
Abstract
Abstract
Introduction:
Single-incision laparoscopic cholecystectomy (SILC) promises improved cosmesis and may further minimize the invasiveness of intraabdominal interventions but cannot come at the expense of patient safety. This study describes the evaluation of a novel 5-mm instrument designed for SILC that maintains an equivalent critical view to that obtained with standard multiport laparoscopic cholecystectomy (MLC).
Materials and Methods:
Sixteen animals were randomly assigned to one of four study arms. Four techniques for laparoscopic cholecystectomy were used: standard four-port MLC, three-instrument SILC (SILC-A), three-instrument SILC using a suture for lateral retraction (SILC-B), and three-instrument SILC using the novel instrument for retraction (SILC-C). Each case was timed and video-recorded. The video was cropped to obscure the method of retraction and evaluated by five experienced laparoscopic surgeons blinded to the technique used. Each case was rated subjectively on a safety and visualization scale of 1–4.
Results:
SILC-A and SILC-B cases were significantly longer in duration than both SILC-C and MLC cases. The safety and visualization scale results were lower for the SILC-A technique but were equivalent for the MLC, SILC-B, and SILC-C techniques.
Conclusion:
This study introduces a novel instrument for gallbladder retraction. In this initial evaluation, the new instrument showed encouraging results in its ability to generate good visualization, support the safe critical view technique, and reduce the length of the procedure.
Introduction
Recently, many new platforms, instruments, and trocars have been developed for single-site surgery with the purpose of improving the ease and accessibility of this technique. Cholecystectomy, as the most common laparoscopic surgical procedure, seems like the perfect entrée for many into single-incision surgery, but as a growing number of surgeons embrace this new field, safety is a real concern.
The “critical view of safety,” initially espoused by Strasberg et al., 4 has become the gold standard method for safe laparoscopic cholecystectomy. This technique is defined by clear visualization of the cholecystic hilar structures and is made possible by the simultaneous retraction of the gallbladder in two opposing vectors. The fundus is retracted cephalad while the infundibulum is retracted laterally, thus maximizing the cystic duct–common bile duct angle. This bidirectional retraction is optimally accomplished with two instruments.
In an attempt to avoid the clashing engendered by multiple instruments vying for space at the single-access site, most single incision laparoscopic cholecystectomy (SILC) techniques use some variation of a three-instrument cholecystectomy.5,6 This method allows for only a single-retraction instrument, leading to inadequate gallbladder retraction and puts the major structures at risk. 7
This study introduces a novel handheld retractor, designed to provide the equivalent retraction of two separate graspers while only occupying the space of one. This new instrument's retraction was compared for safety and adequacy of visualization with that produced by standard multiport laparoscopic surgery (MLC) and two common methods of SILC.
Materials and Methods
This study was approved by our institution's Animal Care and Use Committee. Sixteen male mongrel dogs weighing 20–30 kg were used for this study. Each animal was previously part of an unrelated acute or survival study not involving the liver or gallbladder and enrolled in this study after completion of their primary protocol.
T-retractor instrument
The novel instrument consists of a single 5-mm shaft with a hinged 3-cm T-bar affixed to the end. Mounted at either end of the T-bar is an individually actuated grasper (Fig. 1). Each grasper can be actively opened with a second laparoscopic instrument but is maintained in a closed configuration by an internal spring (Fig. 2). The hinged T-bar allows the two grasping ends to functionally retract the fundus of the gallbladder cephalad while the infundibulum is retracted laterally.

T-retractor instrument.

A second instrument is used to individually open the graspers built onto each end of the T-retractor. Grasping force is maintained by a spring built into the shaft.
This instrument was hand-built specifically for this study and is not currently commercially available.
Study
Each animal was randomly assigned to one of four study arms. Four animals in each arm underwent one of the following methods of laparoscopic cholecystectomy:
The MLC Group received traditional four-port MLC.
The SILC-A Group received three-instrument SILC. For this technique three trocars were placed at the “umbilicus”: One trocar was used for the camera, one for the dissector, and the third for a grasper with which the lower third of the gallbladder was retracted in a generally cephalolateral direction (Fig. 3).
Single-incision laparoscopic cholecystectomy-A. A single retraction instrument provides generally cephalolateral retraction obscuring the cystic duct–common bile duct angle.
The SILC-B Group received suture-assisted SILC. The same trocar and instrument configuration was used as for SILC-A, but in addition a single suture was placed through the gallbladder infundibulum for lateral retraction while a standard grasper was used for cephalad fundal retraction (Fig. 4).

Single-incision laparoscopic cholecystectomy-B. Sutured retraction. A single grasper retracts the fundus, while a suture placed through the abdominal wall retracts the infundibulum.
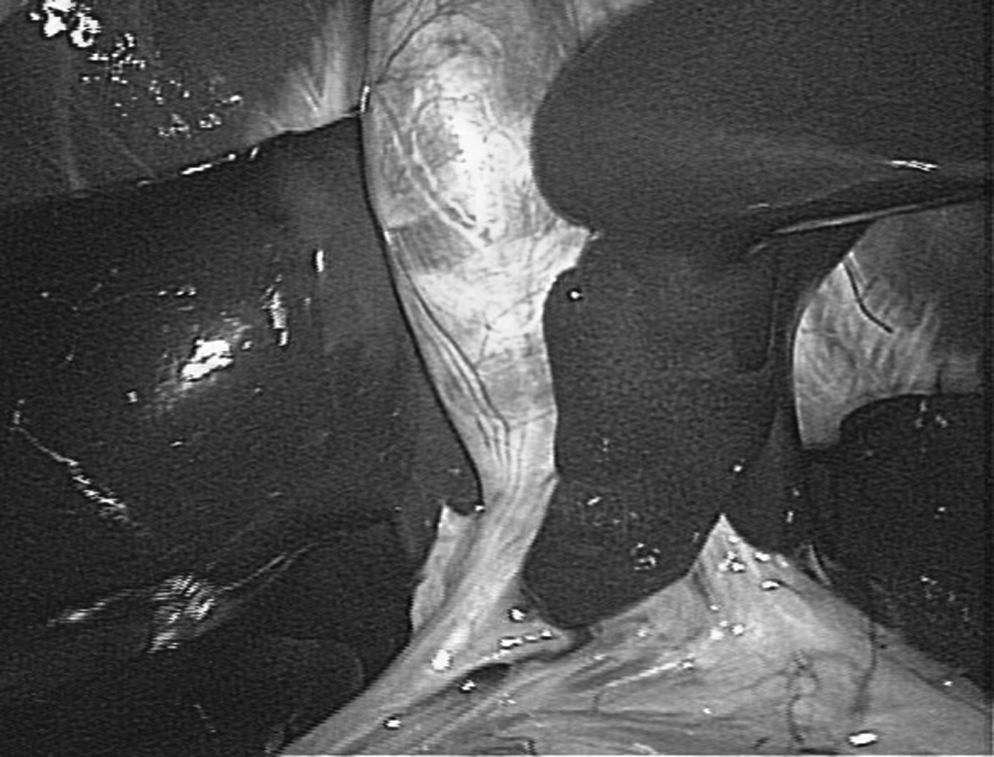
The SILC-C Group received the novel instrumentation. For this technique, three trocars were placed at the “umbilicus.” One trocar was used for the camera, one for the dissector, and the third for the novel T-retractor instrument (Fig. 5).

Single-incision laparoscopic cholecystectomy-C. T-retractor. Critical view.
Each case was timed and video-recorded. The video was cropped to obscure the method of retraction and evaluated by five experienced laparoscopic surgeons blinded to the technique used. Each case was rated subjectively on a safety and visualization scale of 1–4 (1=poor, 4=excellent). A P value of <.05 was considered significant.
Results
The mean operative times for SILC-A and SILC-B cases were 54.25±11.62 and 52.75±11.70 minutes, respectively, significantly longer than both MLC and SILC-C cases, which required 29.75±5.32 and 30.75±1.71 minutes, respectively (Table 1).
MLS, multiport laparoscopic cholecystectomy; NS, not significant; SILC, single-incision laparoscopic cholecystectomy.
Respective mean safety and visualization scale results for MLC cases were 3.75±0.50 and 3.75±0.50, for SILC-A cases were 2.0±.082 and 2.25±0.96, for SILC-B cases were 3.25±0.50 and 3.63±0.48, and for SILC-C cases were 3.50±0.58 and 3.75±0.50. There was no significant difference in scores among MLC, SILC-B, and SILC-C in regards to the safety of the technique and the visualization of the structures, but all three techniques had significantly better scores than SILC-A (Table 1).
Discussion
Laparoscopic cholecystectomy is a procedure with a well-established safety profile. It is highly standardized and is easily taught to trainees. Whether SILC bestows any patient benefit other than improved cosmesis remains a matter of speculation and awaits larger trials and more sensitive evaluation tools. 8 At best, the benefits of SILC are likely to be modest and thus must not compromise the exemplary safety profile of standard MLC.
Two general methods have been described for SILC. One involves a single-retraction instrument at the umbilicus rather than the two lateral retractors used in standard MLC. The second method involves some form of static retraction either alone or in combination with the single-retraction instrument. The most common manifestation of the static retraction technique is using sutures to fix the gallbladder to the abdominal wall.3,9–11
Both of these techniques have significant shortcomings. Safe retraction and exposure of the critical view require simultaneous retraction of the fundus cephalad, while the infundibulum is retracted laterally. The single retractor method does not provide this retraction and instead tends to obscure the cystic duct–common bile duct angle by retracting the gallbladder in a general cephalolateral direction.
The static retraction method provides acceptable bidirectional retraction but suffers from its own unique set of limitations. First, there is a need for puncturing the gallbladder, which often results in bile and even stone spillage. In addition, suturing adds an extra level of difficulty that may take this method out of the hands of the average community hospital–based surgeon and junior-level trainee.
An additional difficulty experienced with this method is the fixed nature of the retraction, which precludes dynamic manipulation of the gallbladder during dissection. Dynamic manipulation, commonly used during MLC, restores some of the depth perception lost with laparoscopy and may be especially indispensable in cases of acute cholecystitis or complex anatomy. Dynamic retraction is also valuable during resection of the remaining gallbladder corpus from the gallbladder fossa where inadequate traction can lead to a loss of the correct plane. Lastly, sutures require multiple stab wounds to the abdominal wall, which may add to the pain and morbidity of this technique.
Despite only having a single shaft, the T-retractor provided excellent bidirectional retraction, resulting in excellent safety and visualization scores while maintaining short operative times. This supports the contention that this instrument is easy to use and provides an equivalent critical view to that seen with MLC. Also, robust, continuous, and dynamic manipulation of the gallbladder was easily controlled by the operating surgeon at all times during the dissection.
A T-retractor such as that described may be advantageous in settings other than SILC. It may help facilitate standard cholecystectomy training, by giving the attending surgeon the ability to control the gallbladder with one hand, thereby freeing his other hand to direct a trainee. In a rural or military setting where surgical assistants are in short supply, connecting the retractor to a locking arm may allow the surgeon to operate solo. Lastly, a two-headed T-retractor may also be helpful in other laparoscopic procedures such as colectomy where the surgeon would benefit from wide angle retraction.
We did identify some potentially significant shortcoming with the current design of the instrument. Its predefined distance between grasper heads (3 cm) would render it unable to simultaneously grasp the fundus and infundibulum of a short gallbladder. An additional shortcoming was the spring that kept the jaws apposed. Although adequate for grasping a normal gallbladder, it would likely not generate enough force to maintain its hold on a thickened gallbladder wall such as that found in cholecystitis. Future designs should include the ability to adjust the length of the T-bar and a mechanism for locking the jaws of the graspers.
Optimally, surgeons facile with standard multiport laparoscopy should be able to transition to SILC without sacrificing safety or established surgical principles. This study introduces a novel instrument for gallbladder retraction. In this initial evaluation, the new instrument showed encouraging results in its ability to generate good visualization, support the safe critical view technique, and reduce the length of the procedure. Further study is necessary to confirm whether these benefits can be reproduced in a human trial.
Footnotes
Disclosure Statement
No competing financial interests exist.