 5 O'clock position in the case of the right thoracic route. A guidewire was passed into the small hole without resistance and a 15-mm CRE™ Wireguided Balloon Dilator (Boston Scientific Corporation, Natick, MA) was introduced to enlarge the opening. The endoscope was then advanced into the postmediastinum or the right thoracic cavity through the entry site at the muscular layers of the upper esophagus. A postmediastinum tunnel to the hiatus was fashioned using CO2 insufflation and blunt dissection that was performed by advancing the endoscope. In the case of the right thoracic route, selective mainstem bronchus intubation was done preoperatively and the endoscope was introduced up to the abdominal cavity via a route dorsal to the pulmonary hilum.
In the peritoneal cavity, the sutures that were previously applied to the edge of the distal esophagus were grasped by an endoscopic grasper. Gastric pull-up was performed until the distal esophagus entered into the upper esophagus through the entry site by withdrawing the endoscope and using the laparoscope to push the stomach into the tunnel. After gastric pull-up, the anchor sutures were removed using endoscopic scissors, leaving only one thread to retract the distal esophagus toward the oral direction.
An end-to-side esophagoesophageal anastomosis was conducted using BraceBar™, a prototype of the double T-bar suturing device (Olympus Medical Systems Co.). This device was originally developed to establish endoscopic full-thickness closure of large gastric perforations. Details of the instruments were described by Sumiyama et al. 10 Thereafter, the device was improved and became easy to manipulate. A new prototype was used in this study. In short, this tissue anchoring device consists of a needle catheter with a slidable outer sheath (Fig. 1a) and a bifurcated nylon suture with three T-tags, two of which are fixed at the distal ends of the separated nylon threads and the other tag is placed at a position proximal to them (Fig. 1b). These tags and thread were loaded inside the needle catheter in advance (Fig. 2a). The needle was advanced through the scope, and all layers of the perforation site were penetrated by the needle catheter. Then, the first T-tag and thread were released out of the catheter blindly behind the gut wall (Fig. 2b), and the catheter was withdrawn into the lumen, leaving the T-tag and thread in place. Next, the other side of the perforation site was punctured, and the second T-tag was released in the same manner (Fig. 2c). After the needle catheter was pulled back into the duct, the outer sheath of the catheter was advanced and the proximal tag, which could slide over the thread, was firmly pushed to cinch the pair of T-tags (Fig. 2d, e).
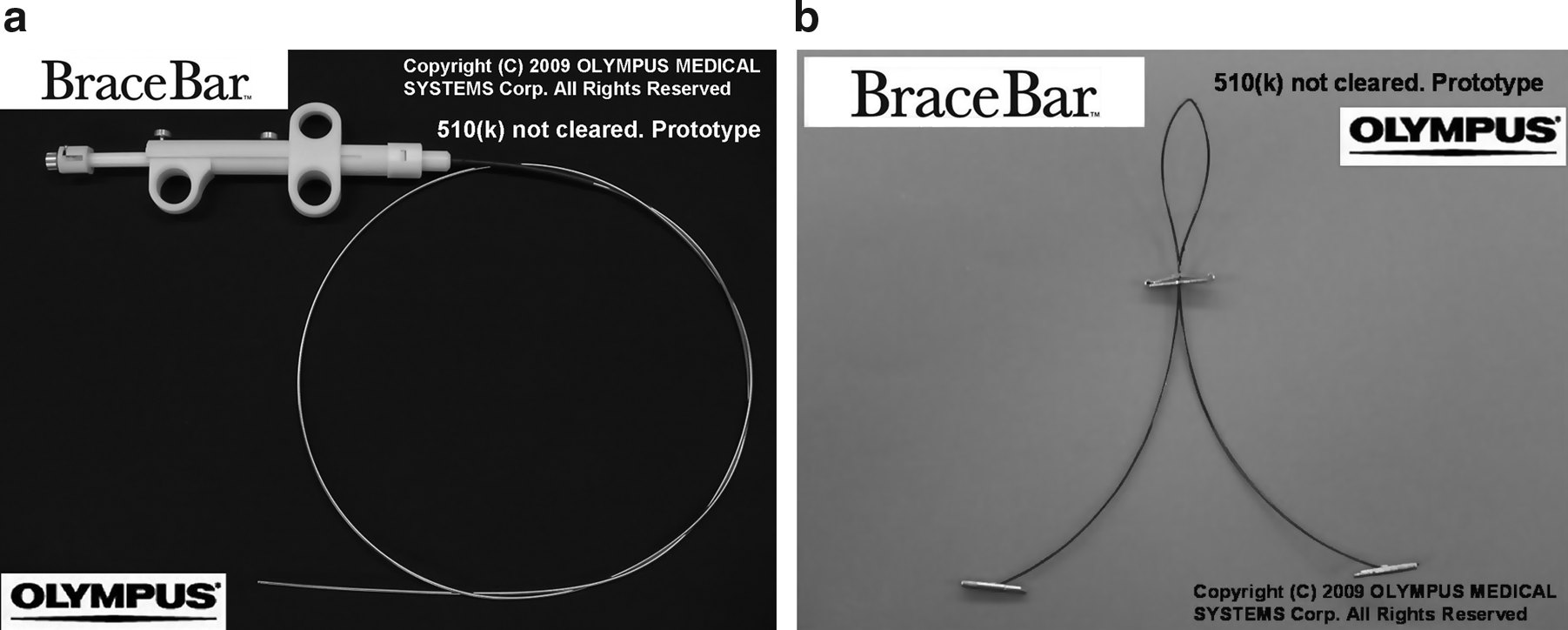
BraceBar™, a prototype of the double tissue anchoring device, consists of two parts: an applicator
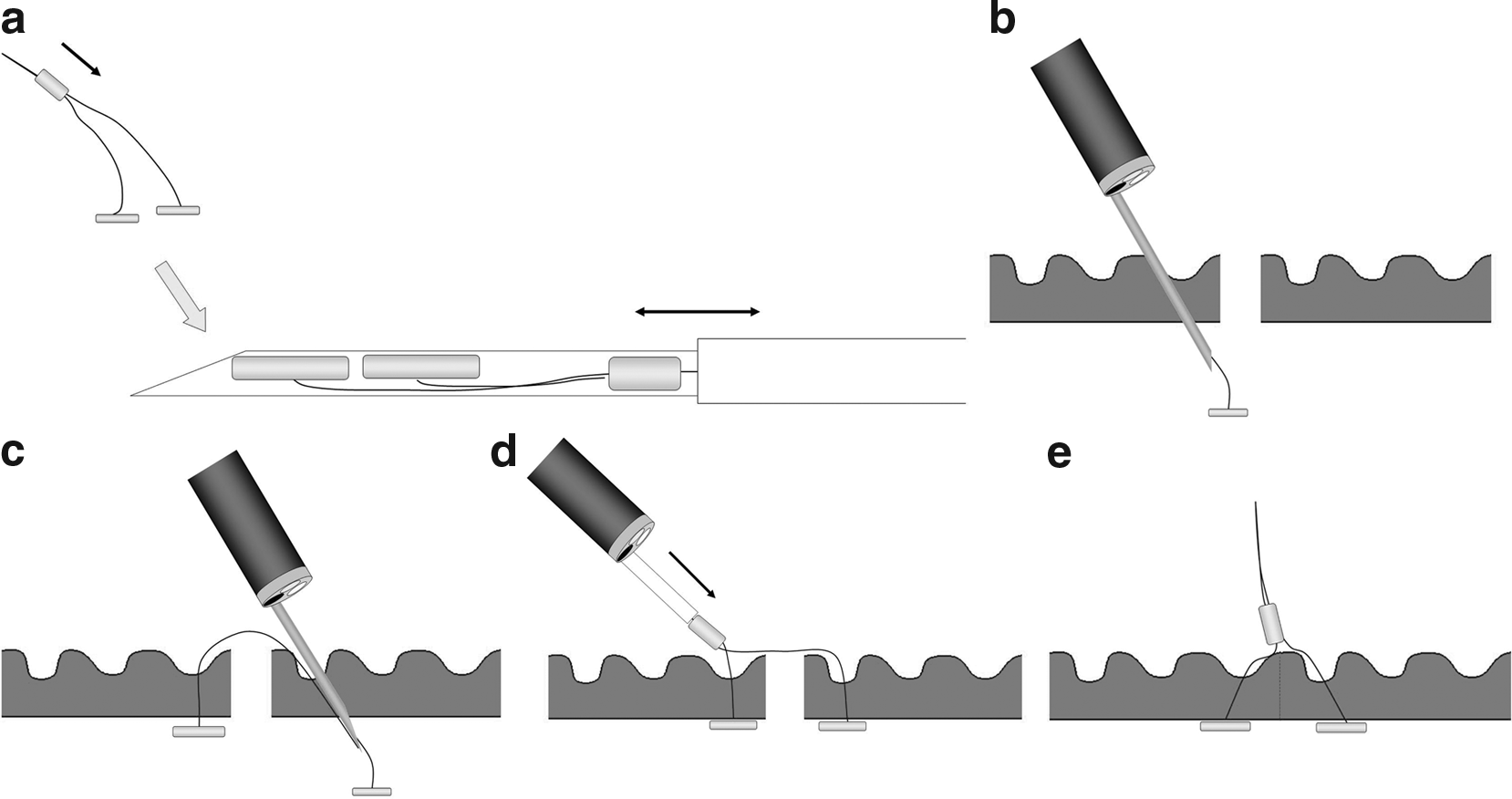
Schema of full-thickness suturing by using BraceBar.
We used this device to perform anastomosis. The full thickness of the distal esophagus, which was pulled into the upper esophagus, was punctured by the needle catheter. Next, the first T-tag was placed inside the distal esophagus and the catheter was withdrawn. Then, the upper esophagus was penetrated and the second T-tag was positioned outside the esophagus. Four sets of the T-tags and threads were used to anastomose the upper and distal esophagus. Punctures were performed under good observation by retracting the stump using an EndoLifter™ (Olympus Medical Systems Co.). Finally, the edge of the distal esophagus was grasped with an endoscopic grasper that had been advanced through the channel. Then, the stump was fastened with a snare instrument that had been introduced over the scope and was incised to open the anastomosis.
After the procedure was completed, thoracotomy was performed to evaluate the results of our procedure. The animals were sacrificed at the end of the experiments.
Results
The laparoscopic procedures were performed without any complications. The lesser curvature of the porcine stomach was much shorter than that of human. Therefore, in some cases, the hepatoduodenal ligament had to be divided to achieve complete gastric mobilization. In addition, it was sometimes necessary to elongate the stomach by dividing the lesser curvature using an Endo-GIA so that the distal esophagus could reach the upper esophagus easily.
Only the experiment on the first pig was performed under direct vision through thoracotomy to collect porcine anatomical information to perform transesophageal surgery on pigs. In addition, endoscopic ultrasonography (EUS; GF-UCT2000; Olympus Medical Systems Co.) was performed to understand the relationship between the esophagus and the great vessels. Direct entry to the postmediastinum through the upper esophagus and creation of a postmediastinal tunnel to the peritoneal cavity were achieved. Based on information obtained from the experiment on first pig, the following experiments were planned and tried without EUS and thoracotomy.
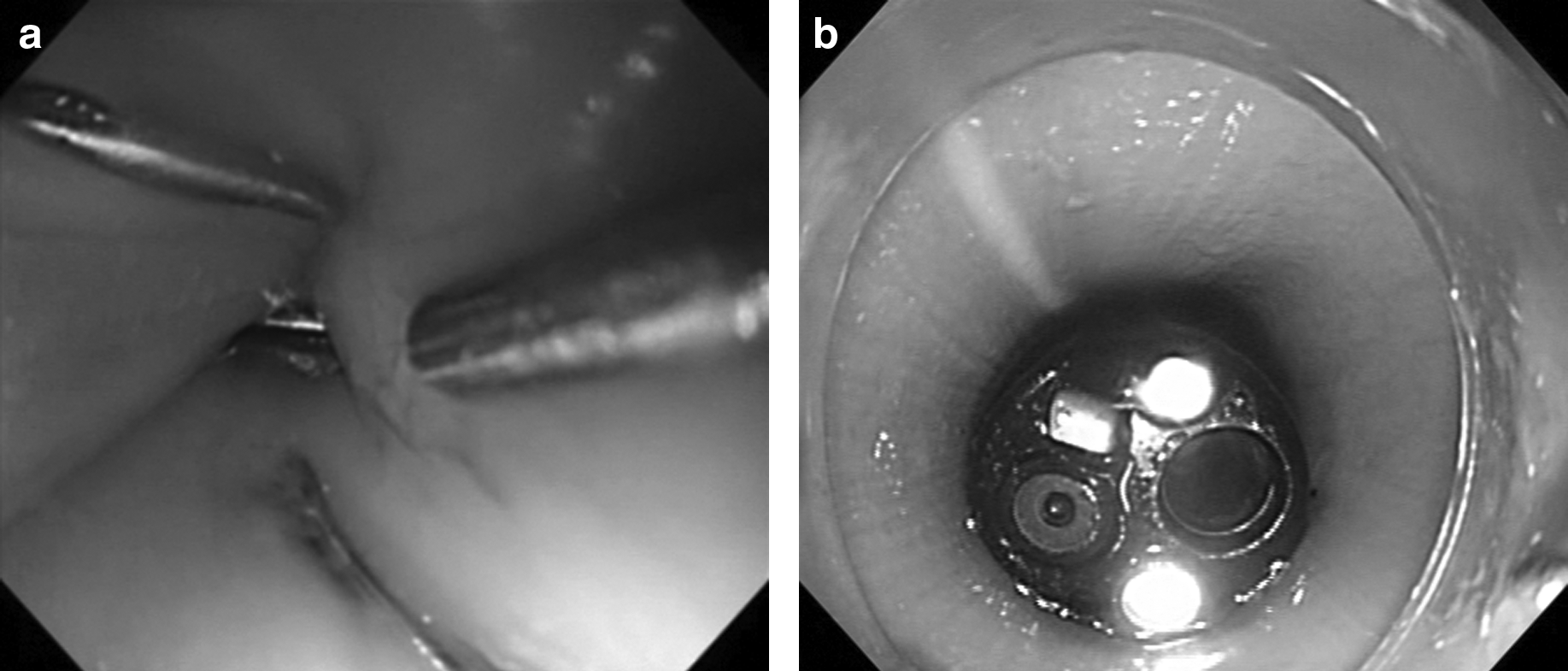
As for the route, we tried to perform gastric pull-up through the postmediastinal route three times. An entry site to the postmediastinum was successfully created each time and a postmediastinal tunnel was fashioned in 2 cases (Fig. 3a–c). The postmediastinum could easily be dissected; however, pleural injury occurred during the dissection. The cause of this complication was excessive pushing of the endoscope in the wrong direction: the endoscope was pushed not toward the peritoneal cavity but toward the pleural cavity. Postmediastinal gastric pull-up was attempted but could not be achieved. At the third trial of the postmediastinal pull-up, we arrived at the conclusion that the mediastinum of the pig was too small to confine the bulky porcine stomach; therefore, the method was intraoperatively changed to the right thoracic route and it was adopted in the experiments on the following 5 pigs. The right thoracic route was fashioned successfully with the correct entry site three times in six attempts. A hemorrhagic death due to injury of the great vessel occurred at the first attempt of the right thoracic route. In this case, the entry site was created in the middle esophagus, which is surrounded by the great vessels and was more distal than previously planned. In the other 2 cases, an entry site to the postmediastinum was unexpectedly created, because the small incision for balloon dilation was made incorrectly: failure to incise at the 5 O'clock position occurred in 1 case and incomplete full-thickness incision of the muscular layer occurred in the other case. In these cases, the postmediastinal tunnel was first formed, and a small incision was made on the right pleura mediastinalis to create an entry site to the right thoracic cavity. After balloon dilatation, the endoscope could be advanced to the right thorax. As a result, right thoracic gastric pull-up by the combined use of the laparoscopic approach and NOTES approach was achieved in five of six attempts (Fig. 3d). The only case of failure was the one in which a fatal complication occurred.
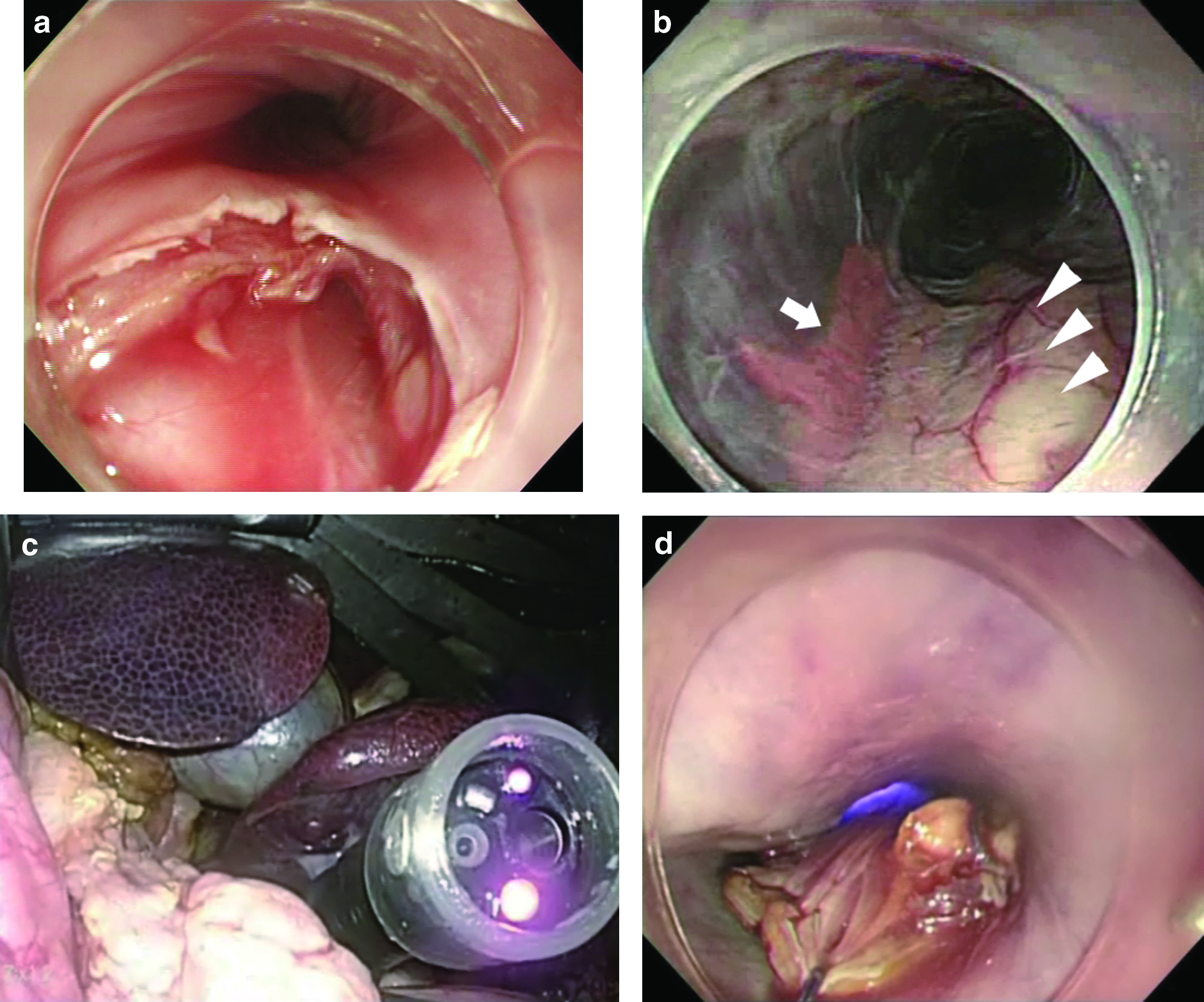
Creation of the postmediastinal route.
Esophagoesophageal anastomosis using BraceBar was attempted in experiments on 3 pigs. At the first trial, the upper and distal esophagus could be fixed by four pairs of anchoring T-tags (Fig. 4a–c). The opening of anastomosis succeeded in the second and third attempts. All punctures to the distal esophagus were performed under the observation of a transgastric endoscope that had been introduced to the distal esophagus through the trocar placed in the left lower quadrant in the second attempt of anastomosis (Fig. 5a). After completion of anastomosis, the endoscope or the guidewire was passed through the anastomosis to confirm the patency (Fig. 5b). There were no injuries to other organs during the procedure.
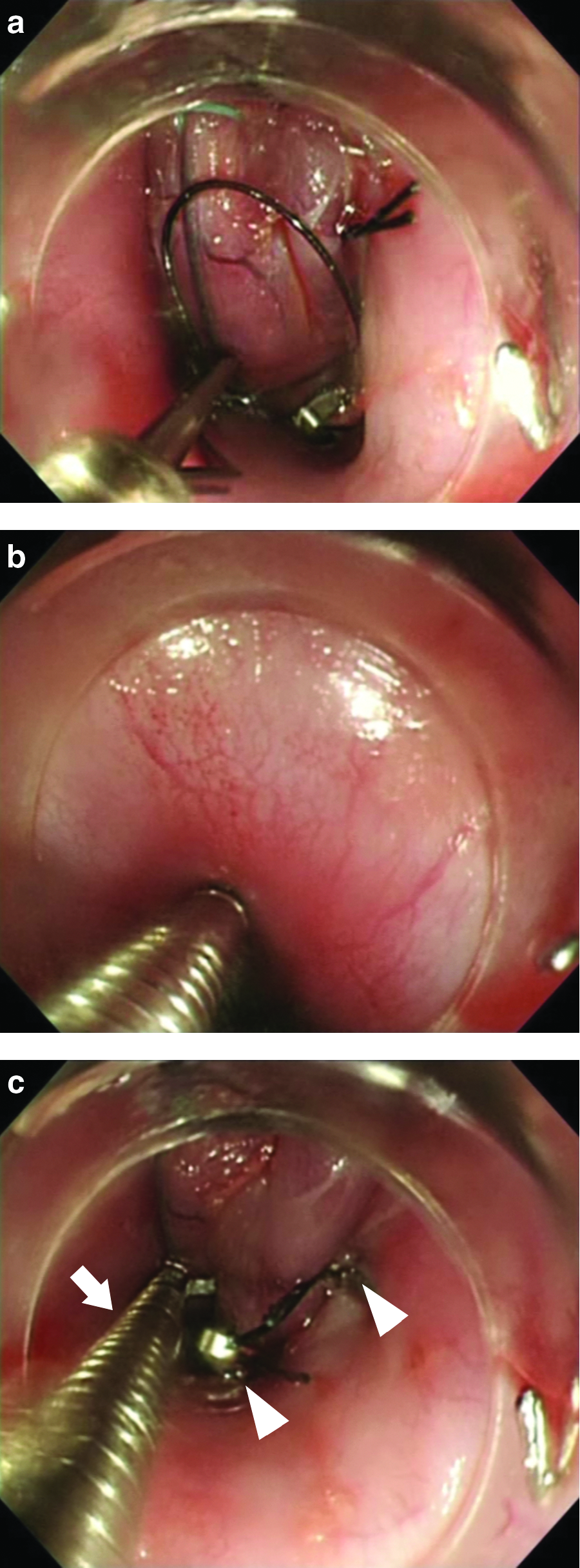
Esophagoesophageal anastomosis by using BraceBar.
The length of time of the laparoscopic surgery was constant at approximately 2 hours. In contrast, the length of time of the NOTES approach showed a steep learning curve. The shortest time of gastric pull-up from introduction of the endoscope to pulling the distal esophagus to the upper esophagus was 30 minutes and that of anastomosis from the first puncture of the needle catheter to creation of the anastomotic orifice was 37 minutes. Postmortem direct observation through thoracotomy showed that the stomach passed through a route dorsal to the hilar area (Fig. 6). A simple leak test, CO2 insufflation performed by the endoscope after filling the right thorax with saline, did not show any bubbles in the third trial of anastomosis.
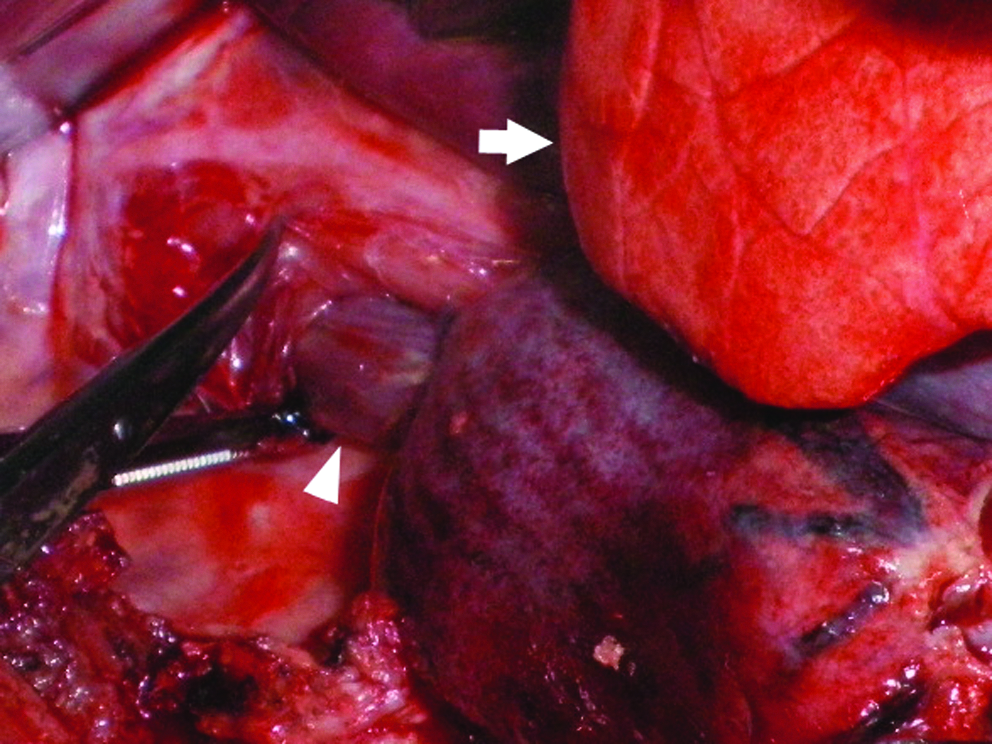
Postmortem investigation through thoracotomy (right thoracic route) showed that the stomach was pulled up behind the lung (arrow) and the distal esophagus (arrowhead) entered the upper esophagus.
Discussion
Since Kalloo et al. 11 reported the first case of NOTES, not only many animal studies but also clinical experiences have been described recently. As for the transesophageal approach, pilot studies of mediastinoscopy,12–14 mediastinal lymph node resection and transesophageal thoracoscopy with pleural biopsy,13,14 esophagomyotomy and vagotomy, 15 epicardial coagulation, 16 and Heller myotomy 17 have been published in the literature. To our knowledge, this is the first study to apply NOTES for esophageal atresia. Thoracoscopic repair 6 and laparoscopic gastric pull-up1–4,8 have been described as minimally invasive surgery for esophageal atresia. However, thoracic incisions, even when small, are painful and primary repair of long-gap cases is difficult by the thoracoscopic approach alone. A cervical incision for anastomosis in laparoscopic gastric pull-up leaves cosmetic concerns in children for a long period. Our procedure, gastric pull-up completed by using a laparoscopic approach and transesophageal NOTES approach, has the potential benefits of the absence of an upper-body scar and primary repair of long-gap pure esophageal atresia.
The concept of our procedure was based on Scharli's operation. 9 A major difference between our procedure and the gastric transposition described by Spitz 18 is that the distal esophagus is not resected. There are two reasons to leave the distal esophagus unresected. First, we believe that it is better to anastomose the upper esophagus with native distal esophagus than to anastomose it with the colon, jejunum, or stomach. Second, fundoplication can be easily performed when the distal esophagus is left in place. GERD is one of the cumbersome postoperative problems. Its incidence was reported as 15%–30%.19,20 Long-term medication impairs patients' quality of life, and an additional antireflux surgery is required in some cases. Our proposed method including concomitant fundoplication may prevent this complication.
The mucosal flap safety valve technique 10 has been widely used in the peroral transesophageal route in the literature. However, the upper esophagus of neonates with this disease is short and it would be difficult to create a submucosal tunnel. Therefore, we adopted a method of direct access method into the postmediastinum or the right thoracic cavity. The position of the entry site, both the direction and the depth, is quite important. The 6 O'clock position has to be incised to create the postmediastinal tunnel and the 5 O'clock position has to be incised to create the right thoracic route. If the direction of the entry site is differs from the respective directions, the endoscope will enter an unexpected space. There is a risk of injury to critical organs such as the great vessels or trachea if the entry site is placed in the ventral side. In addition, the depth of the entry site is very important, because incision of the middle esophagus, which is surrounded by vital organs, may result in fatal complications as we experienced. In clinical practice, surgeons would have to obtain detailed anatomical information by carefully examining computed tomography and/or magnetic resonance imaging scans before the surgery to minimize the risk. Moreover, EUS will provide important information on organs outside the esophagus.
Both tunnels to the abdominal cavity, that is, the mediastinal route and the right thoracic route, were easily created when the entry site was placed in the accurate position. Although we had planned to perform gastric pull-up via the postmediastinal route in the study, this method had to be abandoned due to porcine anatomical reasons: the narrow mediastinum and bulky stomach. Even though we selected the right thoracic route in this study, we believe that mediastinal gastric pull-up would be possible in clinical cases. We established a technique of how to fashion the mediastinal tunnel by using the NOTES approach. Many patients have undergone gastric pull-up through the mediastinum route by a combination of laparoscopy/laparotomy and cervical incision.
There are several challenges that must be overcome before NOTES can be applied in clinical practice, and bowel anastomosis is one of the most challenging and imperative assignments. Rolanda et al. 21 reported peroral esophageal segmentectomy and anastomosis using a single transthoracic trocar. To our knowledge, the present study is the first study to complete esophagoesophgostomy without thoracoscopic assistance. However, our method has room for improvement. The current device requires several steps to anchor a pair of T-tags and the endoscope has to be repositioned several times. The needle catheter has to be inserted blindly. In the second attempt of anastomosis, we could observe inside the distal esophagus during anastomosis by introducing a transgastric endoscope through a trocar placed in the left lower quadrant, but it was not possible to monitor organs outside the upper esophagus in this study. We hope that a simpler, safer, non-time-consuming device is developed for secure bowel anastomosis.
Even though end-to-end anastomosis is usually performed in clinical practice, end-to-side anastomosis was alternatively performed in this study. A model of esophageal atresia was created by interrupting the lower esophagus. However, this was not a perfect model, because the upper half of the resected esophagus was much longer than that of patients with esophageal atresia. Resecting the upper esophagus to create a perfect model would require opening of the pleura mediastinalis under thoracotomy or thoracoscopy, and opening of the pleura mediastinalis would hinder planned NOTES procedures. Although we have not yet tried end-to-end anastomosis, we consider that it can be completed by using our technique.
This study has several limitations. The sample size was small and only acute experiments were conducted. In addition, the pigs were large compared to neonates or infants with this disease. The instruments were too large to be used in neonates and infants because they were developed for adults. In spite of these limitations, our study shows the feasibility of gastric pull-up by using the combined technique of laparoscopy and NOTES. A study with a larger sample size in the survival setting will be required to verify the safety of this procedure. Smaller instruments for pediatric surgery are needed to apply this approach in the clinical setting in the future.
Footnotes
Acknowledgment
This study was supported by grants from the Ministry of Education, Culture, Sports, Science, and Technology of Japan.
Disclosure Statement
No competing financial interests exist.