
Abstract
Abstract
Solid pseudopapillary neoplasm of the pancreas in children is rare, and the most common localization of the tumor is the tail. The authors encountered such a case in a 10-year-old girl with a giant solid pseudopapillary neoplasm at the uncinate process of the pancreas. Imaging examination showed there was a distinct distance between the neoplasm and the main pancreatic duct. Using a 4-port transperitoneal laparoscopic technique, complete resection of the tumor was successfully performed. Laparoscopic approach appears to be safe and feasible in children with solid pseudopapillary neoplasm, and an organ-preservation operation can be successfully performed if there is no communication between the tumor and the pancreatic ductal system.
Introduction
Case Report
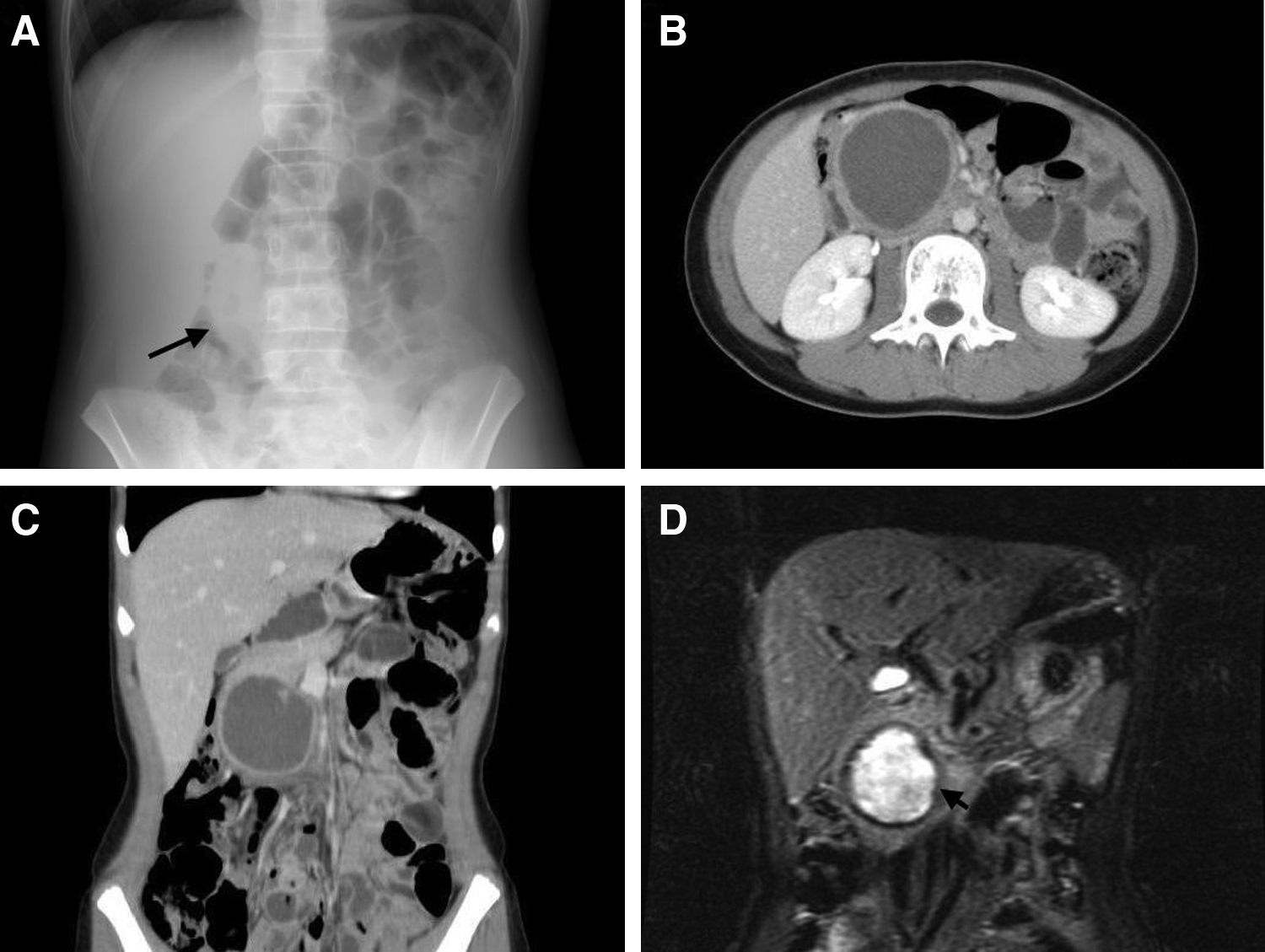
A 10-year-old girl had had recurrent episodes of mild-to-moderate abdominal fullness and feeding intolerance for the past 2 years. She was admitted with the complaint of these symptoms increasing in intensity over the recent week. The physical examination was unremarkable except for the abdominal examination. The abdomen was slightly protuberant; there was marked tenderness localized to the upper abdomen, overlying a firm, fixed mass (8×7 cm) (Fig. 1). All laboratory findings, including pancreatic function test, were normal except for a C-reactive protein of 12.08 mg/mL. The abdominal radiograph revealed prominent colonic air and a mass in the mid-abdomen (Fig. 2). A computed tomographic (CT) scan of the abdomen showed a 55×39×46 mm cystic mass over the pancreatic head. Tumor markers were as follows: carcinoembryonic antigen, 1.1 ng/mL; carbohydrate antigen (CA) 19-9, 66.67 U/mL; CA 125, 40.33 U/mL; and CA 72-4; 3.75 U/mL. Magnetic resonance cholangiopancreatography (MRCP) showed that there was a distinct distance between the neoplasm and main pancreatic duct. Therefore, an organ-preserving operation was performed, and a laparoscopic approach was elected.

Left: Port placement for the operation. Black dotted lines indicate the size and location of the tumor. Right: Aesthetic results 16 days after the operation. Some aberration of the umbilicus was noted since the tumor was delivered via the extended umbilical incision.
The patient was placed in a supine modified lithotomic position with the surgeon standing between the legs. Intraoperative endoscopic retrograde cholangiopancreatography (ERCP) was performed and showed no filling defect in the main pancreatic duct. Further, the cystic neoplasm did not fill with contrast media, which appeared to be unrelated to either the biliary or pancreatic ductal systems. Laparoscopy was performed with a 5-mm Hasson port at the umbilicus, and video laparoscopy was performed with a 5-mm 30° laparoscope (Karl Storz GmbH, Tuttlingen, Germany). Three additional 5-mm working ports were placed, one at the subxiphoid, one at the right lower quadrant, and one at the left upper quadrant (Fig. 1). The Kocher maneuver was performed to expose the pancreatic head and uncinate process (Fig. 3). The inferior vena cava, transverse colon, duodenum, and pancreas were clearly identified. The lesion was then visible between the pancreatic head and second and third portions of the duodenum above the inferior vena cava. Initially, the cystic contents were percutaneously aspirated to yield biochemical information. Bloody fluid was obtained. Although dense adhesions were present between the mass and the pancreas and the duodenum, the laparoscopic approach facilitated good visualization, and these adhesions could be divided according to different contours with the aid of a Harmonic Scalpel (Ethicon Endo-Surgery, Cincinnati, OH). Since the splenic vessels were not encountered during resection of the tumor, a spleen-sparing operation could be ensured. After the tumor had been completely mobilized, the specimen was put in an extraction bag and delivered via the extended umbilical incision (Fig. 1). No postoperative drainage was placed. Operative time was 480 minutes, and blood loss was estimated as 100 mL without blood transfusion.
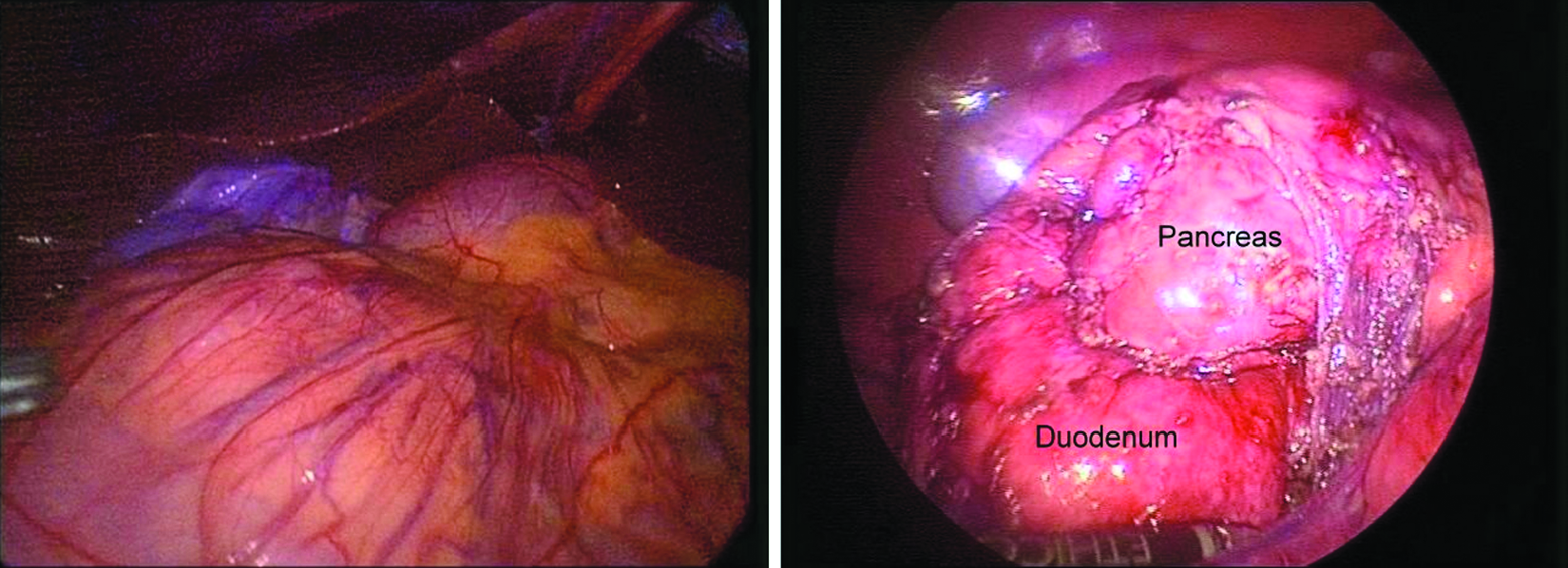
Left: Operative photograph showing a mass located behind the greater omentum. Right: After complete resection.
The specimen of aspirated cystic fluid yielded no bacterial growth, and biochemical analysis revealed an elevated amylase level (629 U/L) and high red blood cell count (37,500/mL). Histology confirmed the diagnosis of solid pseudopapillary neoplasm with hemorrhage. Macroscopically, the specimen displayed as grayish and elastic. On microscopic examination, it showed sheets of relatively uniform cells with round to oval nuclei with finely stippled chromatin and eosinophilic cytoplasm. Pseudopapillae with hyalinized cords surrounded by neoplastic cells were seen. Extensive coagulative necrosis was identified. These neoplastic cells were positive for CD10 and negative for synaptophysin, chromogranin-A, progesterone receptor, and β-catenin. The patient resumed oral intake on postoperative day 1, and she was discharged on the fourth postoperative day. There was neither recurrence up to the time of writing (20 months) nor abdominal discomfort that presented beyond the usual postoperative period. Pancreatic function tests were within normal limits.
Discussion
Solid pseudopapillary neoplasm of the pancreas, first described by Frantz in 1959, 2 is a relatively uncommon tumor, accounting for less than 1% of all pancreatic tumors, 3 and most reports are of Asian origin.4–8 It typically affects young women with a reported male/female ratio of approximately 1:10, and usually has nonspecific clinical manifestations. 9 In a large review of 718 solid pseudopapillary neoplasms of the pancreas, the most common localization of the tumor was the tail (35.9%), whereas the uncinate process of the pancreas was the least likely location (0.43%, only 3 cases). 9 Although previously considered benign, the tumor is currently considered a low-grade malignant epithelial neoplasm with low metastatic rate and high overall survival.
Sonography and CT scan are the mainstay of imaging modalities in the detection and diagnosis of the neoplasm and usually show a large well-encapsulated lesion with mixed solid and cystic components in various proportions.6,7 However, the features of the tumors on MRI are not well described. 7 On ERCP, the relationship between the tumor and the pancreatic ductal systems could be seen, thus providing information about optimal treatment protocols. 9
In approximately 85% of patients, solid-pseudopapillary neoplasm is limited to the pancreas, whereas about 10% to 15% of tumors have already metastasized at the time of presentation. 10 Surgery is advocated in all cases. However, there has been much controversy on the surgical procedure for the treatment of solid-pseudopapillary neoplasm. 8 Aggressive en bloc resection is typically curative in patients with local extension or concomitant metastases, or in patients without a definitive preoperative diagnosis. 6 However, unlike other childhood pancreatic neoplasms, the prognosis after complete surgical resection is quite favorable, and tumor recurrence is relatively rare. 5 In the present case, MRCP showed that there was a distinct distance between the neoplasm and the main pancreatic duct. On ERCP, there was no contrast media filling in the cystic neoplasm. Neither displacement nor disruption of the main pancreatic duct can be seen. Since its low metastatic potential, an organ-preservation operation is advised in the present case with localized disease in order to provide a relatively good quality of life. 11 Therefore, a simple tumor enucleation instead of pancreaticoduodenectomy was performed.6,8,9,11,12
With refinements in minimally invasive surgery, laparoscopic surgery can be safely applied to benign or low-grade malignant tumors of the pancreas.4,13 On reviewing the literature from 1953 to 2010, operations on only 5 such children with solid pseudopapillary neoplasms have been successfully performed; all arose in the body and/or tail and had a spleen-preserving distal pancreatectomy.5,14–16 Recently, laparoscopic resection of uncinate process of the pancreas has been reported in an adult. 11 This, however, appears to be the first report of complete laparoscopic excision of a solid pseudopapillary neoplasm of uncinate process of the pancreas in a child. Despite the present case representing experience within the learning curve and time-consuming operation, the laparoscopic approach holds promise for providing advantages seen with minimally invasive approaches in other procedures, such as postoperative recovery and cosmetic considerations (Fig. 1). 17 The operation time may also be prolonged because of intracystic hemorrhage before the operation and dense adhesions between the tumor and surrounding tissues.
This case presents a relatively uncommon clinical problem and is the first case report of successful laparoscopic management in a child with a solid pseudopapillary neoplasm of uncinate process of the pancreas. Laparoscopic pancreatic resections appear to be safe and feasible in children with solid pseudopapillary neoplasm, and an organ-preservation operation can be successfully performed if there is no communication between the neoplasm and the pancreatic ductal system.
Footnotes
Disclosure Statement
No competing financial interests exist.