
Abstract
Abstract
Background:
The division of the splenic hilum is the most delicate step during laparoscopic splenectomy. An incorrect approach could lead to a series of related complications. Aim of the study was to report authors' personal experience in a series of 107 laparoscopic splenectomies where the splenic hilum was approached by means of stapling device. A possible relationship between instruments used to divide the splenic artery and vein and complications was analyzed.
Methods:
Laparoscopic splenectomy was performed in 107 cases at authors' institution between 1998 and January 2011. In all the patients, splenic hilum was approached by means of vascular stapler.
Results:
Indications for the spleen removal mainly were hematologic disorders. Associated surgical procedures were performed in 32 cases. Among the 13 patients who required a conversion to open splenectomy, only in 3 cases the reason was related to the hilum management. Postoperative complications included portal vein thrombosis in 3 cases, pancreatic fistula in 1 case, and bleeding, requiring reintervention, in 2 cases.
Conclusions:
The use of the stapling device is a safe and effective method to approach the splenic hilum during laparoscopic splenectomy. In experienced hands it showed a low rate of related complications.
Introduction
Splenic hilum artery and vein may be approached and secured by means of clip placement, 5 suture ligatures,5,6 radiofrequency instruments,7–9 and stapling devices.10–12 The use of staplers to seal splenic vessels seems to be feasible and may solve many hemostatic problems in the operating theatre. However, there are some concerns about possible complications such as bleeding, pancreatic injury, arteriovenous fistula formation, and splenic or portal vein thrombosis related to the stapler usage.7,13,14
In this study the authors analyzed their experience on 107 cases where vascular stapling of the splenic hilum has been routinely used during laparoscopic splenectomy. Intra- or immediate postoperative bleeding, as well as other postoperative complications, has been evaluated and discussed.
Materials and Methods
The charts of 107 patients operated on with laparoscopic splenectomy between January 1998 and January 2011 at authors' institution were retrospectively reviewed.
Patients' age ranged from 8 to 83 years, and male-to-female ratio was 0.81. Spleen size (longitudinal diameter), assessed by computed tomography scan, ranged from 10 to 14 cm in benign splenic diseases and from 18 to 24 cm in malignant disorders. Haemophilus influenzae, meningococcal, and pneumococcal vaccinations, if not previously received, were administered at least 2 weeks before surgery.
Laparoscopic splenectomies were performed with patients lying in the right lateral position with the left flank elevated about 30° above the operating table. The trocars were positioned in the mid-clavicular line 10 mm above the transverse umbilical line (Hasson trocar), in the subcostal area laterally to the mid-clavicular line (5 mm trocar), in the left flank at the level of the transverse umbilical line (12 mm trocar), and in the subcostal area in the anterior axillary line (5 mm trocar). After introduction of the trocars, diagnostic laparoscopy and detection of accessory spleens were accomplished. The procedure started with the division of the splenocolic ligament followed by the section of the gastrosplenic ligament by means of the ultrasonic dissector (Ultracision Harmonic Scalpel; Ethicon Endosurgery, Inc., Cincinnati, OH). At that moment splenic artery was recognized, mobilized, and double clipped to avoid bleeding during the following steps of the procedure. The convex surface of the spleen was then accurately dissected from the lateral abdominal wall and from the diaphragm. At that point, hanging the spleen, the splenic hilum was approached from the anterior aspect. Splenic artery and vein were secured, taking care not to damage pancreatic tail, using the stapling device (Endo GIA Vascular Stapler; Ethicon Endosurgery, Inc; Fig. 1). The spleen was then inserted in a plastic bag (endobag), which was pulled through the 10-mm abdominal access. In the end, the spleen was crushed and removed piece by piece. In malignant cases, where spleen size was particularly marked, the spleen was pulled out the abdominal cavity through an accessory abdominal incision.
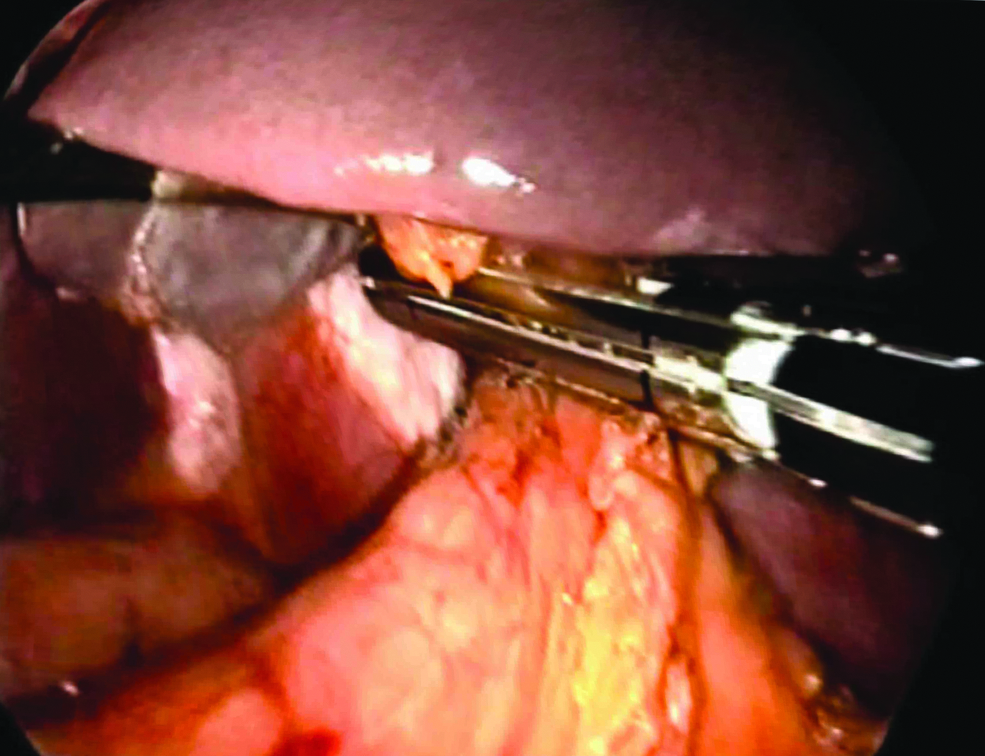
Hanged spleen technique and splenic hilum section by means of stapling device.
Results
Indications for laparoscopic splenectomy were idiopathic thrombocytopenic purpura in 74 cases, splenic lymphoma in 10, hereditary spherocytosis in 10, β-thalassemia in 4, and mielofibrosis, splenic cyst, splenic mycosis, and benign tumors in 9 cases. In 32 patients laparoscopic splenectomy was associated with concomitant surgical procedures: liver biopsy (11 cases), cholecystectomy (10 cases), ovarian cyst resection (2 cases), abdominal lymph node biopsy (2 cases), accessory spleens removal (6 cases), and pancreatic tail resection (1 case). Mean operative time was approximately 65 minutes, ranging from 40 minutes to 1½ hours.
In 13 patients (12.2%) laparoscopic splenectomy was converted to open procedure. Causes for conversion included in 10 cases invasion of the splenic malignant disease to surrounding structures (diaphragm, pancreatic tail, stomach, and splenic flexure) and in 3 patients intraoperative bleeding.
Postoperative complications were encountered in 6 cases (5.6%). Bleeding, requiring reintervention, occurred in 2. Three patients developed a portal vein thrombosis and another 1 a pancreatic fistula, all conservatively treated. No death has been reported. Perioperative data have been summarized in detail in Tables 1 and 2.
Laparoscopic Surgery Unit, Department of Surgery, University of Catania, Policlinico V. Emanuele Hospital, Catania, Italy.
CT, computed tomography.
Laparoscopic Surgery Unit, Department of Surgery, University of Catania, Policlinico V. Emanuele Hospital, Catania, Italy.
Discussion
Laparoscopic splenectomy has been considered in many institutions the standard approach for most hematological diseases requiring removal of the spleen, and it is now accepted for a variety of spleen disorders. 7 Even though laparoscopic splenectomy offers a myriad of advantages over conventional splenectomy,11,15,16 many technical aspects still remain controversial.
Splenic hilum vessel control is the most troublesome step in the laparoscopic removal of the spleen. Intraoperative or postoperative bleeding from the splenic hilum is the complication of major concern during this procedure. 4 Pancreatic injury, pancreatic fistula, arterovenous fistula formation, and portal vein thrombosis are other complications that may be related to the technique used to control the splenic artery and vein during the minimal access surgery of the spleen.13,14 A proper splenic hilum hemostatic control is thereby essential to reduce the incidence of these complications.
For many years hilar vessels were individually identified and secured by the use of clips or ligatures,5,6 but with the huge advancement in laparoscopic field, today other technical approaches have gained a distinct reputation for transection of the splenic pedicle.7–13
In literature some instrumental devices have been proposed and used by several different authors.7–12 Evaluation on the safety and the efficacy of some of these reported techniques, however, is controversial since no randomized studies have been performed and complications cannot be specifically related to each technical approach of the splenic hilum.
Misawa et al., 7 Alwabari et al., 8 and Wang et al. 9 reported the use of radiofrequency instruments to seal the splenic vessels. In Misawa et al.'s series, 7 radiofrequency has been used in 27 cases, associated with ligation in 9 of them. In his study a conversion because of hilar bleeding was referred in 1 case, and a postoperative hemoperitoneum and a pancreatic fistula in other 2 patients. In 1 case, in addition to the radiofrequency instrument, it was necessary a clip placement because of bleeding from a branch of the splenic artery as a consequence of an incorrect application of the radiofrequency device. However, except for this last one, in Misawa et al.'s study a strict relationship between radiofrequency technique and complications cannot be evaluated. Similarly, in Alwabari et al.'s report, 8 intraoperative bleeding, requiring in 1 case conversion to open surgery, cannot be specifically related to the radiofrequency device since several techniques have been used in the same series. Eventually, in Wang et al.'s report, 9 no complications seemed to be associated with the use of the radiofrequency instrument for splenic hilum section.
The use of stapling devices has been described by several other authors. In large series this technique of splenic pedicle control has been related to bleeding or other postoperative complications.10–12
In Casaccia et al.'s study, 10 the stapling device was used in 676 laparoscopic splenectomies. In this multicenter analysis a surgical conversion was made in 54.1% of 39 patients because of hemorrhagic matter involving the hilum. A postoperative bleeding was encountered in 30 cases, of which 26 required reintervention. Splenic/portal vein thrombosis occurred in 14 cases and 5 patients developed a pancreatitis. Wang et al. 11 reported 5 cases of conversion to open splenectomy and 4 cases of postoperative bleeding. Kawanaka et al., 12 eventually, encountered 12 cases of massive intraoperative bleeding, which were responsible for conversion to open surgery. Postoperative bleeding was instead reported in 8 cases, and 24 patients developed a portal vein thrombosis. The aforementioned data have been reported in Table 3.
In our experience splenic hilum stapling device has been used in a consecutive series of 107 patients. We report an incidence of bleeding (intra- and postoperative) in 5 cases (4.7%), which is on the average compared with those reported by the other aforementioned authors (0%–7.6%).7–12
In our opinion, it is essential that stapler is used with a proper technique. Before applying the device we dissected completely the spleen from the spleno-colic, gastro-splenic, and spleno-diaphragmatic ligaments. Moreover, the lateral position of the patient during the procedure is of help to apply the device while the “hanged spleen” technique 17 is accomplished.
Before firing the stapler we accurately separated the spleen from the pancreatic tail. Besides, in order not to damage the tail of the pancreas, the firing of the stapler was accomplished only after releasing the tension of the hanging manoeuver (Fig. 1). More specifically, first, the spleen is hanged; this allows the surgeon to cautiously position the vascular stapler across the splenic pedicle. Second, the spleen is released from the hanging and the vascular charge is fired; this raises the distance between the spleen and the pancreatic tail, increasing thereby the safety of the vessels sealing.
Using these technical pearls we report, besides a low incidence of intraoperative and postoperative bleeding, only 1 case of pancreatic fistula, encountered in the patient where pancreatic resection, was associated. In the 3 cases of portal vein thrombosis, although we assumed that it could be related to the usage of the stapler, a multifactorial etiology should be hypothesized.
Our conversion rate, as well as morbidity and bleeding incidence, is similar to those reported in other series with other techniques of splenic hilum hemostatic control. However, we believe that the use of staplers, which are easily available in the operating rooms, seems more feasible and easily reproducible in the surgical practice, provided that the above-reported technical steps are strictly followed.
In conclusion, the introduction of mechanical vascular staplers specifically dedicated to minimally invasive surgery has made the laparoscopic splenectomy procedure simple and yet safe. A proper technique and an appropriate training are essential to minimize the complications related to their use. Randomized, controlled trials, however, are needed to definitely evaluate the value of the stapling device in management of the splenic hilum during laparoscopic splenectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.