
Abstract
Abstract
Introduction:
Since the publication of the REMATCH trial results, it is estimated that almost 5 million Americans have been found to have heart failure. Limited availability of organs for transplantation, coupled with wider selection criteria for destination therapy, has resulted in a substantial increase in the number of patients with permanently assisted circulation. Given the high rate of complications related to circulatory assist devices, it is expected that these patients will be undergoing noncardiac surgical procedures more commonly.
Materials and Methods:
We describe a laparoscopic splenectomy in a patient supported with a Heartmate II left ventricular assist device. Using this case as a model, we discuss hemodynamic changes associated with pneumoperitoneum and anesthesia induction. Additionally, an extensive literature search was performed to asses the frequency of laparoscopic procedures performed on patients with circulatory support.
Results:
Laparoscopic splenectomy was performed without significant hemodynamic changes. To our knowledge, this is the first laparoscopic splenectomy performed in a patient with this mode of circulatory support.
Conclusion:
Laparoscopic procedures can safely be performed in patients with compensated heart failure, who are supported with ventricular assist devices.
Introduction
Clinical Case
A 60-year-old man with a Heartmate® II LVAD, implanted 20 months before presentation as “destination therapy” for ischemic cardiomyopathy, was admitted for treatment of Staphylococcus epidermidis bacteremia discovered during surveillance blood culturing. At the time of presentation, he was febrile (38.2°C), with a leukocyte count of 15.3×109 cells/L. There was no evidence of surgical-site infection, and intravenous antibiotic therapy with Vancomycin (1000 mg twice a day) was commenced. Upon availability of organism sensitivity, the therapy was changed to Cloxacillin (2000 mg every 4 hours). After 5 days of therapy, both fever and leukocytosis persisted. Subsequent computed tomography of the abdomen and chest revealed a large splenic abscess (Fig. 1). After considering the options of percutaneous drainage versus splenectomy, it was decided to proceed with laparoscopic splenectomy upon reversal of anticoagulation. The warfarin was discontinued, and once the International Normalized Ratio (INR) decreased below 2.2, therapy with intravenous heparin allowed for maintenance of a PTT between 80 and 110 seconds awaiting the target INR of 1.4 or less. On the day of operation, heparin was stopped 4 hours before the scheduled operating time. Upon induction and intubation, necessary monitoring lines, including a five-port Swan-Ganz catheter, were inserted by the anesthesia team. The radial artery cannula revealed a mean arterial pressure (MAP) of 76 mmHg. The LVAD was connected to the main power supply unit. Four skin incisions were made for the camera and the laparoscopic instruments (Fig. 2). Special attention was paid to the position of the VAD pump and its driver lines. The abdomen was inflated gradually with carbon dioxide to achieve pneumoperitoneum of 15 mmHg. There were minimal hemodynamic fluctuations and variations of the VAD's speed and pulsatile index (PI) during induction, pneumoperitoneum creation, and during the procedure (Fig. 3). The spleen was easily mobilized paying attention not to spill the contents of the abscess, and splenectomy was safely performed. The patient was discharged home in 6 days after appropriate levels of anticoagulation had been achieved. Intravenenous antibiotic therapy was continued for a total of 6 weeks.
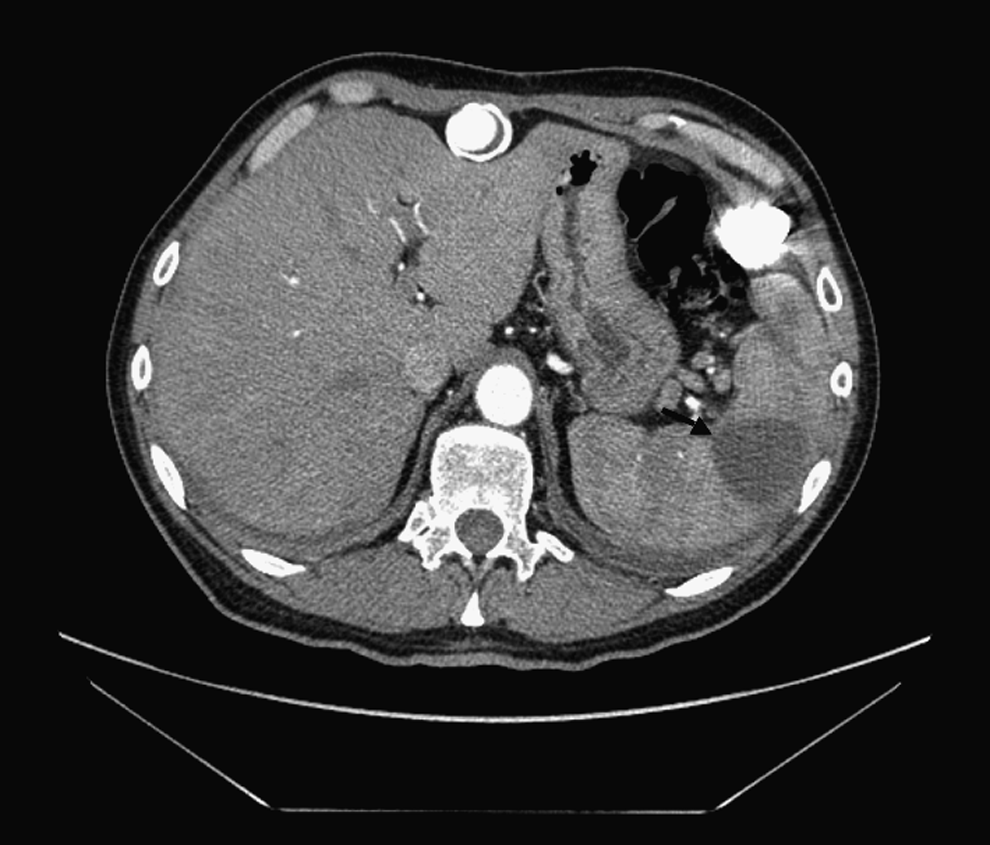
Computed tomography demonstrating a large splenic abscess (arrow).
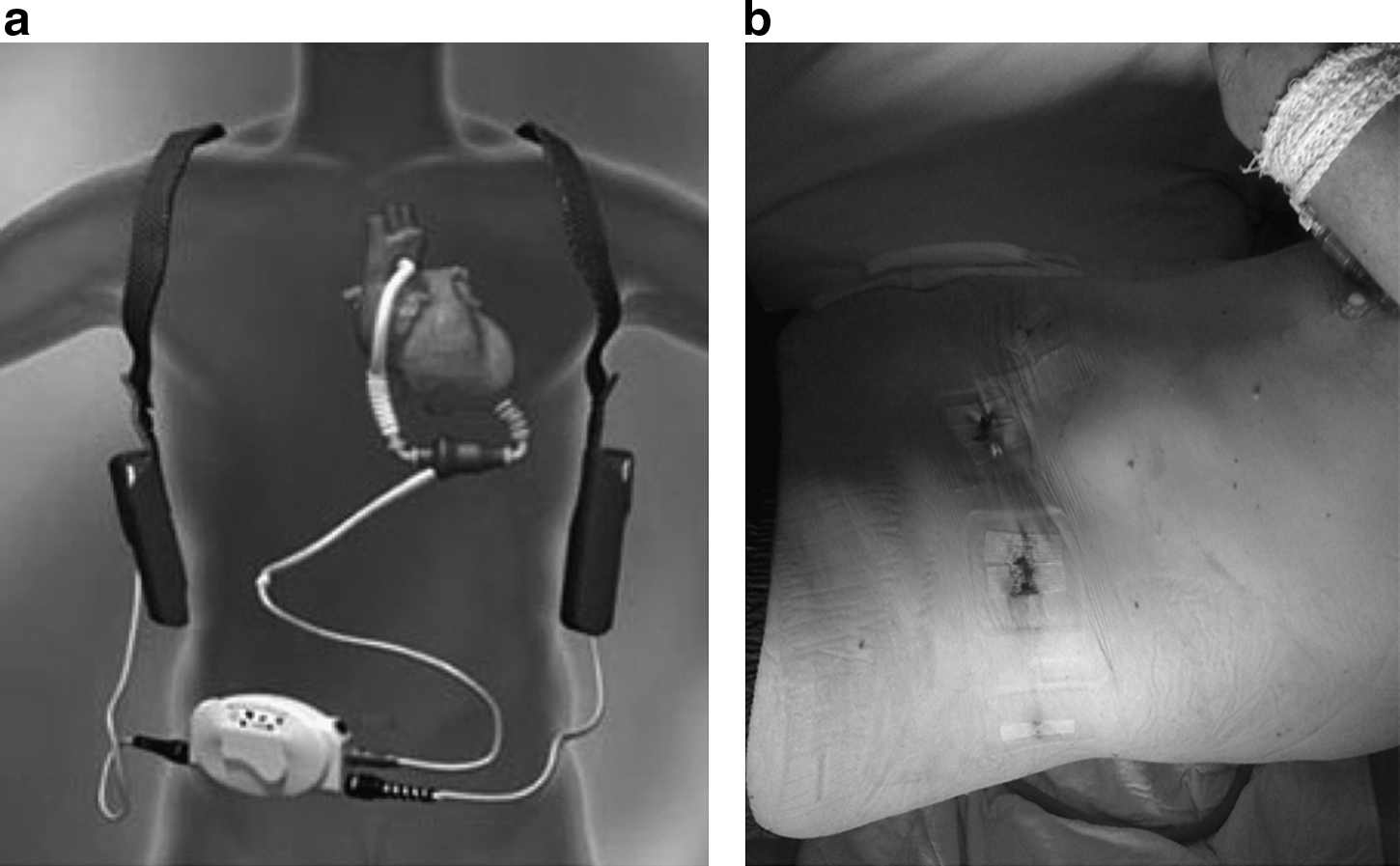
Heartmate® II LVAD
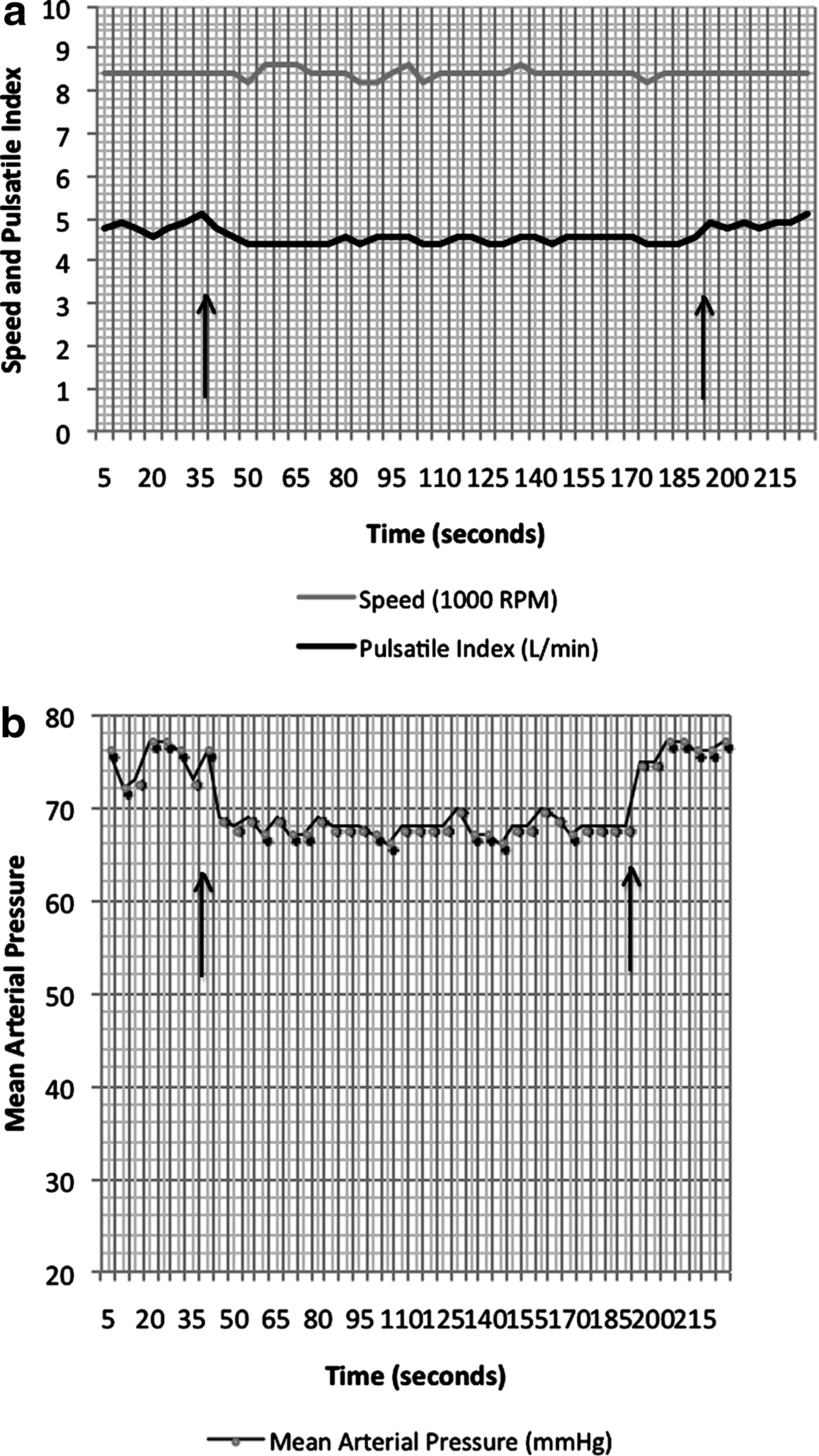
The variation of pump speed and pulsatile index
Discussion
The REMATCH trial revealed that hemodynamic restoration with implantable LVADs not only prolongs survival, but also improves quality of life among patients in heart failure. Consequently, the number of patients on LVAD “destination therapy” has increased as various devices are implanted in heart failure centers around the globe. Heartmate II (Fig. 2) is one of the newer-generation intracorporeal LVADs commonly implanted in our centre.
Considering that the majority of these devices require abdominal wall transgression, the potential for abdominal complications, infectious or otherwise, is substantial. Recent reports suggest that solid-organ complications arise in almost a quarter of patients with implanted LVADs, resulting in the need for frequent noncardiac surgical interventions. 2 Considering the fragile physiologic state of these patients, a laparoscopic approach to abdominal surgery becomes very attractive. Although there are several published case series of patients with circulatory support undergoing open abdominal surgery, the safety of laparoscopy in this patient population has not been studied. An extensive review of the literature yielded a paucity of case reports, none of which dealt with solid-organ surgery (Table 1).
BiVAD, biventricular assist device; LVAD, left ventricular assist device.
The significant physiologic impact of pneumoperitoneum, in the context of compromised myocardial performance, may lead to hemodynamic compromise regardless of circulatory assistance. Even though the function of Heartmate II LVAD depends on both pre-load and afterload, the principles of Starling's law do not apply when either of these physiologic parameters is significantly altered. 3 Trendelenburg position and pneumoperitoneum lead to depressed native cardiac output, elevated filling pressures, and worsening hypercarbia 4 and may significantly impair the LVAD pump flow. Any alterations in afterload, especially significant peripheral vasoconstriction, may further expose the patient to a risk of malperfusion and cerebral anoxia. Figure 3 demonstrates a stable pump speed during the induction and pneumoperitoneum stages of the procedures. The MAP and PI, however, show more variation. In the absence of pneumoperitoneum, the MAP and PI were 75.5±1.6 mmHg and 4.9±0.1 L/minutes, respectively, whereas during the procedure the same parameters were 67.9±0.9 mmHg and 4.5±0.1 L/minutes. Catecholamine surges during induction and pneumoperitoneum are expected to increase the peripheral resistance; however, an increase in the mean blood pressure is not seen. Although these are not clinically significant hemodynamic changes, they confirm the pump's strong dependence on the venous return (preload). Adequate fluid management during the procedure thus becomes paramount.
Because of the position of the device itself and its drive lines, the laparoscopic surgical approach may need to be modified to perform the procedure safely. In the case of laparoscopic splenectomy, particular care has to be taken when positioning the patient in the right lateral decubitus position. The subcostal incision and port placement must not compromise the “pocket” nesting the device or the LVAD itself. Any such manipulation could predispose the patient to deleterious consequences—mechanical and infectious, alike.
Conclusion
Laparoscopic procedures can safely be performed in patients with LVADs. Physisologic changes associated with anesthesia and pneumoperitoneum appear to be subclinical and do not seem to affect the function of the device. Each surgical procedure, however, requires both careful operative planning and perioperative monitoring.
Footnotes
Disclosure Statement
No competing financial interests exist.