
Abstract
Abstract
Background:
The benefit of single-incision multiport laparoscopy (SIMPL) remains a matter of vivid discussion. For good reason it has been speculated that SIMPL causes more postoperative pain, because a minilaparotomy is required to place the multiport system. We prospectively evaluated postoperative pain scores and requirement of analgesic medication following conventional laparoscopic (CL) versus SIMPL appendectomy in children.
Methods:
The access for laparoscopic appendectomy was decided upon the surgeon's preference. Between April and October 2010, individual abdominal pain scores at 8, 16, 24, 48, and 72 hours postoperatively as well as the incidence of umbilical or shoulder pain and the total amount of peri- and postoperative analgesics, operative time, length of hospital stay, and demographics were assessed. Analgesics (paracetamol and/or metamizole, 15 mg/kg body weight) were administered regularly or on inquiry of the patient. Data are presented as means±standard deviation tested at a significance level of P<.05.
Results:
All operations were laparoscopically completed without conversion or addition of extra ports. Thirty-nine patients (8 SIMPL appendectomy) at a mean age of 12.3±2.4 years and a mean body mass index of 19.16±3.2 kg/m2 were included. Equal operation times were observed (SIMPL: 68.5±19.9 minutes versus CL: 66.2±19.5 minutes). There were no significant differences for the individual pain scores or the incidence of umbilical and shoulder pain between study groups. The total amount of required analgesic medication was significantly lower after SIMPL appendectomy (SIMPL: 65.73±43.8 mg/kg versus CL: 106.39±46.4 mg/kg, P=.04).
Conclusion:
In summary, the present study substantiates the evidence that SIMPL appendectomy in children and adolescents is not only feasible but also beneficial for the patient without translation into increased postoperative pain. Presently, we are conducting a randomized, blinded study to validate these findings.
Introduction
Intuitively, it has been implied that the patient benefits from SIMPL, because one incision should cause less pain, a faster convalescence, and better cosmetic results.4–6 On the other hand, working through one access only might compromise the performance of the surgeon, especially when the instruments cause clashing, crowding, and crossing. 7 With negotiation of technical drawbacks and increasing surgical experience,8,9 single-surgical access techniques have recently found their way into pediatric surgery with promising results.7,10,11 However, important phenomena have not been carefully investigated yet.
The aim of the present study was to evaluate individual postoperative pain and requirement of analgesic medication in a homogenous cohort of children undergoing SIMPL versus conventional laparoscopic (CL) appendectomy.
Materials and Methods
A prospective study of patients older than 4 years undergoing laparoscopic appendectomy for acute appendicitis or right lower quadrant pain was conducted between April and October 2010. Patients with pre- or intraoperative signs of perforation or an intraabdominal abscess were excluded to standardize the degree of inflammation. Both surgical access techniques were explained to the parents in detail and written consent was obtained. Data collected from medical reports included demographics (age at surgery, gender, and body mass index [BMI]), perioperative findings (mode of anesthesia, local anesthesia for trocar insertion, conversion of the technique, operative time, and histological and microbiological examination), as well as the postoperative course (duration of stay).
Data analysis was performed using JMP 7 software (SAS Institute, Cary, NC). After testing continuous data for normal distribution, either the two-sided t-test or Mann–Whitney U test was applied. For nominal data, contingency tables and Fisher's exact test analyses were used. Significance level was set as P<.05. Data are presented as means±standard deviation if not differently indicated.
Surgical technique
Perioperative anesthesia was standardized for both groups. The access for laparoscopic appendectomy was decided upon the surgeon's preference. Conventional appendectomy was usually performed by a resident under the supervision of an attending physician in a three-trocar technique, placing a 12-mm trocar (to retrieve the specimen) with a 5-mm scope transumbilically and two 5-mm working trocars in the midline of the lower abdomen and the left lower quadrant. For SIMPL appendectomy, which was performed or supervised by an attending surgeon who is very experienced in single-incision techniques, a multichannel TriPort System (Advanced Surgical Concepts, Bray, Ireland) was introduced through a 12–15-mm transumbilical incision. Five-millimeter double prebent graspers (Olympus, Hamburg, Germany) were used for dissection. In both techniques, the appendix was mobilized with a straight electrocautery instrument (BiClamp; ERBE Elektromedizin GmbH, Tübingen, Germany) and divided at its base using an endosurgical stapler (Endopath, ETS Endoscopic Linear Cutter; Ethicon, Norderstedt, Germany). Because of the inconsistency in performing surgeons, there was some variability in the technique. 12 Standard reusable laparoscopic equipment sets were used for both techniques. The use of the disposable TriPort System (Advanced Surgical Concepts) added additional costs of 335 Euro per SIMPL operation.
Pain management and documentation
Postoperative pain treatment consisted of intravenous and/or oral administration of paracetamol or metamizole (15 mg/kg body weight [BW]) regularly and on request by the patient. Regular medication was usually applied for the first 24–48 hours and reduced to an on-demand administration based on the individual postoperative pain. The total amount of administrations and dosage (mg/kg BW) per drug were recorded for every patient. Depending on the patients' age and compliance, a visual analog scale (VAS) or a faces pain scale (FPS) ranging from “no pain at all” (equaling VAS: 0/FPS: 1) to “worst possible pain” (VAS: 10/FPS: 6) was used to score individual pain at 8, 16, 24, 48, and 72 hours postoperatively. Values assessed by FPS were transformed into VAS to allow an interscale comparison according to the following formula:.
Results
Between April and October 2010, a total of 52 patients underwent surgery for an acute appendicitis or right lower quadrant pain. Thirteen patients were excluded from the study for (1) age ≤4 years (n=2), (2) increased inflammation such as perforation (n=9) or Douglas abscess (n=1), and (3) another applied technique (transumbilical laparoscopic-assisted appendectomy, n=1).
Demographics
Twenty-two girls and 17 boys were included in the study. Mean age at surgery was 12.3±2.4 years (range: 7.6–17.4 years). Mean BMI was 19.16±3.2 kg/m2 (range: 14.3–31.5 kg/m2) corresponding to a BMI percentile of 55.9%. There were no significant differences in gender, age at surgery, BMI, or BMI percentile for SIMPL and CL appendectomy, respectively.
Peri- and postoperative findings
All operations were laparoscopically completed without conversion or addition of extra ports. Histological examination revealed 33.3% early acute, 64.1% ulcero-phlegmonous, and one chronic appendicitis. Mean operation time was 66.4±19.3 minutes (range: 32–127 minutes) and did not differ between study groups (CL: 66.2±19.5 minutes versus SIMPL: 68.5±19.9 minutes). A greater incidence of postoperative vomiting was observed after SIMPL compared with CL appendectomy (25.0% versus 8.3%; data did not reach the level of statistical significance). The mean duration of hospital stay after surgery did not differ between groups (CL: 3.68±1.3 days versus SIMPL: 3.63±1.2 days).
Individual postoperative pain scores and required analgesics
Individual pain scores showed no significant differences of individually assessed pain after conventional laparascopic and SIMPL appendectomy after 8, 16, 24, 48, and 72 hours (Table 1 and Fig. 1). About half of the children reported at least once shoulder pain and in >70% umbilical pain, irrespective of the surgical technique (Table 1).
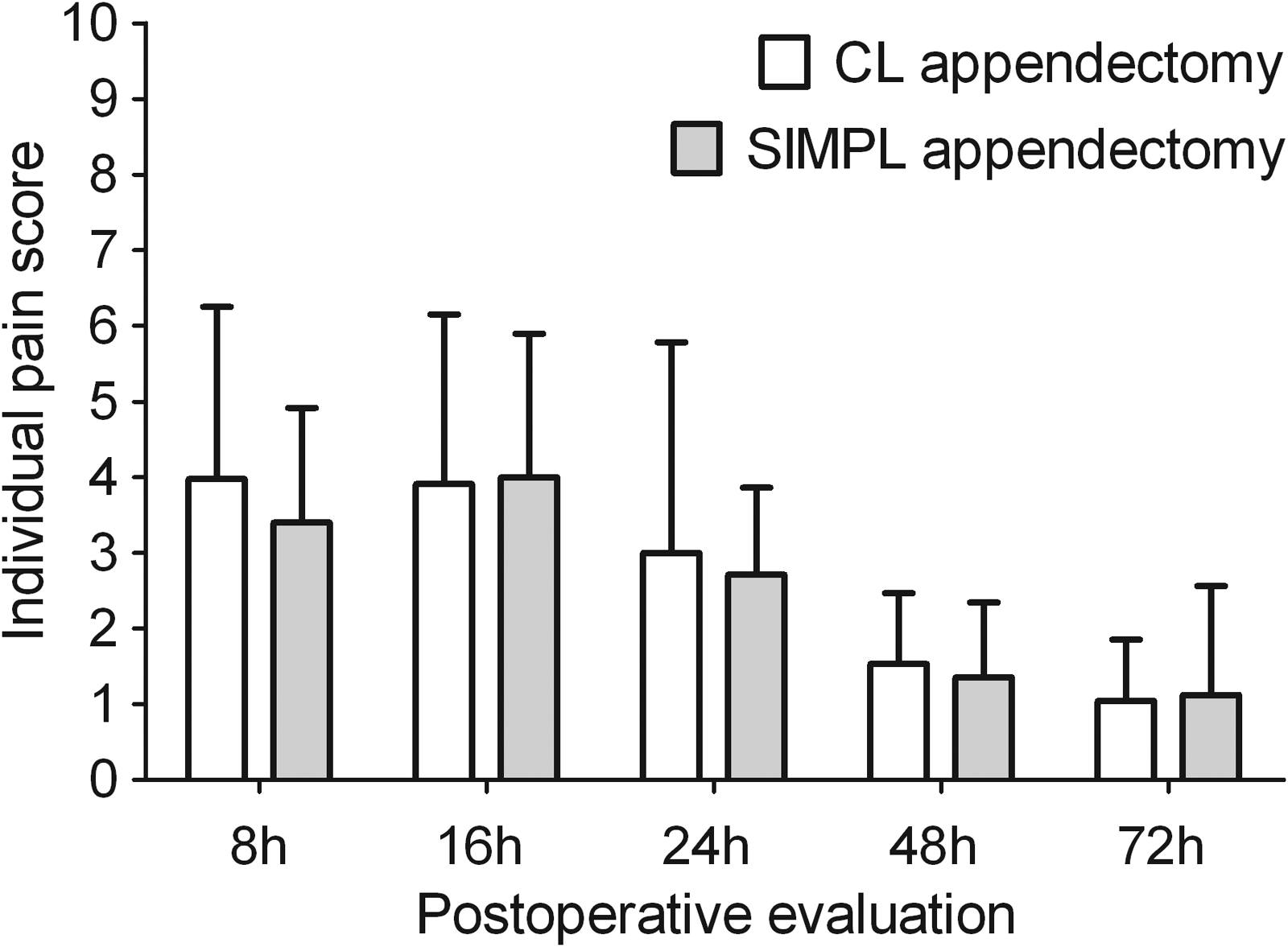
Individual postoperative pain scores at 8, 16, 24, 48, and 72 hours did not differ after single-incision multiport laparoscopic (SIMPL) versus conventional laparoscopic (CL) appendectomy.
CL, conventional laparoscopic; SIMPL, single-incision multiport laparoscopy; ns, nonsignificant.
The total amount of administered analgesics was significantly lower after SIMPL than conventional laparoscopic appendectomy (SIMPL: 65.73±43.8 mg/kg versus CL: 106.39±46.4 mg/kg, P=.04; Fig. 2). Similarly, the quantity of applied analgesics was lower after SIMPL appendectomy, even though this did not reach significance (SIMPL: 4.75±3.3 versus CL: 7.33±3.0, P=.06). However, the requirement of analgesics remained unaltered in patients who suffered acute abdominal pain (SIMPL: 72.15±39.1 mg/kg versus CL: 106.39±46.4 mg/kg). On the contrary, the quality of abdominal pain (acute/chronic) did not affect the total requirement of analgesic medication (acute: 102.48±46.4 mg/kg versus chronic: 59.32±51.4 mg/kg, P=.09).
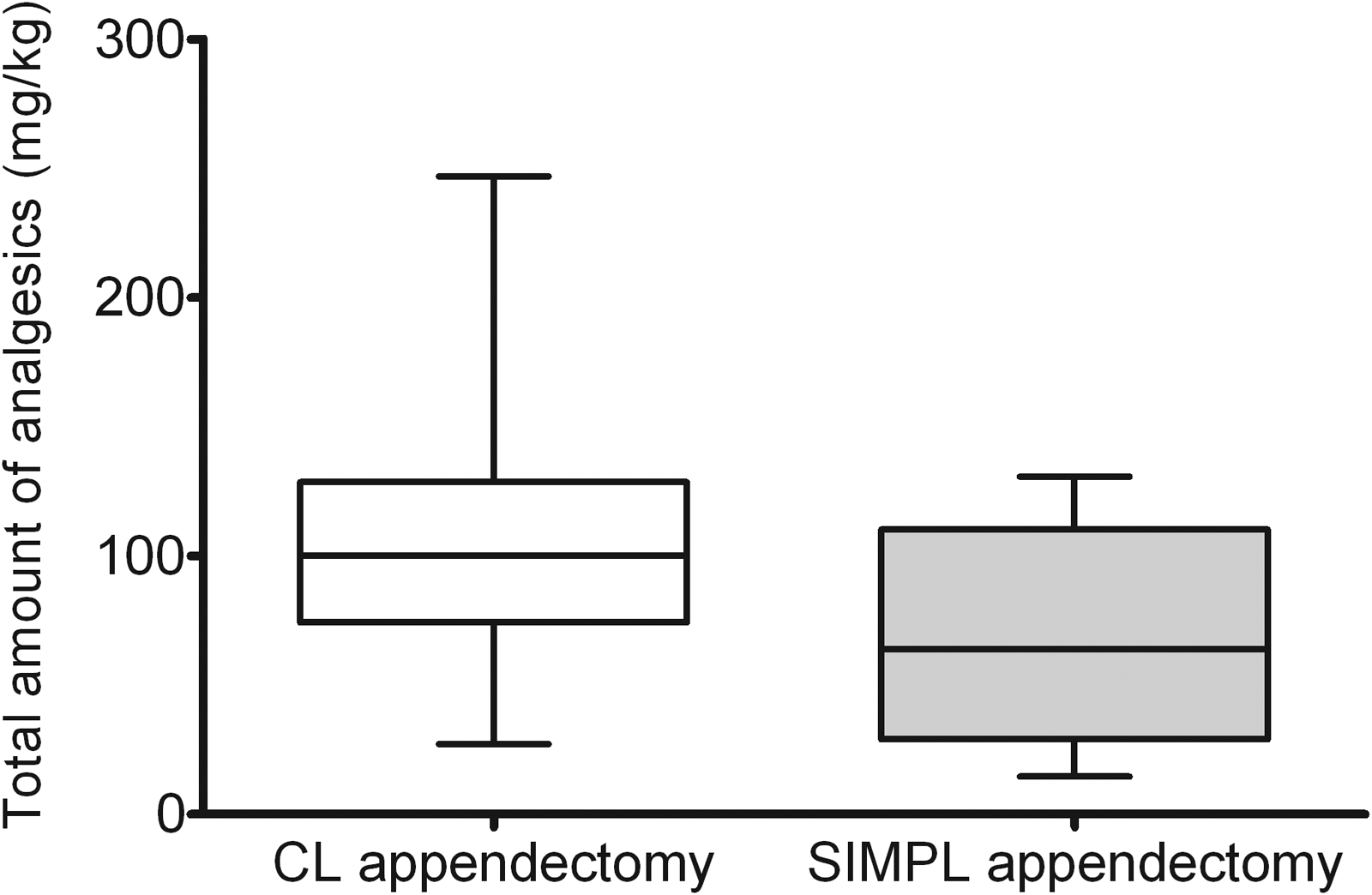
The total amount of required analgesics (mg/kg body weight) after SIMPL was significantly lower than after CL appendectomy.
Discussion
Single-incision laparoscopy claims to admit an almost “scarless surgery” and suggests various advantages for the patients.4–6 However, especially in children and adolescents, this discussion is presently substantiated mainly by feasibility studies. Further, the increase in operative costs for disposable instruments such as the TriPort System may attenuate the enthusiasm for an invisible scar. 7 Solid evidence about benefits for the patient, such as less postoperative pain and improved cosmetics, is still pending. The present study aims to contribute to this debate.
Theoretically, the single surgical access may either reduce postoperative pain by minimizing the operating trauma or induce it, because multiport devices require a minilaparotomy, which may amplify the surgical injury—Quod erat demonstrandum pro libris, which needs to be shown in children.
One of the major obstacles to evaluate the impact of single-surgical access techniques is that the term “SILS” is used for a wide variety of accesses in the literature: some authors favor one skin incision and place several regular ports through the abdominal wall 13 or through a surgical glove serving as a multichannel device. 14 Others employ bulky multiport systems, which require a considerable opening in the fascia.15,16 Likewise, no study has so far investigated the differences between a 15-mm access in a 4-year-old child and a 16-year-old adolescent.
In any case, a larger umbilical incision including the opening of the fascia over a longer segment may translate into more postoperative pain. 7 This has also been theoretically supported by an elegant study that examined the impact of wound sizes. The author hypothesized that the total tension across multiple incisions is always less than the total tension for one incision of the same total length, concluding that one 20-mm port may not be superior to three 5-mm ports in terms of port-site morbidity. 17
On the contrary, others have speculated that limiting the number of incisions will decrease the trauma to the tissue and translate into reduced pain, which is in line with our findings. In 43 adults undergoing SILS versus conventional laparoscopic appendectomy, short-term operative outcomes such as postoperative pain scores and length of hospital stay did not differ. 18 Another randomized controlled study examined pain scores in 40 adults who underwent SILS or classic laparoscopic cholecystectomy and observed significantly lower pain scores at 6 and 12 hours postoperatively as well as a reduced request for analgesics and an unaltered incidence of nausea and vomiting after the SILS procedure. 19 In a retrospective study on 20 consecutive pediatric SILS interventions including appendectomy, intravenous analgesia requirements and hospital length of stay mirrored that of a standard laparoscopy. 20 Similarly, Chandler et al. reported an overall decrease in intravenous narcotics after single-incision laparoscopic appendectomy when compared with a conventional laparoscopic appendectomy in a large study on 110 children. 21
Although systematic studies on single-surgical access interventions especially in children are sparse, our findings underscore those of others, proofing that single-incision laparoscopic appendectomy is a safe technique even in young as well as obese children.12,21–24 In our study, all operations were laparoscopically completed without conversion or addition of extra ports. Mean operation time was similar for conventional laparoscopic and SIMPL appendectomy, which is in parallel to findings of others in adult and children.18,22 However, even shorter operation times for SILS than CL appendectomy in children have been reported. 12 This may be due to an increased number of cases, underscoring the importance of the learning curve for this novel technique or differences in access techniques.8,21 Most important though, using a multiport system (SIMPL) we obviated the need for extra ports or extra instruments without a port, which are “hidden” in some series of SILS. 12
In summary, the present study substantiates the evidence that SIMPL appendectomy in children and adolescents is not only feasible, but also beneficial for the patient. In our small group of children, SIMPL appendectomy did not translate into increased postoperative pain, but reduced the amount of postoperative analgesics compared with a conventional laparoscopic access. Presently, we are conducting a randomized, blinded study to validate these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.