
Abstract
Abstract
For safe and effective laparoscopic surgery it is important to maintain a favorable view of the operative field. However, the use of a conventional liver retractor needs an additional wound and carries a risk for liver injury during surgery. We developed a novel retraction technique for the lateral lobe of the liver using a silicone disk (Hakko Co. Ltd.) during laparoscopic surgery. We used a silicone disk that consists of a silicone rubber membrane inside a flexible ring and four monofilament threads. The disk can be inserted into the abdomen under the pneumoperitoneum through a 12-mm port and is located at the dorsal side of the lateral lobe of the liver. The threads are withdrawn through the abdominal wall, two threads close to the infraxiphoid space and the other two threads bilaterally below the costal arch. Thus, the lateral lobe of the liver is safely raised to the ventral side and covered with a silicone membrane. We introduced this technique for various laparoscopic operations, such as gastrectomy, gastroplasty, and fundoplication. There were no complications related to the procedure. This retraction technique is easy, results in less liver damage, and provides an excellent operative view around the esophageal hiatus. The silicone membrane covering the lateral lobe reduces the risk of liver injury during surgery using laparoscopic forceps to a low level.
Introduction
Here, we describe a novel technique for retraction of the lateral lobe of the liver using a silicone disk during laparoscopic surgery. This procedure is easy, carries only a small risk of liver damage than other technique, and provides an excellent operative view around the esophageal hiatus even in patients with hypertrophic fatty liver.
Preparation of a Device for Liver Retraction
The silicone disk (Hakko Co. Ltd.) consists of a silicone rubber membrane inside a flexible ring. It is used for organ exclusion during laparoscopic surgery. Two sizes are available, 120×80 mm and 160×100 mm (Fig. 1A). We used a small disk for retraction of the lateral lobe of the liver. The product has four eyelets on the edge of the major and minor axes of the flexible ring. We ligated four monofilament threads (0-PDS; Johnson & Johnson KK. Co. Ltd.) to the flexible ring through these eyelets (Fig. 1B). One of the threads attached to the minor axis was tied to the tip of a J-shaped retractor (Endo Maxi Retract or Endo Mini Retract; United States Surgical Corporation).
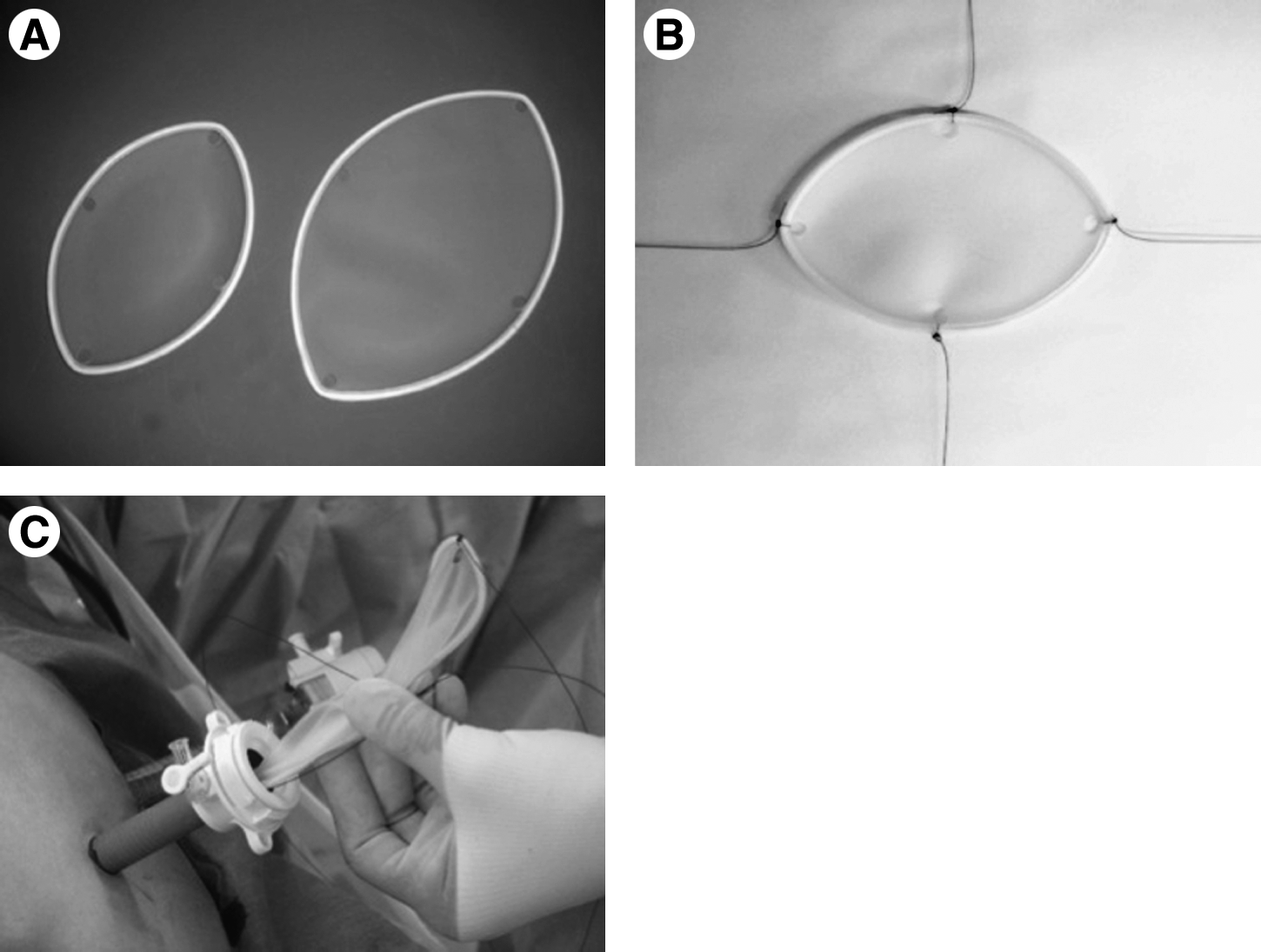
Preparation of the device.
Surgical Procedure
The silicone disk was inserted through a 12-mm port under the pneumoperitoneum, which spontaneously regained its original shape in the abdominal cavity (Fig. 1C). The lateral lobe of the liver was raised from the dorsal side using laparoscopic forceps. The hook of the J-shape retractor was advanced to the coronary ligament of the lateral lobe of the liver from the dorsal to the ventral side (Fig. 2A). Then, a small incision was made near the tip of the J-shaped retractor at the ventral side of the coronary ligament (Fig. 2B). The thread from the ventral side was held using forceps (Fig. 2C). The thread was pulled out close to the infraxiphoid space through the abdominal wall using an Endo Close (United States Surgical Corporation) (Fig. 2D). The disk was located at the dorsal side of the lateral lobe of the liver by this procedure. The contralateral thread attached to the minor axis of the ring was guided to the infraxiphoid space (Fig. 3A). The threads from the major axis were pulled to the bilateral infracostal arch in a similar manner (Fig. 3B). Thus, the lateral lobe of the liver was safely raised to ventral side and covered with the silicone membrane (Fig. 3C). At the end of surgery, the disk could be easily removed together with the 12-mm port.
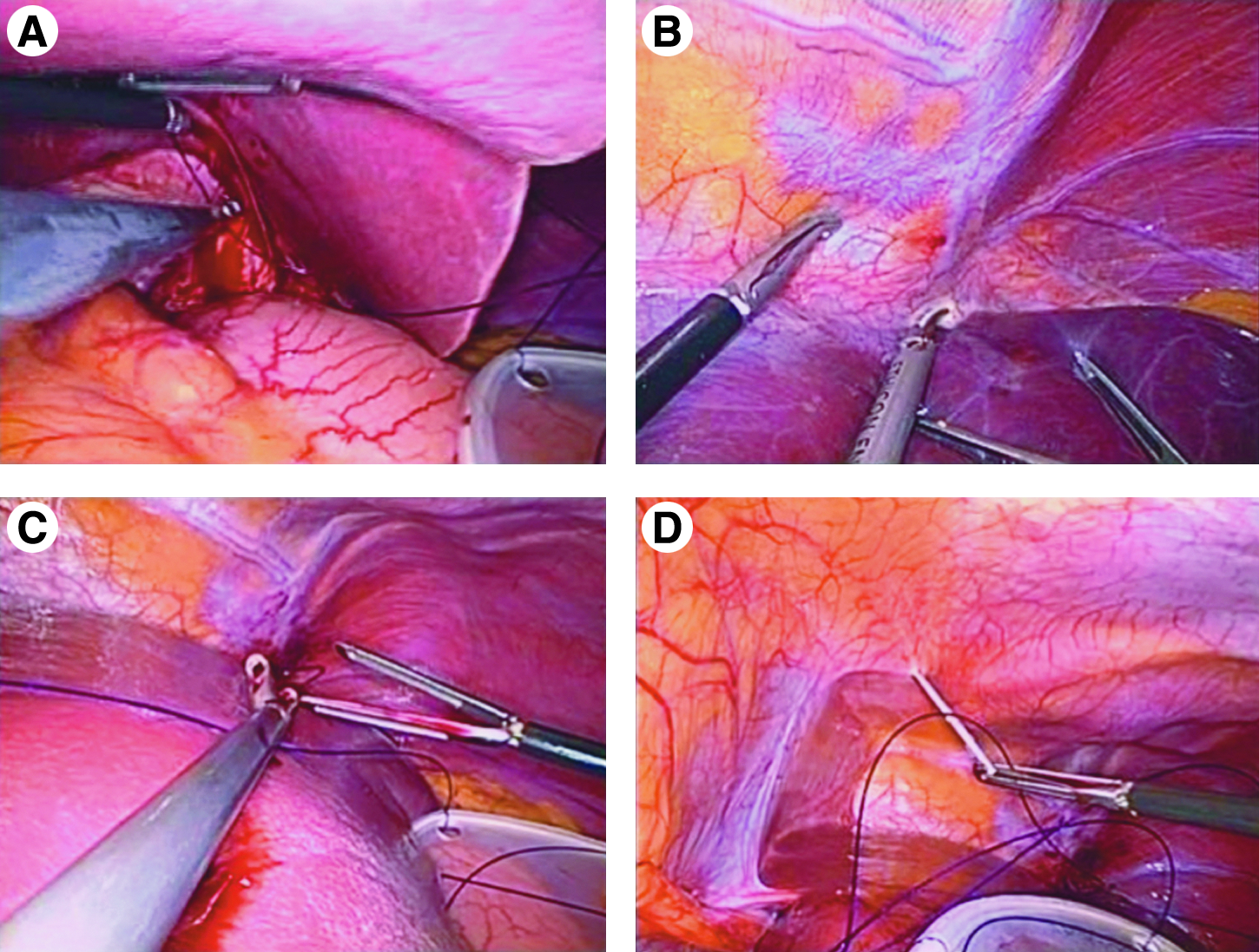
Procedure for raising the lateral lobe of the liver (1).
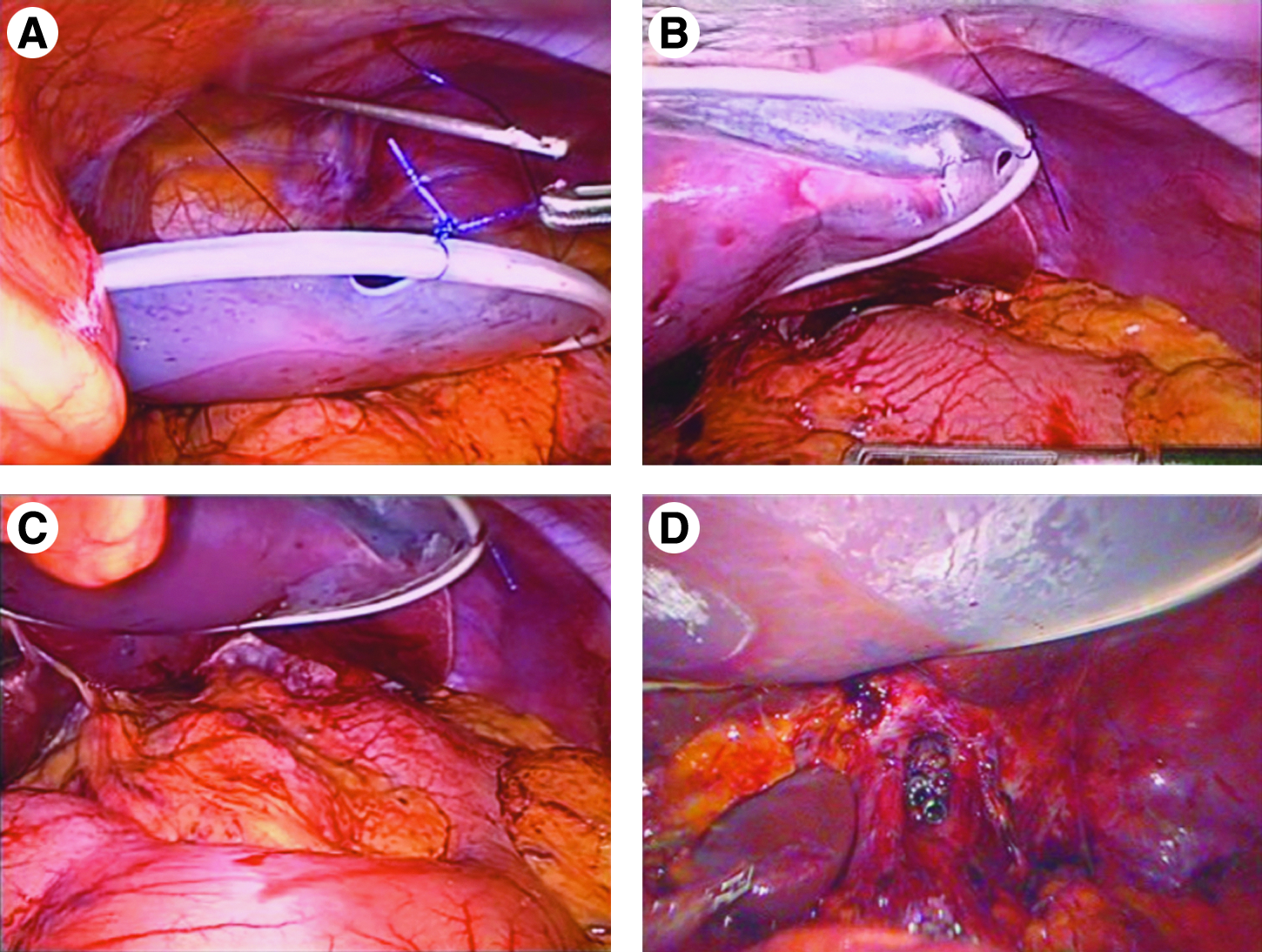
Procedure for raising the lateral lobe of the liver (2).
Our Experience with the Silicone Disk
We introduced this technique in June 2010 for various laparoscopic operations. These included gastroplasty, gastrectomy, and fundoplication (details of the number of these procedures in Table 1). None of the cases required the additional port from infraxiphoid space. Especially, we were able to perform laparoscopic fundoplication through only two ports with this retraction technique. This retaraction technique provides an excellent view around the esophageal hiatus and is safe even in operations on patients in whom the lateral lobe of the liver is hypertrophied (Fig. 3D). The risk of liver injury during operation by laparoscopic forceps around the esophageal hiatus is low because of the silicone membrane covering over the lateral lobe. There were no complications related to this procedure.
Discussion
The safety and accuracy of laparoscopic surgery depends on adequate working space and operative view. In laparoscopic upper abdominal surgery, the operative view is obstructed by the lateral lobe of the liver. Many techniques have been reported for retraction of the lateral lobe of the liver during laparoscopic surgery.1–3 However, conventional liver retractors, such as fan retractors and toothed graspers, require an additional infraxiphoid port, which may be associated with port site complications and postoperative liver damage.3–5 Yassa and Peters 5 reported CT findings of focal hepatic injury after surgery for upper gastrointestinal malignancies in 10 cases. They used a table-mounted, modified Weinberg's retractor and concluded that the location of hepatic injury corresponded to the site of retractor placement during surgery. In a case of retractor injury during laparoscopic Nissen fundoplication, Pasenau et al. 3 used a toothed grasper for retraction of the lateral lobe of the liver. They concluded that a pause in the operation when a change in color of the liver was detected helped to reduce the risk for liver hematoma and that retractors without sharp edges should be used to decrease the risk for direct liver laceration. In upper abdominal laparoscopic surgery, such as gastrectomy with lymphadenectomy or fundoplication, a safe and effective retraction technique for the lateral lobe of the liver is desirable.
Sakaguchi et al. 1 reported a simple lifting technique of the liver using a Penrose drain and a J-shaped retractor during laparoscopic gastrectomy. Their technique is easy and less costly than other retraction techniques. We have previously used this technique in laparoscopic gastrectomy for gastric cancer and consider it to be useful, but it presents some operative difficulty in cases with a hypertrophic fatty lateral lobe of the liver. Accordingly, we have developed a novel retracting technique of the liver. De la Torre et al. 2 described a liver suture retractor using 0 silk suturing across the right crus above the esophageal hiatus during single-incision laparoscopic placement of an adjustable gastric band. Retraction of the liver during single-incision laparoscopic surgery is a challenging technique for laparoscopic surgeons. 6 However, the use of a thin liver retractor in patients with a hypertrophic lateral lobe of the liver carries a comparatively high risk for liver injury during operation. Our technique using the silicone disk is little more costly than conventional technique using Penrose drain, but it is safe and associated with less liver damage, and the risk for liver injury from laparoscopic forceps during surgery is very low because of the silicone membrane covering the lateral lobe.
In conclusion, our technique is easy and safe compared with other retraction techniques. The procedure can be performed in various types of laparoscopic gastrointestinal surgery without the need for specific skill. Therefore, we believe that our retraction technique can be used in single-incision laparoscopic surgery of the upper gastrointestinal tract.
Footnotes
Disclosure Statement
No competing financial interests exist.