
Abstract
Abstract
Introduction:
Alvimopan coupled with an enhanced recovery protocol (ERP) has been shown to reduce length of stay (LOS) after open colectomy, but its role after laparoscopy remains unknown. This study evaluated alvimopan with an established ERP for laparoscopic (LAP), hand-assisted laparoscopic (HAL), and open colectomy.
Materials and Methods:
Consecutive patients who underwent elective colectomy by any technique were retrospectively identified. Patients were excluded if they developed a major intra-abdominal complication, medical complication, or had a complex preoperative evaluation. Patients were stratified into 4 groups based on the surgical approach (open/HAL vs. LAP) and the use of alvimopan. All patients were managed by using an ERP. The incidence of postoperative ileus (POI) and LOS were compared between alvimopan and control groups for each surgical approach.
Results:
There were 282 patients. Demographics were similar across the 4 groups. The mean number of alvimopan doses administered was 6.7±2.6. For patients in the open/HAL group (n=149), the incidence of primary ileus was 9.5% (7/74) and 16% (12/75) for alvimopan and control patients, respectively (P=.231). A significant decrease in LOS was noted with alvimopan (5.6±2.5 vs. 6.8±3.3 days, P=.009). For patients after LAP (n=133), there was no significance difference in POI with or without alvimopan (3.9% [3/76] vs. 3.5% [2/57], P=1.00). There was no difference in LOS (3.9±1 vs. 3.7±1.4 days, P=.305).
Conclusion:
The addition of alvimopan to an established ERP will lead to improvement in clinical outcomes in patients after open/HAL colectomy. The benefit of alvimopan after LAP remains negligible.
Introduction
Several methods have been suggested to decrease the incidence of POI. Although these techniques have shown some benefit, none have been completely successful in preventing POI. For example, laparoscopic surgery has demonstrated an improvement in the duration of POI and LOS but one large study reported an incidence of 15.4%. 5 Thoracic epidural analgesia can shorten the duration of POI, but its impact on LOS is inconsistent. 6 Enhanced recovery protocols (ERPs) that utilize a multimodal approach (e.g., early removal of nasogastric tubes, restriction of IV fluids, early initiation of oral intake and ambulation, etc.) have been associated with earlier gastrointestinal recovery with reduced LOS and have become the preferred postoperative treatment modality. 7 Nevertheless, POI remains a major clinical and economic burden to the healthcare system.
Alvimopan is a peripherally acting mu-opioid receptor antagonist, which when coupled with an ERP has demonstrated a decreased incidence of POI and a reduction in LOS.8–12 In fact, one pooled analysis of randomized controlled trials in patients undergoing laparotomy revealed a significant reduction in POI (8% vs. 13.9%, P=.007) with an absolute difference in LOS of ∼18 hours when alvimopan was administered (P<.001). 13
The role of alvimopan in laparoscopic (LAP) surgery, however, remains unknown. Since opioid analgesic requirements and LOS tend to be lower than in open procedures, the benefit of alvimopan is questionable. Therefore, we sought to evaluate the impact of adding alvimopan to an established ERP for patients who underwent LAP, hand-assisted LAP surgery (HALS), and open colectomy.
Materials and Methods
Institutional Review Board approval was obtained before study initiation. Adult patients who had undergone elective (i.e., nonemergent) colorectal surgery by a board-certified colorectal surgeon by using any technique were retrospectively identified over an 11 month period. Patients were excluded if they were not managed by using an ERP, developed a major intra-abdominal complication (e.g., anastomotic leak, intra-abdominal abscess, etc.), a major medical complication (e.g., postoperative pneumonia, deep vein thrombosis, etc.), or had a complex work-up before surgery. The ERP utilized has been published elsewhere and consists of removal of the nasogastric tube in the operating room, analgesia via patient-controlled analgesia (IV hydromorphone is preferred) for 12–18 hours postoperatively with subsequent conversion to oral analgesics, early ambulation (as soon as possible after the procedure with a minimum of five walks outside the room on the first postoperative day), full liquids as the first meal after surgery with advancement ad libitum, and no specific restrictions. 14 Antiemetics (ondansetron or prochlorperazine) were administered as needed according to the operating surgeon. The decision to use alvimopan was at the discretion of the attending surgeon according to their usual practice. When utilized, alvimopan (12 mg) was administered 30 minutes–5 hours before surgery and then twice daily beginning on the postoperative day 1 (for a total of 15 doses or 7 days maximum). The ERP has been operationalized by using a preprinted order form that is used for all patients who have undergone colectomy.
Patients meeting inclusion/exclusion criteria were stratified into 4 groups based on the surgical approach (open/HALS and LAP) and the use of alvimopan. HALS and open patients were grouped together, as continuous quality improvement data at our institution has demonstrated a similar rate of POI and LOS for these two techniques. Classification and regression tree analysis was conducted to validate the appropriateness of this approach. Additionally, a subgroup analysis was performed to evaluate each surgical approach separately.
The primary outcome variables were the incidence of POI and hospital LOS. POI was defined as three episodes of vomiting over 24 hours, cessation of oral diet, or the need for an NG tube within 5 days of surgery. Criteria for hospital discharge were the tolerance of three general meals without nausea or vomiting, absence of abdominal distention, adequate oral analgesia, and passage of flatus. A secondary analysis was conducted that adjusted the incidence of POI and LOS to include 30-day readmission caused by delayed ileus and the respective increase in LOS. The incidence of POI and hospital LOS was compared between alvimopan and control groups for each surgical approach (open/HALS, LAP).
A sample size calculation was conducted which revealed that 63 patients would be needed in each group to detect a 1 day difference in LOS with 80% power, alpha=0.05. Pair-wise comparisons for continuous data were analyzed by using Student's t-test (if normally distributed) or Mann Whitney U if not. Dichotomous data were analyzed by using Pearson's Chi square or Fisher's exact test as appropriate. A P value of <.05 was used to determine statistical significance. All statistical analyses were performed with SPSS version 13.0 (Chicago, IL).
Results
There were 308 patients identified, of which 282 met inclusion/exclusion criteria and were included in the final analysis (Fig. 1). Demographics are displayed in Table 1. The mean number of alvimopan doses administered was 6.7±2.6. There were fewer doses administered in the LAP group (7.6±2.8 vs. 5.9±2, P<.001).
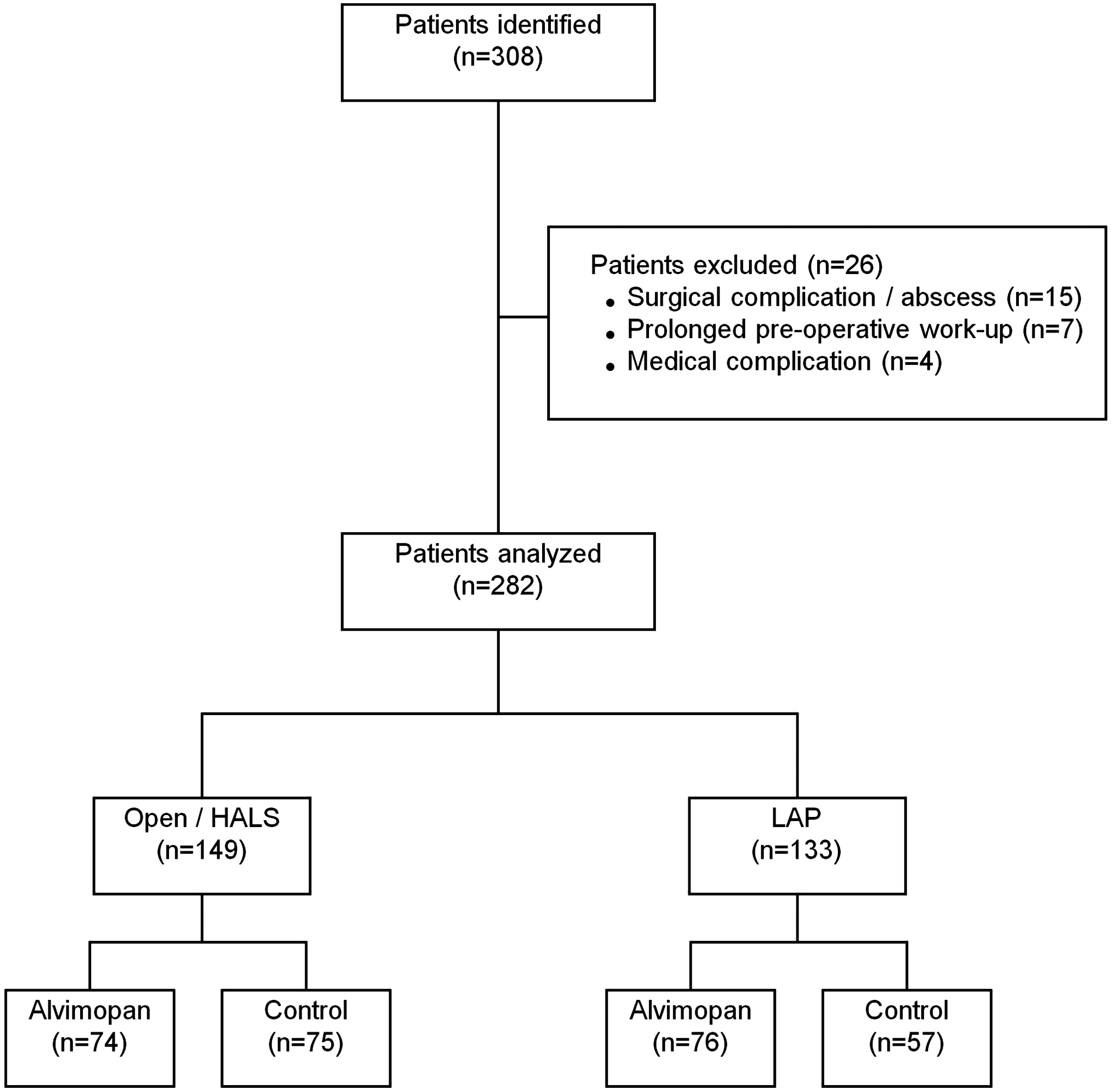
Patient selection. HALS, hand-assisted laparoscopic surgery; LAP, laparoscopic.
HALS, hand-assisted laparoscopic surgery; LAP, laparoscopic; IBD, inflammatory bowel disease.
For patients in the open/HALS group, the incidence of primary POI was 9.5% (7/74) and 16% (12/75) for alvimopan and control patients, respectively (P=.231). A significant decrease in LOS was noted with alvimopan (5.6±2.5 vs. 6.8±3.3 days, P=.009). When readmission data (caused by delayed POI) were included, the incidence of POI (both primary and delayed) was 10.8% (8/74) and 16% (12/75) for alvimopan and control groups, respectively (P=.353). This corresponded to a total LOS of 5.7±2.6 days in the alvimopan group and 6.8±3.3 days in the control group (P=.018).
For patients in the LAP group, the incidence of POI was 3.9% (3/76) and 3.5% (2/57) for alvimopan and control patients, respectively (P=1.00). There was no difference detected in LOS (3.9±1 vs. 3.7±1.4 days, P=.305). When both primary and delayed POI were considered, the incidence of POI was 6.6% and 3.5% for alvimopan and control groups, respectively (P=.698). There was no difference in LOS (4.1±1.5 [alvimopan] vs. 3.7±1.4 days [control], P=.128).
Overall, POI was more commonly observed with open/HALS versus LAP (12.8% [19/149] vs. 3.8% [5/133], P=.007). Further, POI was associated with an increase in LOS by 5.3 days in the open/HALS group (10.8±4.6 vs. 5.5±1.9, P<.001) and 2.4 days in the LAP group (6.2±2.4 vs. 3.8±1, P=.083). In patients who had POI (n=24), LOS was 8.6±4.2 days when alvimopan was used (n=10) and 10.8±4.8 days when it was not (n=14), P=.262. All but 1 patient (LAP/control) survived hospital discharge.
When each surgical approach was separately taken, the incidence of POI was 15.6% (19/122), 0% (0/27), and 3.8% (5/133) in the open, HALS, and LAP group, respectively (P=.001). In addition, LOS was 6.4±3.1, 5.3±1.8, and 3.8±1.2 days for the open, HALS, and LAP groups, respectively (P<.001). When the effect of alvimopan was evaluated, there was no difference in the incidence of POI, but a shorter LOS was noted with alvimopan in the open and HALS groups accordingly (Table 2).
Discussion
POI continues to be a significant clinical burden despite recent efforts aimed at reducing its occurrence. Several advances have been made in reducing the incidence of POI, particularly the use of multimodal ERP. ERPs consist of early removal of nasogastric tubes, early administration of nutrition, ambulation, and limited use of systemic narcotics. One systematic review reported a significance decrease in primary LOS (weighted mean difference=−1.56 [−2.61 to 10.50]) with ERP. 15 This difference was largely due to the prevention or reduction of POI. Along with ERP, laparoscopic surgery can lead to a significant benefit in the incidence of POI. In one review of a large national database (n=32,733), the incidence of POI was 15.4% after laparoscopic colectomy compared with 17.6% with an open procedure (P<.05). 5 This is similar to a recent meta-analysis whereby laparoscopic surgery was associated with significantly less POI than open surgery (odds ratio=0.39 [0.21–0.72], P=.003). 16
Few studies have evaluated the combined approach of ERP with laparoscopic surgery. In one study of 60 patients, no improvement was noted in gastrointestinal function or LOS when laparoscopy was added to an established ERP. 17 A second study of 58 patients reported a reduction in LOS with laparoscopic surgery (7.4 [6–9.2] vs. 5.2 [4.2–6.5] days, P=.018). 18 The incidence of POI, however, was not reported.
The addition of alvimopan to an ERP is an attractive option to reduce the incidence of POI given its complex pathophysiology and the influence of opioid narcotics. In a pooled analysis of phase-III randomized controlled trials with alvimopan, a difference in LOS of 18 hours was reported. 13 In our study, the incidence of POI was reduced by 40%, and a significant reduction (by ∼1 day) in LOS was detected in patients after either an open or HALS procedure. Although the reduction in POI did not reach statistical significance (thus, the observed outcomes could be due to chance), the clinical significance should not be underestimated. We noted an increase in LOS by 5.3 days when POI occurred compared with when it did not. This is similar to a recent analysis that reported an added 4.9 days with primary POI. 4 These data would indicate that even a small reduction in the incidence of POI can lead to a tremendous impact on hospital LOS and the overall burden to the healthcare system. We did not include patients who had extended LOS due to reasons such as surgical complications (e.g., anastomotic leaks, abscess, etc.), complex medical conditions (e.g., venous thromboembolism, advanced neurologic disease, etc.), or prolonged presurgical workups to better assess the relationship between POI, LOS, and potential benefit with alvimopan. This was done to reduce the influence of confounding variables (both pre and postoperatively) and avoid inflation of these outcomes caused by factors that are not affected by alvimopan (venous thromboembolism, pneumonia, etc.). It is important to note that these results did not change when readmissions caused by delayed POI were considered.
In contrast to the results obtained in patients after open or HALS procedures, alvimopan was not associated with the same improvements in patients after laparoscopic surgery. The role of alvimopan in laparoscopic surgery has been questioned given its mechanism of action and the fact that laparoscopic surgery is typically associated with shorter recovery times and lower narcotic use. 19 We were unable to demonstrate a benefit with alvimopan on POI incidence or LOS in this population. Given the lower incidence of POI, however, along with the shorter duration of hospital stay (compared with open/HALS), larger sample sizes may be required. Based on our results, we suggest a process of dosing all patients preoperatively, however, only continuing the medication postoperatively in HALS, open, or LAP converted to open cases.
Although the acquisition of cost for alvimopan is high, the high cost associated with POI can lead to significant cost savings if its incidence can be reduced. Interestingly, the costs associated with primary POI are similar to those encountered with severe postoperative surgical complications (e.g., anastomotic leak, intra-abdominal abscess, etc). 4 In a post-hoc analysis of previously conducted randomized controlled trials, alvimopan was associated with a potential savings of $879–$977 per patient. Of note, the mean number of alvimopan doses administered was 8.9. In our study, a total of 6.7 doses were administered during the hospital stay. This is substantially lower than what might be expected when estimating drug utilization and direct costs, as the maximum allowable doses per course of therapy is 15. In fact, using the wholesale acquisition cost of $62.50 for each 12 mg capsule, the added drug costs per patient are $437.50 (compared with $937.50 with 15 doses). This should be considered when assumptions are made for pharmacoeconomic analyses evaluating the cost effectiveness of alvimopan.
Limitations to this trial include its retrospective nature and the potential for selection bias with regard to who did and did not receive alvimopan. In addition, there could have been other factors which may have influenced LOS that was not related to POI. Although we did exclude patients with significant confounding variables for LOS that could not be explained by POI (e.g., surgical complications, major medical complications, prolonged preoperative work-up, etc.), other reasons not recognized by these investigators may have existed.
In conclusion, the addition of alvimopan to an established ERP will lead to improvement in clinical outcomes but only in patients who undergo open/HALS procedures. Clinicians should consider administering a preoperative dose to all patients who undergo colectomy (by any technique) but only continuing postoperative therapy in patients with open/HALS procedures or in patients after LAP who convert to an open approach. Future trials are needed to assess the cost effectiveness of this approach.
Footnotes
Disclosure Statement
Dr. Senagore is on the advisory board and is a consultant for Adolor Corporation.