
Abstract
Abstract
Background:
After being introduced in 1992, laparoscopic adrenalectomy has been accepted as the gold standard today for benign diseases. The need is now being realized for newer innovations to further reduce the trauma of surgical access. We report our experience and outcome of the first case series of single-port access adrenalectomy by using SILS™ port.
Methods:
Between June 2009 and November 2010, 6 patients with adrenal tumors underwent single-port access adrenalectomy via SILS port. The device was placed through a single 3 cm incision. The patients' demographics, adrenal mass characteristics, operative time, conversion rate, intraoperative and postoperative complications, and postoperative pain score were measured. Five patients underwent adrenalectomy by using the retroperitoneal approach and 1 by using the laparoscopic transperitoneal approach.
Results:
Three men and 3 women with mean age 51 years (range, 37–67) underwent single-incision adrenalectomy. The mean tumor size was 3.3 cm (range, 1.5–6). Three of these cases were Conn's syndrome, and the remaining 3 were incidentaloma. No significant complications or conversions to the conventional procedure were recorded. The mean operative time was 121 minutes (range, 70–165). The mean hospital stay was 2.7 days (range, 2–4). No local recurrences or hormonal relapse have been recorded to the present with a median follow-up of 12 months (range, 3–20).
Conclusions:
In our short experience, single-port access adrenalectomy seems to be safe and feasible in improving the advantages of laparoscopic approach, especially in terms of cosmesis, but further randomized controlled trials are needed to evaluate the benefits of this novel approach.
Introduction
We would like to report our initial experience with 6 cases of single-port access adrenalectomy by using SILS™ (Covidien, Norwalk, CT) device. The aim of the current study is to verify the feasibility and safety of single-port access adrenalectomy.
Patients and Methods
From June 2009 to Nov 2010, 6 patients with adrenal mass underwent single-port access adrenalectomy at our institution. Institutional Review Board approval was obtained to perform this procedure in our department. All patients were fully informed about the procedure with the possibility of conversion to conventional laparoscopy and open surgery.
All patients requiring adrenalectomy were included in the study. The exclusion criteria were those who had malignant adrenal tumor, previous surgery in the retroperitoneal area, and contraindications to general anesthesia or laparoscopy. Three patients had Conn's syndrome secondary to aldosterone-producing adrenal mass. Preoperatively, all the patients with aldosteronoma were medically optimized with their hypertension controlled and hypokalemia corrected. The remaining 3 patients had adrenal incidentaloma that was larger than 4 cm or imaging characteristics atypical for an adenoma, cyst, or myelolipoma.
The data were prospectively collected by using our hospital database. Data collected included the patients' demographics with regard to patient age, body mass index (BMI), adrenal mass characteristics, operative time, conversion rate, intraoperative and postoperative complications, and outpatient follow-up. The visual analog scale (VAS) pain score was recorded on 48 hours after the operation. The pain scale used ranged from 1 (minimal pain) to 10 (worst). The mean follow-up was 12 months (range, 3–20 months).
Due to their retroperitoneal location, the laparoscopic approach to adrenals may be either transperitoneal or retroperitoneal. The retroperitoneal approach to the adrenals can be carried out via either the flank or the back (posterior). The posterior retroperitoneal approach is the preferred method in our institution, and the details are provided in the following discussion. For the transperitoneal approach with a single-access port, the operative techniques are described in detail elsewhere.10,11
The procedure is performed under general anesthesia with the patient in a prone jack-knife position (Fig. 1). For the procedure, we used the SILS Port System (Covidien). This is a multi-instrument–access port that allows three laparoscopic instruments to be concurrently used through separate trocars sited within the port. An incision of 3 cm is made in the retroperitoneal region beneath the 12th rib. The incision is deepened, and the retroperitoneum is entered. The SILS (Covidien) port is inserted (Fig. 2), and gas insufflation is started to a pressure of 15–18 mmHg. A 5 mm 30 degree Endoeye™ (Olympus Medical, Tokyo, Japan) is introduced. Further dissection of the retroperitoneal space is performed by bluntly pushing the retroperitoneal fatty tissue downward, thereby exposing the area of the adrenal. The adrenal gland is identified at the superior pole of the kidney. Next, the mobilization of the upper pole of the kidney is performed. Dissection of the adrenal gland then begins from medial to lateral aspect (Fig. 3). On the right side, the vena cava is identified and superiorly approached to identify the short adrenal vein. This vessel is secured between hemolocks and divided. The gland is then laterally and cranially dissected to complete its removal. For the left-sided adrenalectomy, it is required that the upper pole of the kidney be completely mobilized, as the lower pole of the adrenal lies in front of the kidney. Only then can the inferior part of the gland be dissected. The main vein from the left adrenal joins the diaphragmatic vein between the upper pole of the kidney and the spine. After securing this vein, the gland is further mobilized. The completely dissected gland is removed by using an Endocatch retrieval bag (Covidien). Homeostasis is secured, and the irrigation is carried out if required. A drain is left in situ through the incision when necessary. The wound is closed in layers with absorbable sutures.

Patient in the prone jack-knife position and marked incision site.
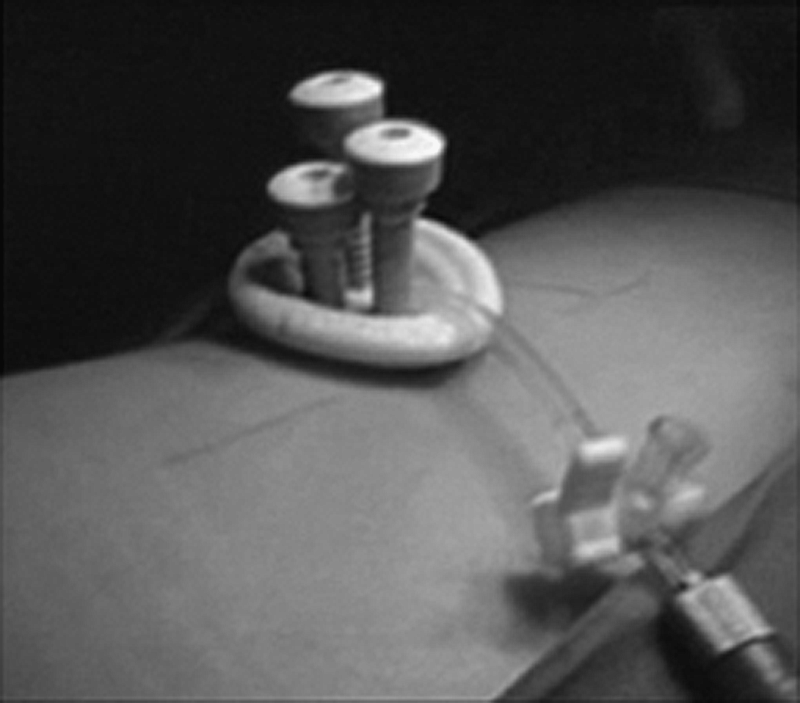
SILS port with three 5 mm trocar after insertion.
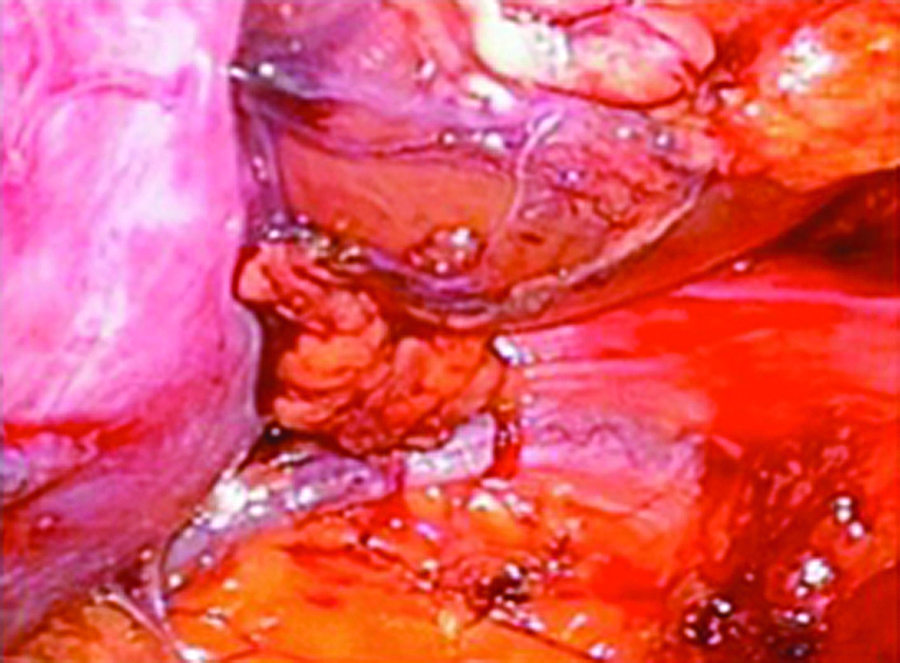
Dissection of the adrenal gland.
Patients are encouraged oral feeding as soon as full consciousness is regained. Full mobilization is encouraged since the day of surgery. Analgesia is provided and administered on request, and pain is recorded by using the VAS pain score.
Results
A total of 6 patients underwent single-incision adrenalectomy between June 2009 and November 2010. This included 3 men and 3 women. The mean age was 51 years (range, 37–67). The mean BMI was 23.5 kg/m2 (range, 21–28.5) with only 1 patient (BMI of 28.5 kg/m2) in the overweight group. The mean tumor size was 3.3 cm (range, 1.5–6). Three of these cases had tumors that were hormonally active, thereby causing the patients to have hyperaldosteronism (Conn's syndrome); whereas the remaining 3 patients had adrenal incidentaloma that was larger than 4 cm or imaging characteristics atypical for an adenoma, cyst, or myelolipoma (Table 1). Three cases had significant previous surgical history including excision of parathyroid adenoma in one, adrenalectomy on the contra-lateral side for malignancy in the second, and low anterior resection for rectal cancer in the third case.
BMI, body mass index.
Five patients underwent laparoscopic adrenalectomy by using the retroperitoneal approach and 1 by using the transperitoneal approach on the left side. The transperitoneal approach was performed because of the surgeon's preference and to avoid the extensive retroperitoneal fat area. All the cases were completed by the single-port access approach. There was no conversion to either conventional laparoscopy or open surgery. The mean operative time was 121 minutes (range, 70–165). No intraoperative and postoperative complications were recorded. There was no mortality. None of the cases met with a significant blood loss requiring transfusions. Drain was inserted for one patient, which was removed on postoperative day 2 without any complication.
The mean hospital stay was 2.7 days (range, 2–4). The mean VAS score at 48 hours was 2.2 (range, 1–3). No local recurrences or hormonal relapse were recorded to the present with a median follow-up of 12 months (range, 3–20). There was no significant wound-related problem (Table 2).
VAS, visual analog scale.
Discussion
Endoscopic technique is now considered the standard for adrenal surgery.13,14 The only possible exception to this is a malignancy. The conventional laparoscopy requires at least three incisions and a 2–4 cm incision for the main port, which depends on the size of the adrenal tumors for the specimen extraction. The extra incisions have the potential to increase the risk of pain, bleeding, and visceral injury as well as of compromising the cosmetic outcomes. 14 Further, it has now been shown that the use of fewer and smaller trocars is associated with a reduced postoperative pain, shorter hospital stay, faster return to recovery, and better cosmesis.15,16 Single-incision adrenalectomy in this way is a step further, which in time can prove to be a viable alternative in terms of safety, efficacy, and treatment outcomes.
Endoscopic access to the adrenal can be obtained by either a laparoscopic transperitoneal or a retroperitoneal route (lateral or posterior). It has been demonstrated by various studies that the posterior approach is feasible, safe, widely applicable, and faster. 17 This is probably because of the naturally occurring anatomic planes of the retroperitoneal organs. Moreover, the retroperitoneal space can be easily created with the scope itself. In our study, we have favored the posterior approach.
There are not many published series for single-port adrenalectomy, especially using a multilumen single-port. We report the first case series of posterior retroperitoneal single-port access adrenalectomy by using SILS port. Our study demonstrated that this approach appears to be a valid treatment option for adrenalectomy showing good clinical outcomes with no major complications.
Looking at the history of single-incision adrenalectomy, Kageyama et al. reported the first series of single-incision adrenalectomy in 2004. 18 The surgery was performed without gas inflation or trocar port placement via a single-incision (mean, 5.6 cm; range, 3–9). This procedure was actually not a laparoscopic procedure, but has become the basis of single minimal incision adrenal surgery for further development.
Hirano et al. reported a series of single-port adrenalectomy in 2005. 19 The surgery was performed via a 4.5 cm incision by using a 4 cm rectoscope for direct visualization. Gas insufflation was not used. This technique provided a platform for the evolution of single-port adrenal surgery.
Walz et al. reported performing a 2 cm single-incision retroperitoneoscopic adrenalectomy by using two ports. 14 The surgery is performed in a single-hand technique; the operating surgeons holds the camera as well as the working instrument simultaneously.
Another matched pair comparison was published by Tao-ping Shi et al. 20 They performed single-port adrenalectomy by using the laparoendoscopic single-site port. They accessed the adrenal via a lateral retroperitoneal approach and found the approach to be safe and feasible. Apart from these, there have been a couple of other reports of transperitoneal adrenalectomy.21,22 A comparison between all these studies and our own has been given in Table 3. No previously published prospective studies have reported on endoscopic adrenalectomy using a single multilumen port via the posterior retroperitoneal approach. Nevertheless, the results from these studies should be carefully considered until larger series of patients subjected to long-term follow-up evaluation can be analyzed.
Lat., lateral; Post., posterior.
Some points that can be made against the single-incision technique include first that the operative techniques are not technically easily and widely applicable due to issues such as loss of triangulation, clashing of instruments, reduced work space, and increased operative time. However, further innovation in instrumentation and visualization has now become commercially available. Newer instruments such as special multilumen ports that allow for simultaneous instruments insertion, articulating and bent instruments, and improvised, smaller laparoscopes have resolved many of these technical difficulties. Interestingly, a recent study compared the currently available multilumen devices including the SILS port including the differences in terms of the insertion method, ease of use, instrument maneuverability, and performing tasks. 23 We do not think that any device is more superior compared with the other, but understanding and familiarity of the device are more crucial in ensuring success and safety of the procedure.
Another problem with the retroperitoneal approach is the reduced space making the use of articulating instruments limited and technically difficult. However, we were able to accomplish most of the tasks such as dissection and retraction by using conventional instruments with little difficulty even in a patient with a BMI of 28.5 kg/m2. From our experience and other reported studies, 20 we believe that obesity is not a contraindication for the single-port technique. We attributed this finding to the flexibility of the port device that we were using as well as the improvised and smaller laparoscope. Finally, we believe that the single-port access approach takes only modestly longer to perform compared with the conventional laparoscopy. The expectation is that the operative time should be reduced as the surgeons become more experienced with the devices.
Conclusions
In conclusion, based on the results and other reported series, the single-port access adrenalectomy seems safe and feasible. The distinct benefit from this technique is noticeable from the improvement of cosmesis (Fig. 4). Despite these generally favorable results, a prospective, randomized trial is needed to compare the efficacy of this novel approach over the standard laparoscopy for adrenalectomy.
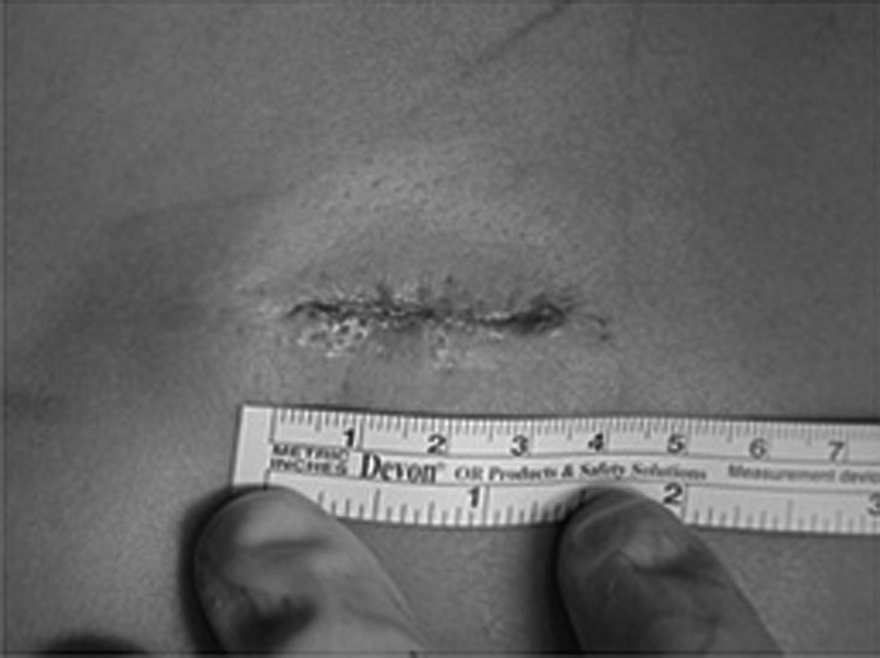
Cosmetic result immediately after surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.