
Abstract
Abstract
Pulmonary intercostal hernias are extremely rare. They have been reported to occur in children after blunt trauma to the chest wall as a result of disruption of intercostal muscle fibers. We present a case of a left anterior chest lung hernia caused by blunt handlebar chest trauma in a 13-year-old boy treated with placement of a mesh using a video-assisted thoracoscopic approach.
Introduction
Case Report
A 13-year-old Caucasian boy sustained blunt injury with bruising to the left anterior-lateral chest wall after an accidental fall on the handlebar of his bicycle. Approximately 10 days after his injury he noticed a bulge in that region, which became more pronounced with coughing. He reported mild discomfort associated with the bulge. A chest radiograph was obtained and it was normal. His physical examination was remarkable by a soft tissue anterior left chest wall mass that bulged with valsalva maneuvers and was not noticeable at rest. It was not painful and it did not cause any respiratory symptoms. The diagnosis of a left anterior pulmonary hernia was made based on the clinical history and physical examination findings. Patient underwent thoracoscopic exploration and was found to have an intercostal muscle fascial defect at the level of the sixth intercostal space, lateral to the midclavicular line. This corresponded to the point of injury reported by the patient. A hernia sac was observed (Fig. 1) within the muscle fascial defect, which measured 4×8 cm. A total of three left chest trocars were placed (5 mm) for the video-assisted thoracoscopic repair. The trocars were placed in the posterior left chest at the level of the posterior axillary line, above and below the level of the hernia. A GORE-TEX® pericardial patch (WL Gore & Associates, Inc., Flagstaff, AZ) 0.1 mm thick, 6×12 cm in size, was rolled and placed inside the left pleural cavity through one of the 5 mm trocars. It was unrolled and placed over the hernia defect on the chest. The patch was secured in place by placement of multiple ProTacks™ (Covidien, Mansfield, MA) as illustrated in Figure 2. At least half of the ProTacks were anchored to the ribs to minimize the risk of patch migration or dislodgement. The hernia sac was not resected. The CO2 pneumothorax was evacuated before closure of the trocar sites and the patient did not require a postoperative chest tube. The patient was discharged 24 hours after the procedure. Short- and long-term follow-up (1 year postoperative) demonstrated complete resolution of the lung hernia and the patient has remained asymptomatic.
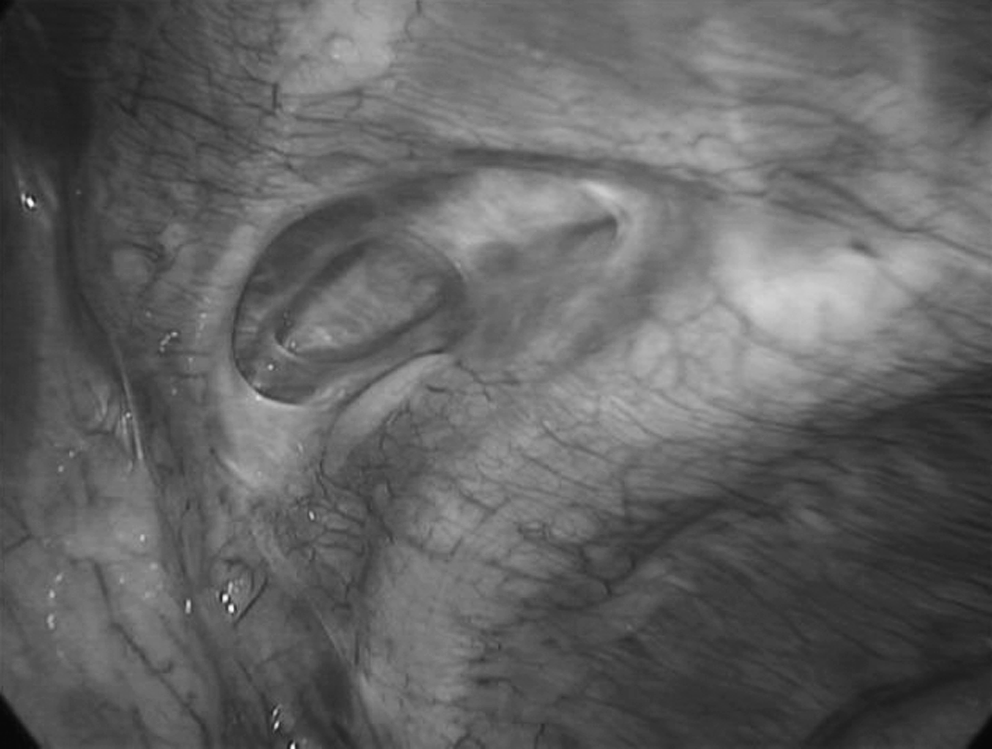
Thoracoscopic view of the handlebar intercostal chest wall hernia. The defect and hernia sac can be clearly observed within the muscle fascial defect that measured 4×8 cm.

The GORE-TEX patch completely covered the defect and it was secured in place by using multiple ProTacks.
Discussion
Lung hernia, also described as pulmonary hernia, is considered a rare condition that can be congenital or acquired. A variety of case reports can be found in the medical and surgical literature. Our report is the sixth pediatric case in the English literature caused by handlebar trauma to the chest.1–6 The term “handlebar hernia” was originally proposed by Dimyan et al. in 1980 7 to describe a traumatic abdominal wall hernia in a patient with blunt abdominal injury caused by the handlebar of a motorcycle. Subsequent use of the term has broadened to include similar injuries sustained from the handlebar of a bicycle, as reported in our case. These injuries are localized hernias resulting from focal, blunt trauma to the abdominal or chest wall that is not sufficient to penetrate the soft tissues but strong enough to cause muscle and fascial disruption. Lung hernias have been reported in adults and children.8,9 However, the frequency of traumatic lung hernias is greater in adults than in children. In addition, lung herniation can be categorized based on its etiology as traumatic, spontaneous, or pathologic. 10 Traumatic lung hernias represent more than half of all the acquired lung hernias reported and tend to occur through an intercostal space after surgery or blunt trauma to the chest. 11 It has been noted that there appears to be an injury pattern within this category of lung hernias that is limited to children. It involves an isolated handlebar injury to the thoracic cage resulting in intercostals lung herniation without associated fractures or other injuries. The lack of associated injuries or fractures is felt to be due to the relative laxity of the pediatric thoracic cage; thus, the intercostal muscles and fascia are disrupted, allowing a lung hernia to develop. The mechanism is identical to that occurring with handlebar hernias of the abdomen, and as such, Holmes et al. 6 have coined the term “thoracic handlebar hernia” to describe this unique injury. Our case is representative of this type of pulmonary hernia.
Lung hernias in symptomatic patients are usually treated with open surgical repair. A few different methods for repair have been reported, ranging from primary closure of the defect with adjacent tissues, closure with synthetic mesh, or plastic surgical procedures.2,10,12 With the advent of video-assisted thoracoscopic surgery (VATS), a new method for repair was developed, as described by Bossche et al. 13 in 1999. The advantage of this method is related to the smaller incisions, eliminating the need for thoracotomy and rib retraction. Patients treated with VATS have a shorter hospital stay, less postoperative pain, and shorter hospital stay. There are some limitations of VATS as seen in cases with extensive pleural adhesions or if the anatomical site does not allow access with thoracoscopy. 13 As illustrated by our case report and by the one reported by Bossche et al., 13 the repair using a synthetic mesh can be easily accomplished with VATS. The availability of tacking thoracoscopic devices allows for permanent and simple fixation of the mesh to the thoracic wall. In the last 10 years, as the application of minimally invasive techniques to thoracic surgery has increased, new cases of lung hernias secondary to VATS (iatrogenic) have been reported.14,15
Spontaneous resolution of lung hernias are known to occur.3–6 It appears that observation is a viable option in asymptomatic patients with small hernias. The expected length of time for resolution is unknown, and it is possible that a prolonged wait may allow for a progressive increase in the size of the lung hernia, which may necessitate a more extensive repair. Incarceration of lung hernia is unusual. 16 It is usually due to an entrapment of the lung on rib spicules at the site of a rib fracture. 17 We advocate routine mesh closure under thoracoscopic observation for symptomatic pediatric patients since the procedure carries a low morbidity and excellent outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.