
Abstract
Abstract
Background:
Minimally invasive procedures for inflammatory bowel disease have been shown to improve recovery in children. We report our initial experience with single-incision laparoscopic operations for pediatric intestinal disease.
Methods:
We retrospectively reviewed 12 procedures in 11 patients (4 women) from March 2010 to January 2011. Procedures were conducted by using standard laparoscopic instruments.
Results:
Mean age was 15 years (9–17 years). Procedures included three total abdominal colectomies, four two-stage ileal-pouch anal anastomosis (IPAA), two single-stage IPAA, two three-stage IPAA, and one ileocectomy. An accessory umbilical port was used in 6 cases. Mean operating time was 287 minutes. Mean length of stay was 4.1 days (3–9 days). Postoperative complications have occurred in 5 patients (42%). Anastomotic leak occurred in 2 patients with IPAA without protective ileostomy, 1 operative small bowel obstruction, 1 pelvic abscess and portal vein thrombosis, and 1 readmission for dehydration. Both patients who had leaked have recovered well and had their stomas reversed. Mean follow-up is 190 days. Average number of daily bowel movements is 4.5. Pouchitis has occurred in 50% (4/8) of patients.
Conclusions:
Single-incision laparoscopic surgery for pediatric intestinal disease is safe and feasible by using standard laparoscopic instruments. We do not advocate IPAA without a stoma due to the high rate of anastomotic leak. Continued experience will shorten operative times and reduce complications.
Introduction
Materials and Methods
After IRB approval, we performed a retrospective review of all patients who underwent intestinal resection by using single-incision laparoscopic surgery at our institution from March 2010 to January 2011. All patients were evaluated in our multidisciplinary inflammatory bowel disease clinic and recorded in a prospective case log. Demographics, perioperative events, and postoperative outcomes were recorded. Standard follow-up consisted of scheduled clinic visits and regular discussions via telephone or electronic mail. All data were entered in an electronic spreadsheet (Microsoft Excel) to calculate the descriptive statistics utilized for this study.
Total abdominal colectomy
In a supine position, single-site access was created at a predetermined ileostomy site. During our initial experience, the rectosigmoid colon was mobilized and divided with a stapler. Dissection progressed in a left to right fashion. Most recently, the dissection was started with the right colon and progressed to the rectosigmoid. The gastrocolic ligaments followed by the colonic mesentery are sequentially divided with LigaSure (Covidien, Mansfield, MA). We have found that progressing from the right to the left simplifies the division of the mesentery and omentum due to the mechanics of a right lower quadrant port (Fig. 1). Once the colon is mobilized and divided, then it is exteriorized through the ileostomy port, and a stoma is fashioned.
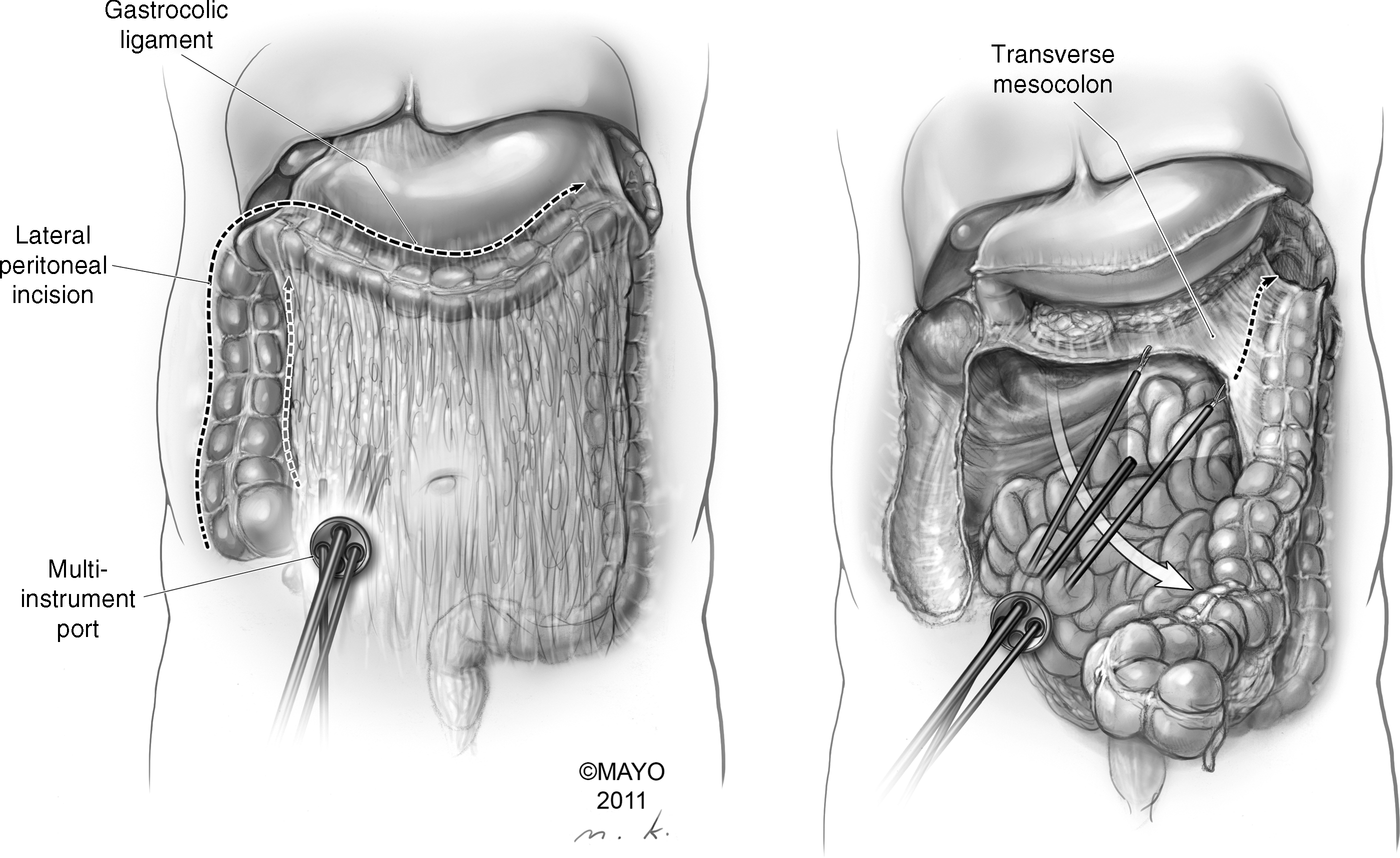
An artistic depiction of the mobilization and division of the gastrocolic ligament and colonic mesentery in a right to left direction. The left panel demonstrates the lateral mobilization and division of the gastrocolic ligament. The inner dashed line represents the initial division of the ascending colonic mesentery to the level of the duodenum. The right panel illustrates the division of the transverse mesocolon. This is most easily accomplished by retracting the colon to the left lower quadrant and viewing the mesentery from “over the top” of the transverse colon. This allows visualization of the supra-colic organs and the small intestine in the infra-colic compartment.
Proctectomy and IPAA
Proctectomy may immediately follow total abdominal colectomies (TAC) or proceed in a delayed fashion depending on the patient's preoperative condition. If pouch creation has been delayed, then the end ileostomy is taken down, and a single-incision access device is placed through the ileostomy site. The small bowel mesentery is lengthened by dividing the retroperitoneal attachments to the base of the superior mesenteric artery, and a 12–15 cm ileal pouch is created through the ileostomy site. An anvil of an EEA stapler (Covidien) is placed if a double stapled technique is planned. Once the pouch has been returned to the abdomen, then proctectomy is completed by using either LigaSure (Covidien) or Harmonic Scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH). Pelvic nerves and ureters are protected by performing this dissection close to the bowel wall. For stapled anastomoses, the rectum is everted through the anus and divided with a linear stapler 1–2 cm above the dentate line. The IPAA is completed by using a circular stapler under laparoscopic guidance. This anastomosis is facilitated by placing extracorporeal suspension sutures in the cut edges of the peritoneal reflection (Fig. 2). Mucosectomy is used for patients with familial adenomatous polyposis or patients too small to accept an EEA stapler transanally. Traditionally, a diverting ileostomy is not used in patients with familial adenomatous polyposis (FAP) and select inflammatory bowel disease (IBD) children.

A medical illustration of the exposure provided by the pelvic suspension sutures. Suture on a large taper needle is passed through the abdominal wall to suspend the cut edge of the peritoneal reflection. This obviates the need for an additional instrument to retract deep in the pelvis.
Ileocectomy with primary ileocolostomy
One patient underwent completion ileocectomy with primary anastomosis after resection of a perforated ileum and end ileostomy at an outside institution. The left lower quadrant ileostomy was taken down, and a single-site access device was created by using an Alexis wound retractor (Applied Medical, Rancho Santa Margarita, CA) and a surgical glove. The mesentery was divided by using LigaSure. A stapled side-to-side functional end-to-end anastomosis was intracorporeally created with the enterotomy closed through the stoma site by using running absorbable sutures.
Single-site access devices
A variety of single-incision ports were utilized. The Gelpoint device (Applied Medical) was used in 6 patients, a Quadport (Olympus America Inc., Center Valley, PA) in 4 patients, a Triport (Olympus) was used in 1, and a “glove port” made from a small Alexis wound retractor (Applied Medical) and a surgical glove were used in the ileocectomy. Currently, we use the “glove port” for all single-incision colectomies.
Follow-up
Diverting stomas are closed at approximately 2 months after IPAA, following a fluoroscopic study of the pouch to evaluate for anastomotic leak, fistula, or stricture. All patients are seen in pediatric surgery clinic 2–4 weeks after discharge from the hospital. Routine follow-up is then conducted by telephone or electronic mail. Additional visits to the pediatric surgery clinic occur at 1 year after ileostomy closure or sooner if the clinical situation deems necessary. We defined pouchitis as an acute worsening in bowel function associated with abdominal pain, lethargy, or fever. Anal examination and pouch endoscopy are routinely performed with a second bout of pouchitis.
Results
We preformed 12 procedures on 11 patients (4 women). Mean age was 15 years (9–17 years). Six patients were diagnosed as having ulcerative colitis, 2 as having Crohn disease (1 colonic, 1 ileocolonic), 2 as having familial adenomatous polyposis, 1 as having ulcerative colitis and juvenile polyposis, and 1 as having indeterminate colitis. The most common indication for operative intervention was failure of maximal medical management (8 patients), whereas 2 pouches were created for cancer prophylaxis, and 1 patient had perforated Crohn disease. Only the 2 patients with familial adenomatous polyposis were not receiving preoperative medications. Of the 9 patients with inflammatory bowel disease, 8 were taking steroids, 7 had received anti-TNF agents, 5 had received 6-mercaptopurine, and 4 were using 5-ASA products. Two patients required preoperative total parenteral nutrition for failure to thrive, 2 patients had autoimmune hepatitis, 1 patient had primary sclerosing cholangitis, 1 patient had idiopathic thrombocytopenic purpura, and 1 patient had juvenile polyposis in addition to ulcerative colitis. Mean body mass index was 20.5 kg/m2 (16.4–25.8 kg/m2).
Total proctocolectomy with IPAA and diverting ileostomy (two-stage IPAA) was performed in 4 patients, TAC with end ileostomy in 3 patients, total proctocolectomy with IPAA and no ileostomy (one-stage IPAA) in 2 patients, completion proctectomy with IPAA (three-stage IPAA) in 2 patients, and completion ileocectomy with primary ileocolostomy was completed in 1 patient. One patient in the three-stage IPAA group underwent a laparoscopic TAC and splenectomy for ideopathic thrombocytopenic purpura (ITP) 6 months before the single-incision completion proctectomy with IPAA. Concomitant procedures included a single-incision cholecystectomy in 1 patient and a single-incision laparoscopic high ligation and cauterization of an indirect inguinal hernia in a woman. Mean operative time was 287 minutes (168–394 minutes). Shortest operative times occurred in the ileocectomy patient at 168 minutes, followed by TAC at 254 minutes, then one-stage IPAA at 300 minutes, three-stage IPAA at 304 minutes, and finally, two-stage IPAA at 327 minutes. Mean blood loss was 60 mL (20–150 mL). No patient received a blood transfusion postoperatively. Of the 8 patients undergoing IPAA, 6 anal anastomoses were double stapled, and 2 were hand sewn after mucosectomy.
The mean skin incision was 2.7 cm (1.5–4 cm), and the mean fascial incision was 4.2 cm (3–5 cm). The largest incisions are the result of ileostomy takedown in a three-stage IPAA or the completion of ileocectomy. Currently, we make our skin incision a 1.5 cm circle at the site of the ileostomy and the fascial incision 3 cm to accommodate the extracorporeal creation of the pouch. Accessory ports were used in 6 operations (5 IPAA and 1 TAC). All ports were placed through the umbilicus, and these incisions were invisible in postoperative follow-up (Fig. 3).

Photograph of a patient 1 month postoperative ileostomy takedown for a two-stage ileal-pouch anal anastomosis (IPAA). A 5-mm umbilical accessory port was used for the total proctocolectomy and IPAA. The umbilical incision is essentially undetectable.
Mean length of stay was 4.1 days (3–9 days). Clear liquids were started on the evening of surgery, and diet was advanced to regular the following day if the ileostomy was functioning. Intravenous narcotics were used for approximately 1 day (range 1–7 days, mode 1 day). Two patients were dismissed from the hospital without the need for oral narcotics.
Postoperative complications have occurred in 5 patients (42%). Anastomotic leak occurred in 2 patients with IPAA without diverting ileostomy, one small bowel obstruction necessitating early stoma takedown, one pelvic abscess and portal vein thrombosis in a patient undergoing TAC, and one readmission for dehydration in a patient with diverting ileostomy. The small bowel obstruction was the result of an omental sling wrapped around the ileostomy. This patient underwent early stoma closure at 20 day post-IPAA after a normal contrast study of the pouch. Both patients with anastomotic leak underwent diverting ileostomies with one requiring percutaneous drain placement. The patient who required drain placement was readmitted on postoperative day 6 when she developed vomiting, abdominal pain, and fever. She remained in the hospital for 14 days after drain placement. The other patient required a total of 9 days in the hospital. Both patients who leaked had their diverting stomas reversed. The patient with the pelvic abscess after TAC required percutaneous drainage and 3 months of subcutaneous heparin for the portal vein thrombosis. Hypercoagulable work-up has been negative. He is currently thriving with his ileostomy and awaiting repeat evaluation for indeterminate colitis.
Bowel function of the patients with IPAA has been closely followed after ileostomy reversal. One patient is awaiting ileostomy takedown and was not included in the analysis, thus leaving 8 patients with a functioning IPAA. Mean follow-up is 190 days (65–292 days) after ileostomy closure. The mean number of daily bowel movements is 4.5 (3–8). Two patients report rare incidences of night-time stooling (1–2 times per month). One patient reported a single occasion of stool incontinence not requiring a pad. One patient receives fiber in supplemental gastrostomy tube feeds, thus resulting in eight bowel movements per day. Four patients have reported at least one episode of pouchitis requiring therapy (50%). Two patients have had three episodes, 1 had two episodes, and 1 had a single episode. With regard to the 2 patients who leaked, 1 reports 3 daily bowel movements with no night-time stooling and no pouchitis. The other reports 8 day time and occasional night-time bowel movements. She has been treated twice for presumed pouchitis with improvement in her symptoms.
Discussion
Surgical management of pediatric intestinal disorders is an integral component to restore health and quality of life in this particularly ill cohort of children. Decades of research and experience has allowed gastroenterologic specialists to adequately treat, and even cure, many of these patients. Surgeons have made significant contributions by reducing the morbidity of the operations required to remove affected bowel. The wide acceptance of laparoscopic procedures has been shown to be safe and improve recovery in these patients. Recently, single-incision laparoscopic surgery has been used in an attempt to again improve the postoperative recovery of our patients. This study reports the results of the first 11 patients who have undergone single-incision intestinal surgery for inflammatory bowel disease and polyposis syndromes at our institution.
Five of our patients (42%) have experienced early postoperative morbidity including 2 anastomotic leaks. Although our leak rate is high, the overall complication rate is similar to other reports.13–18 Indeed, an earlier report from our institution 13 reported a 31% complication rate, whereas other groups reported complication rates between 27% 15 and 64%. 2 A recent analysis of laparoscopic procedures in 136 children with inflammatory bowel disease 2 reported an early morbidity of 27% in patients undergoing small bowel resection and 62%–64% morbidity in children undergoing pouch procedures. The most concerning finding in our study was the two anastomotic leaks. Our previous report 13 found a 5% leak rate. Additionally, a recent study demonstrated a leak rate of 3% in 64 children undergoing single-stage IPAA. 19 Although the difference in leak rates may be explained by the single-incision technique, an alternative explanation is our change to a stapled ileal anal anastomosis. After our review of these data, we recommend a protective ileostomy in all patients with a stapled ileal anal anastomosis regardless of the surgical approach.
When examining our operative times, they are on par with other reports for laparoscopic-assisted 2 or laparoscopic colon and rectal surgery. 13 We used an accessory port in six operations, which sped the operations along. This accessory port eased the transition from three separate laparoscopic ports to two working instruments through a single site. We strongly feel that adding an additional port in the umbilicus does not decrease the cosmetic benefit of single-site surgery and definitely improves the safety of these complex resections. Although our comfort with the single-site two instrument procedure has increased, we will not hesitate to use an umbilical port if needed.
Our length of stay and intravenous narcotic use was short. We believe this is because of the multimodal analgesia that can be utilized with single-incision surgery. We are able to widely anesthetize the incision site with local anesthesia, which decrease the need for early postoperative narcotic use. Thereafter, scheduled acetaminophen and non-steroidal anti-inflammatory medications are able to control postoperative pain well. We are currently investigating the use of regional transversus abdominis plane blocks to determine whether the use of postoperative narcotics can be further reduced.
Postoperative bowel function has been excellent in our patients, including the 2 patients with anastomotic leak. The reported continence, daily bowel movements, and night-time bowel movements are similar to other studies.13–17 Pouchitis continues to be a significant problem as demonstrated in this article and the published experience. Our 50% incidence is also similar to other reports.
In conclusion, we report a large series of children who have undergone single-incision laparoscopic surgery for inflammatory bowel disease and polyposis syndromes. Our operative times, length of hospital stay, postoperative morbidity, short-term bowel function, and rates of pouchitis are similar to open, laparoscopic-assisted, and laparoscopic colon and rectal surgery in children. We do not advocate single-incision restorative proctocolectomy without protective ileostomy due to the high rate of anastomotic leak. With further experience, we believe that operative times and postoperative morbidity will decrease.
Footnotes
Disclosure Statement
No competing financial interests exist.