
Abstract
Abstract
Background:
We present a unique experience with a patient who had undergone continuous ambulatory peritoneal dialysis (CAPD) after laparoscopic repair of ventral incisional hernia (LRVIH) with an expanded polytetrafluoroethylene (e-PTFE) mesh (DualMesh®; WL Gore) and who later suffered from multiple episodes of CAPD-related peritonitis without any signs of mesh infection.
Methods:
A 48-year-old man with an open abdominal aortic reconstruction in 1994 for occlusive arterial disease presented with an incisional ventral hernia. He underwent LRVIH using an e-PTFE mesh of 30×20 cm.
Results:
Postoperatively, he developed renal failure. For various reasons, the only therapeutic option was CAPD. A CAPD-catheter was implanted via laparoscopy, taking care not to compromise the mesh that was completely covered with neoperitoneum. After 3 months of uneventful CAPD, he developed a bacterial peritonitis. Antibiotic treatment failed and the CAPD-catheter was removed. The mesh was left in place and the patient recovered. Later on another CAPD-catheter was implanted via laparoscopy and used for 10 months. Again he developed peritonitis from which he recovered after catheter removal. Mesh was left in place and remained uninfected, probably protected from intra-abdominal bacteria by the neoperitoneum.
Conclusions:
The risk of secondary infection of an intra-abdominal mesh seems to diminish largely after neoperitonealization of the mesh. CAPD seems possible in a patient with an intra-abdominal mesh when it is covered with neoperitoneum.
Introduction
We present a unique experience with a patient who had undergone CAPD after LRVIH with an expanded polytetrafluoroethylene (e-PTFE) mesh (DualMesh®; WL Gore) and who later suffered from multiple episodes of CAPD-related peritonitis without any signs of mesh infection.
Case Report
A 48-year-old man presented with a large symptomatic incisional hernia at a long midline incision in April 2007. His medical history included abdominal aortic reconstruction for arterial occlusive disease in 1994. Although the patient was already showing signs of compromised renal function, he was accepted for surgery because of the disabling effect of his hernia.
He underwent LRVIH in May 2007. An e-PTFE mesh of 30×20 cm was used. The mesh was fixed to the abdominal wall with a “double crown” of tacks (Protack; Covidien). 1 The procedure took 149 minutes and passed uneventfully.
Postoperatively, the patient developed a progression of renal failure that required renal replacement therapy. Hemodialysis via a tunnelled central venous catheter was started. Because of his vascular status, kidney transplantation was not an option. After 6 months of treatment with intermittent haemodialysis, the catheter was obstructed, and the patient refused further haemodialysis. CAPD had to be started. In April 2008, a CAPD catheter (Tenckhoff cath; Tyco Healthcare/Kendall) was implanted laparoscopically by using two trocar ports left laterally in the abdomen, taking care not to compromise the mesh. At laparoscopy, the mesh was found to be completely covered with a thin layer of tissue and some omental adhesions, which were both left intact.
Urea clearances and ultrafiltration rates were satisfactory using a change volume of 11 L/day performed in six cycles using 2.9% glucose solutions (Baxter Physioneal; Baxter Ltd.).
After 3 months of uneventful CAPD, the patient developed CAPD-related peritonitis. Cultures taken from peritoneal dialysis fluid showed infection with Staphyloccus epidermidis. The peritonitis was initially treated with cefazoline intraperitoneally. Antimicrobial treatment was unsuccessful and in July 2008 the catheter had to be removed. The intra-abdominal mesh was showing no signs of infection and was left in place. The patient's condition improved directly and, after a 6-week period of hemodialysis, a new CAPD catheter was inserted via laparoscopy in September 2008. Two trocars were inserted now right laterally in the abdomen, taking care not to compromise the mesh. The situation regarding the mesh was found to be unchanged: no signs of infection and the mesh completely covered with a thin layer of tissue, resembling the patient's peritoneum and omental adhesions (Fig. 1). That catheter was uneventfully used for CAPD the following 10 months. An abdominal X-ray proved adequate positioning of the CAPD catheter (Fig. 2). Then, the patient again developed a CAPD-related peritonitis. Peritoneal fluid cultures showed infection with Delftia acidovorans. Treatment with piperacilline was not successful and the catheter had to be removed again. The intra-abdominal mesh was showing no signs of infection and was left untouched. In October 2009, a third CAPD catheter was inserted again left laterally. At this laparoscopy, there were significantly more adhesions in the abdominal cavity, though not against the mesh itself. That catheter failed to function well and, after being repositioned laparoscopically once without effect, it was finally removed in November 2009. The patient was put on hemodialysis again and remained without any signs of mesh infection until the present day (December 2010).
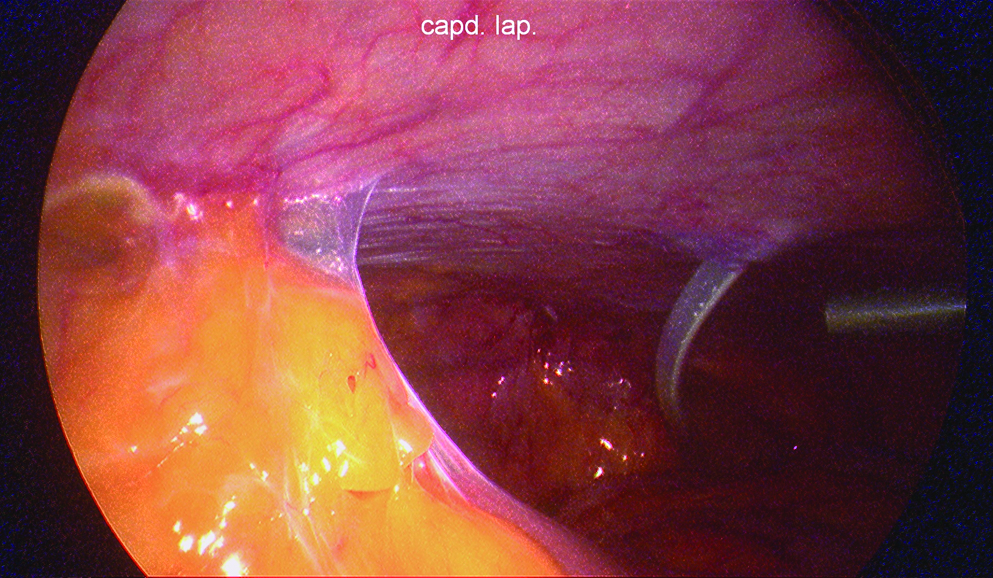
Laparoscopic view of expanded polytetrafluoroethylene mesh (upper left) covered with the neoperitoneum and with omental adhesions. Middle right continuous ambulatory peritoneal dialysis (CAPD) catheter reaching to cavum Douglasi and further right one of the trocars.

Plain X-ray of the abdomen showing the double crown of tacks used for fixation of the mesh and the CAPD catheter in the lower abdomen.
Discussion
LRVIH is dependent upon the intra-abdominal implantation of synthetic meshes. Although mesh use is crucial for effective hernia repair, prosthetic infections can cause a formidable surgical problem. Once infected, a mesh nearly unequivocally requires removal because eradication of infection with mesh in place is usually impossible. Resection of an infected mesh is an operation fraught with morbidity. The risk of surgery, the risk of injury to adjacent structures, the resulting open wound, and the inevitable hernia recurrence are daunting possibilities.
Compared to open repair, LRVIH reduces the risk of mesh infection from 3% to 18%2,3 to less than 0.7%.4,5 The low infection rate is, in fact, the most attractive benefit of LRVIH.
In patients with CAPD there is a high risk of bacterial peritonitis, with a reported incidence ranging between 0.367 and 0.434 episodes per patient per year. 6 Although CAPD peritonitis is obviously a common problem in the renal failure population, it seems that most episodes can be managed using intraperitoneal antibiotics without the need for surgical intervention. However, CAPD peritonitis in patients with an infection-susceptible synthetic material in the abdominal cavity might carry a very high risk of mesh infection. This can further lead to maintenance of CAPD peritonitis and failure of conservative treatment, leading to the necessity to remove both the catheter for CAPD and the infected mesh used for hernia repair. If this is really the case, previous LRVIH might be a contraindication for CAPD. However, there are absolutely no experiences on this issue so far.
Being aware of the infection threat, but also left without any alternative for absolutely indicated renal replacement therapy, we had to perform CAPD in a patient with an already-implanted e-PTFE mesh. The latter has probably been the most frequently used mesh in LRVIH so far, 7 as it prevents tissue ingrowth and severe adhesion formation. However, once infected, e-PTFE undergoes irreversible structural changes and typically responds poorly to antimicrobial regimens. The ultrastructure of the prosthetic biomaterials in general seems of paramount importance for its susceptibility to infection. Polyfilamented meshes and microporous biomaterials, such as e-PTFE, contain pores and interstices smaller than 10 μm, in which bacteria averaging 1 μm in size can proliferate while protected from leukocytes averaging 15–20 μm. 8
The intra-abdominally placed mesh of our patient was indeed exposed to peritoneal fluid containing bacteria as was proven by multiple Gram stains. That mesh infection has never occurred can be explained only by taking into consideration that the bacteria containing peritoneal fluid and the intra-abdominal mesh have actually never been in direct contact.
At reoperations after LRVIH, Koehler et al. 9 observed development of a well-vascularized neoperitoneum across the entire mesh surface in all patients in whom an e-PTFE mesh had been implanted for more than 2 weeks. Animal studies have already shown that neoperitoneum develops within 2 weeks of LRVIH. 10 Our experience with 72 subsequent abdominal operations after LRVIH indicate that 1 month after LRVIH an e-PTFE mesh is unequivocally completely covered with a thin layer of tissue resembling the patient's peritoneum. 11 In the same study, this complete neoperitonealization of mesh proved to be protective against mesh infections at five contaminated reoperations after LRVIH. In all second-look operations performed 1–84 months after LRVIH with Parietex™ Composite mesh (Covidien), Chelala et al. also observed the neoperitoneum that perfectly covered the entire mesh. 12
Conclusions
These observations indicate that the risk of secondary infection of an intra-abdominal mesh diminishes largely after complete neoperitonealization of the mesh. If we assume that that process requires 4 weeks and possibly less after LRVIH and implantation of mesh, CAPD seems possible after that period. Care must be taken in all subsequent procedures, such as placement of a CAPD-catheter, to leave the neoperitoneal coverage of the mesh completely intact.
Footnotes
Disclosure Statement
No competing financial interests exist.