
Abstract
Abstract
Background:
Pneumoperitoneum induced to facilitate laparoscopy is associated with splanchnic hypoperfusion, ischemia/reperfusion (I/R) injury, and oxidative stress.
Aim:
This study investigated the effects of pre- and postlaparoscopic conditioning, zinc, pentoxifylline, and N-acetylcysteine on markers of I/R injury of the small intestine in an animal model.
Methods:
Male Sprague–Dawley rats (n=56) were randomized to 1 of 7 treatment groups. Except for group 7 (control group that underwent sham surgery without pneumoperitoneum), pneumoperitoneum was induced in all by use of carbondioxide insufflation under a pressure of 15 mmHg. Group 1 (laparoscopic I/R) was subjected to 60 minutes of pneumoperitoneum. Group 2 (laparoscopic preconditioning plus laparoscopy) was subjected to 5 minutes of insufflation and 5 minutes of desufflation followed by 60 minutes of pneumoperitoneum. Group 3 (laparoscopy plus laparoscopic postconditioning) was subjected to 60 minutes of pneumoperitoneum and 60 minutes of desufflation followed by 5 minutes of insufflation and 5 minutes of desufflation. Group 4 (zinc), group 5 (pentoxifylline), and group 6 (N-acetylcysteine) received a single intraperitoneal injection of zinc (50 mg/kg), pentoxifylline (50 mg/kg), or N-acetylcysteine (150 mg/kg), respectively, 5 minutes before the desufflation period. Animals were killed at the end of the experiments, and small intestine samples were tested for malondialdehyde (MDA), catalase (CAT), glutathione peroxidase (GPX), and superoxide dismutase (SOD).
Results:
There was no significant difference for MDA levels between each other in the groups 1, 2, and 3. But MDA levels were higher significantly in groups 1, 2, and 3 than those of groups 4, 5, 6, and 7. SOD and GPX levels of group 3 were significantly higher than those of groups 1, 2, 4 through 7. According to the SOD levels, there was no significant difference between each other in those of groups 1, 2, 4 through 7. GPX levels of group 3 were significantly higher than those of groups 1, 2, 4 through 7. GPX levels of group 1 were significantly lower than those of groups 5 and 7. The mean CAT level of groups 1 and 2 was significantly lower than that of groups 3, 6, and 7. The mean CAT level of group 3 was significantly higher than that of groups 1, 2, 4 through 7.
Conclusions:
In this animal model of small intestine I/R injury, laparoscopy caused small intestine ischemia as evidenced by elevated markers of tissue I/R injury. This effect was significantly attenuated by zinc, pentoxifylline, and N-acetylcysteine, but not by prelaparoscopy conditioning and postlaparoscopy conditioning.
Introduction
If high-risk patients can be detected before procedure (age, cardiovascular disease, complex and long-duration operations, some gases, increased end-tidal carbondioxide [CO2], and intraabdominal pressure) 4 in whom laparoscopy was planned, complications can be decreased or protected with antioxidant strategies. Recently, several studies addressed the possibility that oxidative stress might be caused by laparoscopic surgery.6–15 Several solutions have been proposed to reduce the deranged hemodynamic effects, including gasless surgery,8,11 use of gases other than CO2,7,12 fluid overload, Trendelenburg positioning, 12 ischemic preconditioning 10 and postconditioning, 6 and various pharmacologic therapies.6,13,14
Effective prevention strategies are still needed, because, to our knowledge, none of these approaches to prevent laparoscopy-related I/R small intestine injury have been widely adopted. In this study, in an animal model, we tested the effect of pre- and postlaparoscopic conditioning, zinc, pentoxifylline, and N-acetylcysteine, in preventing small intestine injury caused by pneumoperitoneum as measured by tissue markers of oxidative stress.
Materials and Methods
The study was approved by the Kahramanmaras Sutcuimam University Animal Care and Ethics Committee. Male Sprague–Dawley rats (n=56; weight, 300–350 g) were housed in Macrolon cages, 3 rats per cage, at 20–22°C under a 12:12 light/dark cycle. Rats were fed a commercial pellet diet and tap water ad libitum. We have designed a randomized study and was blind for the measurement of biochemical analyses.
Rats were randomized to 1 of 7 treatment groups. Except for group 7 (the control group that underwent sham surgery without pneumoperitoneum), pneumoperitoneum was induced in all rats using CO2 insufflation. Rats were anesthetized with ketamine (im, 50 mg/kg), and after proper preparation of the surgical field, an 18-G Abbocath catheter was inserted into the abdominal cavity below the xiphoid process and connected to an insufflator tube. 5 Carbondioxide was then instilled to a pressure of 15 mmHg using an abdominal CO2 insufflator (Karl Storz GmbH, Tutlingen, Germany). Group 1 was subjected to 60 minutes of pneumoperitoneum. Group 2 was subjected to 5 minutes of insufflation and 5 minutes of desufflation followed by 60 minutes of pneumoperitoneum. Group 3 was subjected to 60 minutes of pneumoperitoneum and 60 minutes of desufflation followed by 5 minutes of insufflation and 5 minutes of desufflation. Groups 4, 5, and 6 received a single intraperitoneal injection of zinc (50 mg/kg), pentoxifylline (50 mg/kg), or N-acetylcysteine (150 mg/kg), respectively, 5 minutes before the desufflation period.
Biochemical analyses
Animals were killed at the end of the experiments. We have made a standard resection of small bowel according to the segment and length. Reperfusion periods were 60 minutes in all of the animals. Following a midline abdominal incision, the adjacent side of the ileocecal junction was localized, and 10 mm proximal to the junction was accepted as terminal ileum and that segment was removed. After the terminal ileum was dissected of fat and connecting tissue (each 10-mm long), it was sent to the biochemistry department.
Small intestine samples were tested for malondialdehyde (MDA), CAT, GPX, and SOD activity. Tissue specimens were washed with 0.9% sodium chloride to remove hematoma, dried, and stored in plastic bottles at 20°C until biochemical analyses were carried out. At the time of analysis, tissue samples were weighed, placed in 1.15% potassium chloride solution, and homogenized for 15 minutes at 14,000 rpm. Aliquots of homogenates were centrifuged at 5000 rpm for 30 minutes, and supernatants were analyzed for GPX, CAT, and SOD. MDA was measured using the Modified Okawa method, absorbance of thiobarbituric acid–MDA. 15 GPX was measured by nicotine amide adenine dinucleotide phosphate reduction at 340 nm, and CAT was measured spectrophotometrically by the disappearance of hydrogen peroxide (H2O2) at 230 nm. 16 SOD was determined as described by Fridovich. 17 This method employs xanthine and xanthine oxidase to generate superoxide radicals, which react with 2-(4-iodophenyl)-3-(4-nitro phenol-s-phenyl tetrazolium chloride) to form a red formazon dye. SOD is measured by the degree of inhibition of this reaction. The concentration of plasma lipid peroxidation (total MDA) was determined using the Okawa method. Protein was measured according to Lowry et al. 18 Results were expressed in nanomoles per milligram protein (nmol/mg protein).
Statistical analyses
All variables were expressed as medians and ranges. All data were processed using Statistical Package for the Social Sciences (SPSS) 9.05 for Windows® (SPSS, Chicago, Illinois). Differences between groups were evaluated using Kruskal–Wallis and Mann–Whitney U tests. P values less than .05 were considered statistically significant.
Results
Rats in all study groups survived until the end of the experiment. Mean value±standard deviation of MDA, SOD, CAT, and GPX has been shown in Table 1. Levels of oxidative stress markers taken from the intestine tissue samples are shown in Figures 1–4. MDA concentrations in groups 1, 2, and 3 were significantly higher than those in groups 4 through 7 (P<.05; Fig. 1). SOD and GPX concentrations in group 3 were significantly higher than those in groups 1, 2, and 4 through 7 (P<.05; Figs. 2 and 3). Even, SOD concentrations were lower in group 1 than in group 7, however that was not significant (Figs. 2 and 3). According to the GPX levels, there was no significant difference between each other in those of groups 1, 2, 4, and 6. GPX levels of group 1 were significantly lower than those of groups 5 and 7. The mean CAT concentration in group 3 was significantly higher than that of groups 1, 2, 4 through 7 (P<.01). The mean CAT concentration in groups 1 and 2 was significantly lower than that of groups 3, 6, and 7 (P<.01; Fig. 4). There was no statistical difference in groups 1, 2, 4, and 5, between each other (P<.05; Fig. 4).
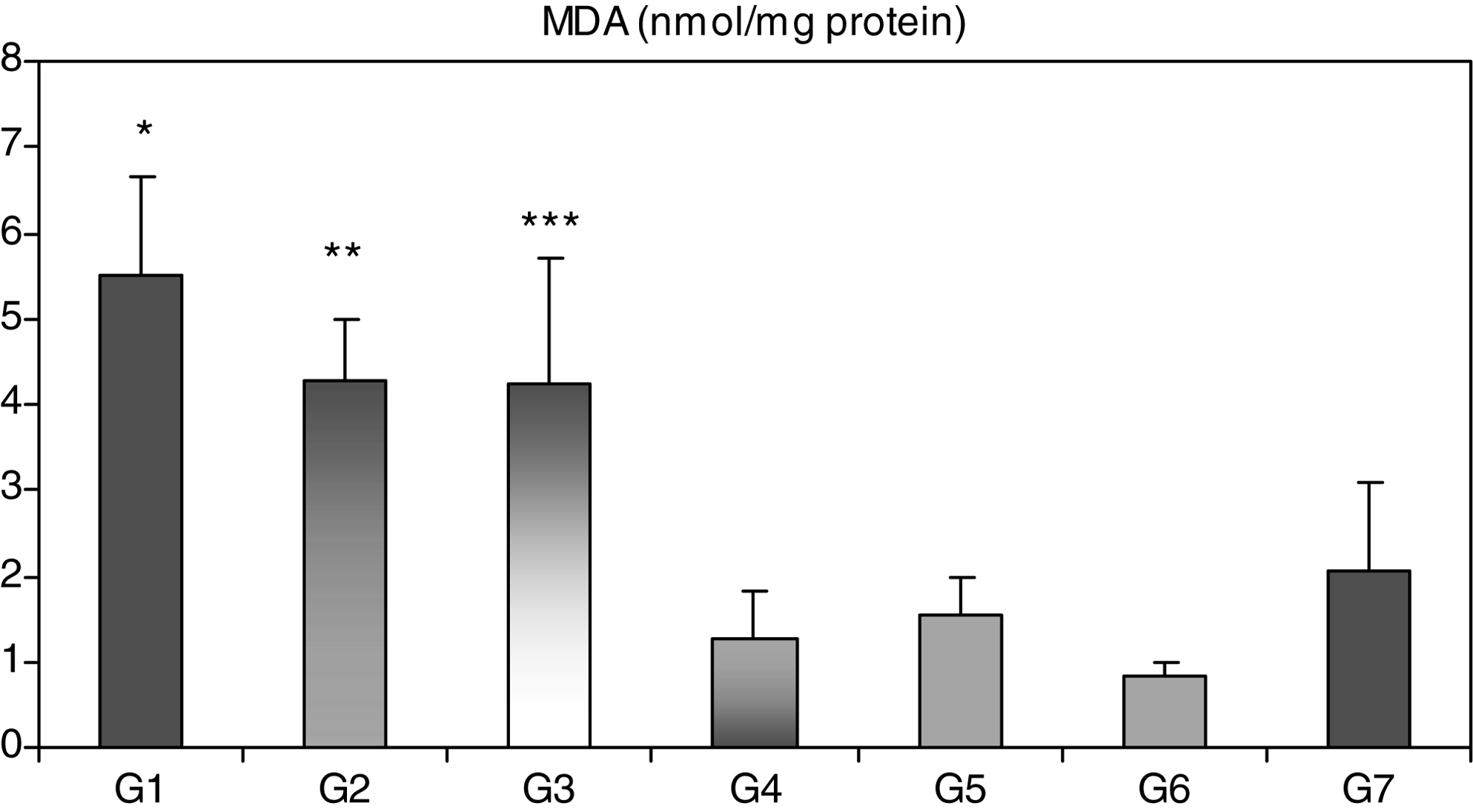
Malondialdehyde (MDA) levels (nmol/mg protein) in small intestine tissue after animals were killed following one of the seven procedures (see explanation in the legend). (*) MDA levels of group G1 were significantly higher than those of groups G4, G5, G6 (P=.001), and G7 (P=.002). (**) MDA levels of group G2 were significantly higher than those of groups G4, G5, G6 (P=.001), and G7 (P=.003). (***) MDA levels of group G3 were significantly higher than those of groups G4, G5, G6 (P=.001), and G7 (P=.011).
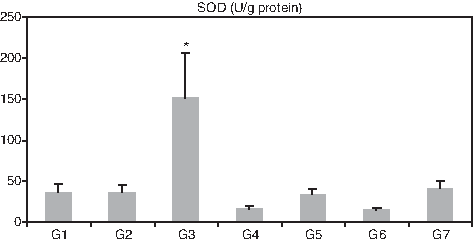
Superoxide dismutase (SOD) levels (U/mg protein) in small intestine tissue after animals were killed following one of the seven procedures (see explanation in the legend). (*) SOD levels of group G3 were significantly higher than those of groups G1, G2, G4, G5, G6, and G7 (P=.001).
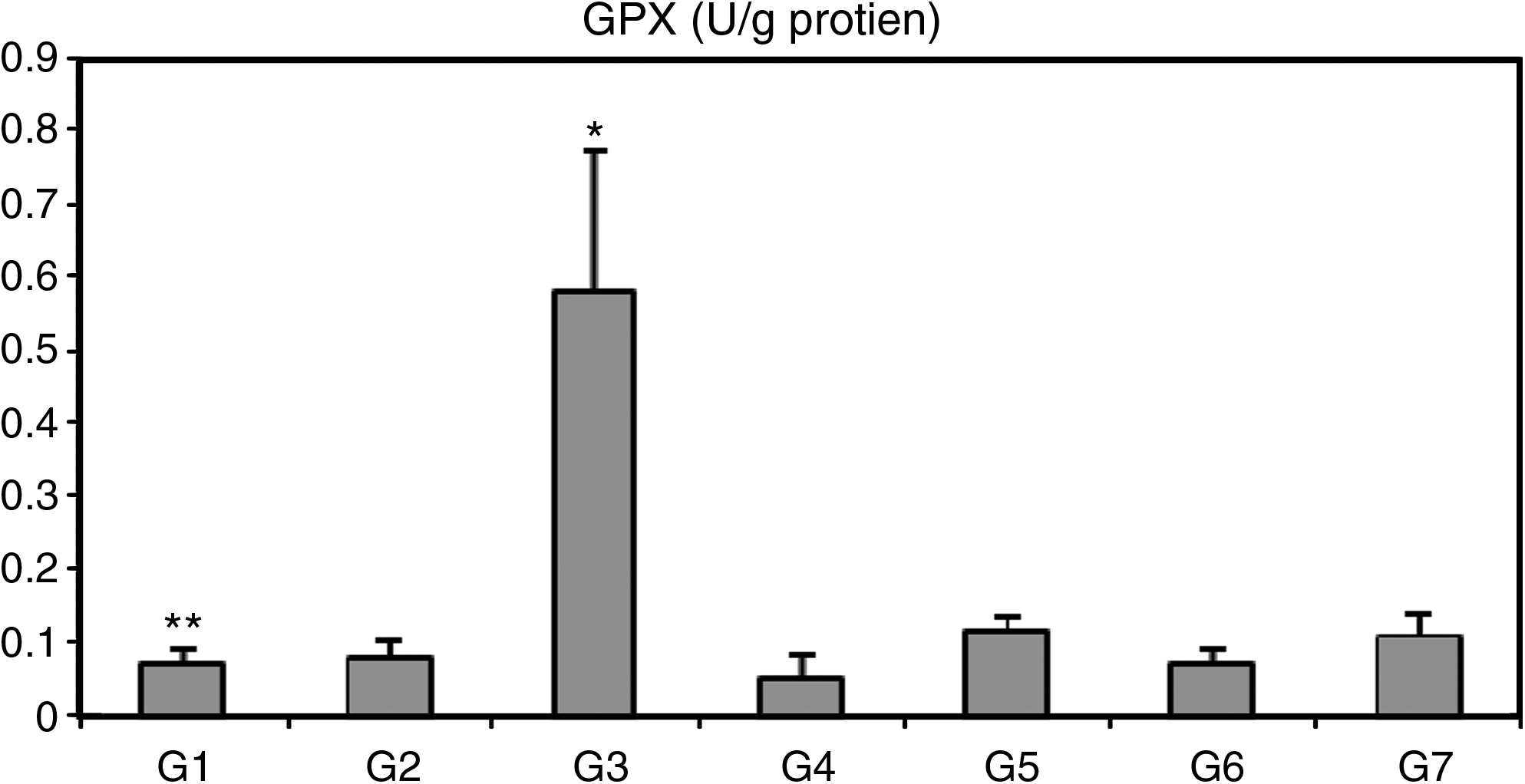
Glutathione peroxidase (GPX) levels (U/mg protein) in small intestine tissue after animals were killed following one of the seven procedures (see explanation in the legend). (*) GPX levels of group G3 were significantly higher than those of groups G1, G2, G4, G5, G6, and G7 (P=.001). (**) GPX levels of group G1 were significantly lower than those of groups G5 and G7 (P=.005).
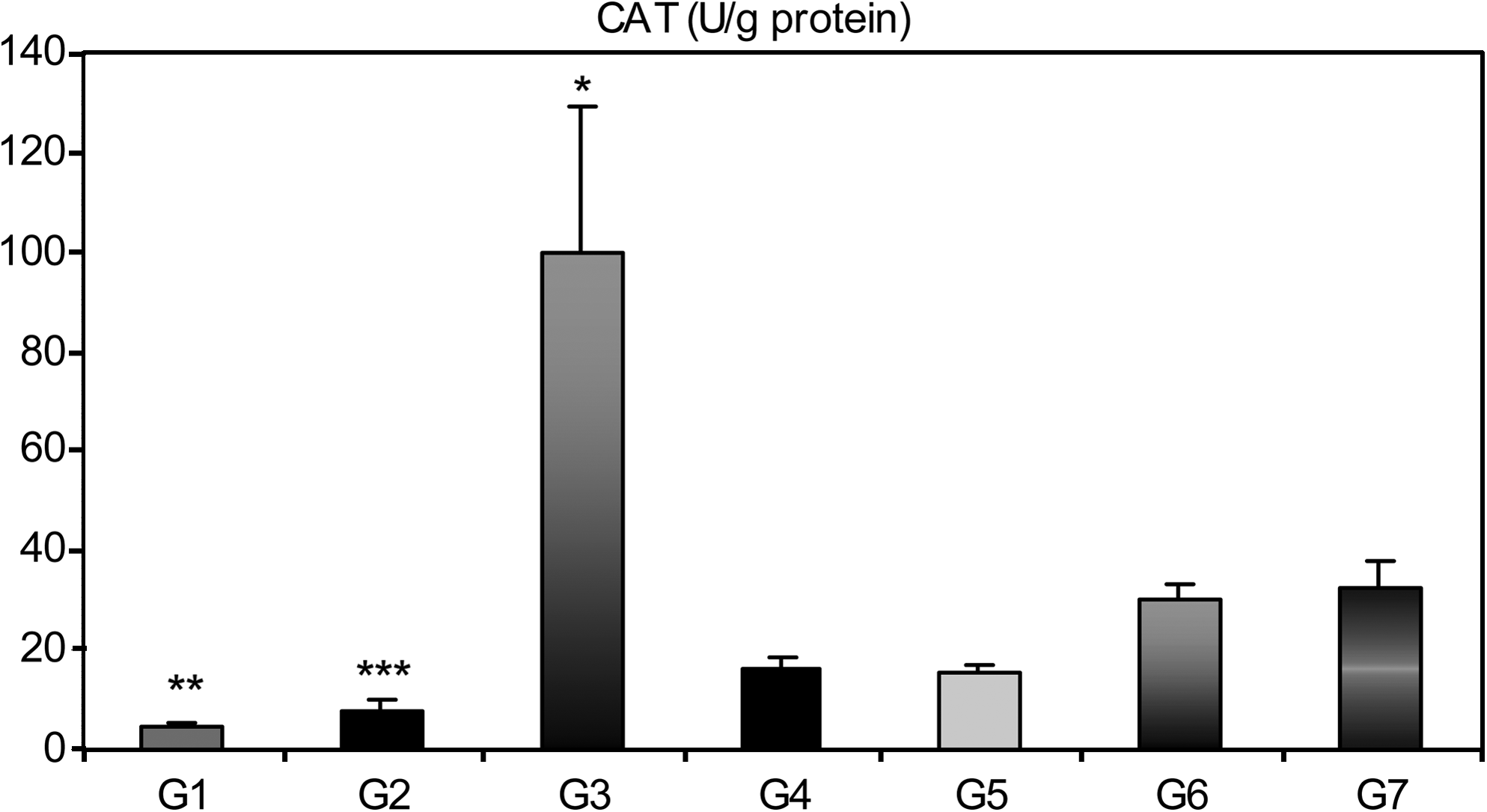
Catalase (CAT) levels (U/mg protein) in small intestine tissue after animals were killed following one of the seven procedures (see explanation in the legend). (*) The mean CAT level of group G3 was significantly higher than that of groups G1, G2, G4, G5, G6, and G7 (P<.01). (**) (***) The mean CAT level of groups G1 and G2 was significantly lower than that of groups G3, G6, and G7 (P<.01).
MDA, malondialdehyde; CAT, catalase; SOD, superoxide dismutase; GPX, glutathione peroxidase.
Discussion
Various tissue markers of oxidative stress have been measured to evaluate the effects of pneumoperitoneum on I/R injury of splanchnic organs. ROS, overproduced during oxidative stress, are potent oxidizing and reducing agents that can directly damage cellular membranes by lipid peroxidation.19–21 Peroxidation of endogenous lipids leads to conversion of reduced glutathione to glutathione disulfide.19–21 MDA is an end product derived of peroxidation of polyunsaturated fatty acids and related esters; thus, MDA tissue levels are a valid reflection of lipid peroxidation.
Another line of cellular defense against free radicals is a system of 3 enzymes: SOD, CAT, and GPX. SOD catalyzes the conversion of superoxides to H2O2, which is subsequently converted to water and oxygen by CAT or GPX. Because it plays such a key role in cellular defense against free radicals, SOD is also an important indicator of the oxidative state.19–21 Laparoscopy-induced I/R damage has been shown in previous studies.1–4 In all of those studies, the marker of oxidative stress MDA was increased and antioxidants were decreased in I/R groups by 14–15 mmHg pressure in intestine. Similarly, in our study, MDA increased in I/R group and antioxidants CAT and GPX decreased significantly according to group 7. But when group 1 was compared with group 7, SOD was lower in group 1, not significantly. That means antioxidant enzyme such as SOD has not decreased enough and still protecting from I/R damage in group 1. Reason of this may be inadequate I/R period. Also previous studies have used 280±15 g rats in weight, we used rats 300–350 g in weight. In other studies, insufficient pressure for I/R in the heavy-weight rats may cause this condition.
Ischemia and following reperfusion is known more harmful than ischemia alone. Precondition is a phenomenon that is used to lessen tissue damage viz, if the blood supply to an organ or a tissue is halted for a short time (usually less than 5 minutes) and then restored two or more times so that blood flow is resumed, the downstream cells of the tissue or the organ are robustly protected from a final ischemic insult when the blood supply is cutoff entirely and permanently.22,23
Precondition has been first shown in dog myocard by Murry et al. 23 Ischemic precondition is one of the rare methods that has shown to increase tissue resistance against I/R damage in experimental and following clinical trials. 23 Recently, postcondition has been reported protective against I/R damage as precondition. It was first determined by Zhao et al. 24 in heart in 2002. The definition of ischemic postcondition is the short periods of ischemia and reperfusion in the early period of reperfusion after prolonged ischemia. 25
While precondition protects both ischemia and reperfusion damage, postcondition protects directly reperfusion damage.
In rats both of the methods were shown beneficial against I/R for intestine by laparotomy. For laparoscopy, only preconditioning has been shown beneficial, and there are no data for postconditioning. 26
In some studies evidence of preconditioning and postconditioning as protection against I/R injury in intestine remains contoversial and shows only minimal benefits. 27 In our study MDA was not decreased enough in both groups 2 and 3 when compared with group 1. According to SOD, GPX, and CAT, there was not any difference between groups 1 and 2. Interestingly, eventhough SOD, GPX, and CAT has increased 2 to 3 folds and significantly in group 3, MDA was not decreased enough. Perhaps, if I/R period has been longer, favorable effects on MDA would be seen.
Our results supported the finding that ischemic preconditioning and postconditioning did not attenuate intestinal injury after laparoscopy-induced I/R, as does pentoxifylline, zinc, and N-acetylcysteine.
Both preconditioning and postconditioning were beneficial for reducing injury in study groups compared with control, but there was no statistically significant difference between groups. This result may be attributable to incomplete ischemia or an insufficient period at laparoscopy that inhibited the occurence of complete beneficial effects of preconditioning and postconditioning.
Another method that we used to reduce the level of oxidative stress and postoperative damage to intestine was pharmacological pretreatment for tissue protection 28 using pentoxifylline, N-acetylcysteine (NAC), and zinc.
Pentoxifylline, a methylxanthine derivative used for its hemorheological properties, has proved to be a potent inhibitor of tumor necrosis factor production. 28 Recent reports suggest that pentoxifylline can enhance the chemotactic response of neutrophils and may inhibit phagocytosis and superoxide production by neutrophils and monocytes. 29 These laboratory findings have been translated into clinical benefits in attenuating I/R injury in patients with intestine, lung, and kidney damage. 30 To date, pentoxifylline has been shown to increase survival rate and preserve intestine function after I/R injury in a rat model. In this study, pentoxifylline has increased MDA levels but has not affected SOD, GPX, and and CAT levels compared with the I/R group 1. The reason for failing increase in SOD and CAT levels sufficiently according to I/R group may be the antioxidant property of itself or the insufficient I/R period to stimulate the antioxidant levels.
NAC, a precursor of glutathione, has been used effectively to replenish intracellular glutathione stores in I/R conditions and can directly scavenge radicals.31,32 In addition, it has antiinflammatory effects.31,32 Although many have investigated the preventive effect of NAC against intestine I/R injury, 32 its benefits in humans have not yet been shown. In this study, NAC decreased the MDA levels and increased CAT levels compared with group 1 but has not changed SOD and GPX levels. The reason for failing increase in SOD and GPX levels sufficiently according to I/R group may be the antioxidant property of itself. Also NAC was the group that decreased the MDA levels most, although it was not significant. NAC effectively attenuated the increase in MDA levels caused by laparoscopy-related pneumoperitoneum.
Zinc has antiinflammatory properties, and in cell culture and animal models, it acts as an antioxidant. These antioxidant properties arise from two mechanisms: (1) via reduction of redox-active metals, and (2) induction of the antioxidant protein, metallothionein, which can scavenge hydroxyl radicals. 33 Other investigators claim that zinc exerts protective effects on tissue through other mechanisms, including DNA binding or inhibition of calcium influx. 33 In this study, group 4 had significantly lower levels of MDA and no difference in SOD, GPX, and CAT levels compared with group 1, supporting evidence of its role in the reduction of I/R injury caused by laparoscopy-related pneumoperitoneum. The reason for failing increase in SOD, GPX, and CAT levels sufficiently according to I/R group may be the antioxidant property of itself or the insufficient I/R period.
Conclusions
Laparoscopy with pneumoperitoneum at 15 mmHg causes increased oxidative stress in small intestine tissue. Zinc, pentoxifylline, and N-acetylcysteine conditioning significantly reduced markers of oxidative stress caused by laparoscopy in this animal model.
Footnotes
Acknowledgment
The authors would like to thank Associate Professor Ali Çetinkaya for his contributions to statistical analysis and figure design.
Disclosure Statement
No competing financial interests exist.