
Abstract
Abstract
The presence of retroperitoneal, mediastinal, and subcutaneous emphysema due to rectal diverticular perforation during diagnostic colonoscopy has not been reported. Further, the management of colonoscopic perforation remains a controversial issue. In this case report, the authors discuss the importance of recognizing this rare complication after colonoscopy and its response to conservative treatment.
Introduction
Case Report
An 82-year-old woman presented with retroperitoneal, mediastinal, and subcutaneous emphysema after diagnostic colonoscopy. She was admitted with a complaint of neck swelling and pain in the lower abdomen and both flanks. Forty-eight hours earlier, the patient had undergone colonoscopy at a private hospital. She was told that there was nothing abnormal except for rectal diverticula and was promptly discharged. However, immediately afterward, she suffered from lower abdominal pain, and the next day from mild neck swelling. During that time, she continued to eat small amount and defecated loose stools three times. Her medical history was unremarkable save hypertension and an appendectomy 40 years ago. A physical examination revealed subcutaneous emphysema of the neck and anterior thoracic wall. Her heart rate was 90/minute, blood pressure 120 over 80, and body temperature 37.6°C. On abdominal examination, tenderness of the lower abdomen and both flank areas was noticed. Her total leukocyte count was 13.2×109 cells/L, C-reactive protein 284, and erythrocyte sediment rate 110. Plain radiography and an abdominal computed tomography revealed pneumoretroperitoneum, pneumomediastinum, and cervical emphysema (Figs. 1–3). A wall defect around rectum was suspected. A photograph taken during colonoscopy performed at the private hospital showed perirectal adipose tissue around rectal diverticulum (Fig. 4).
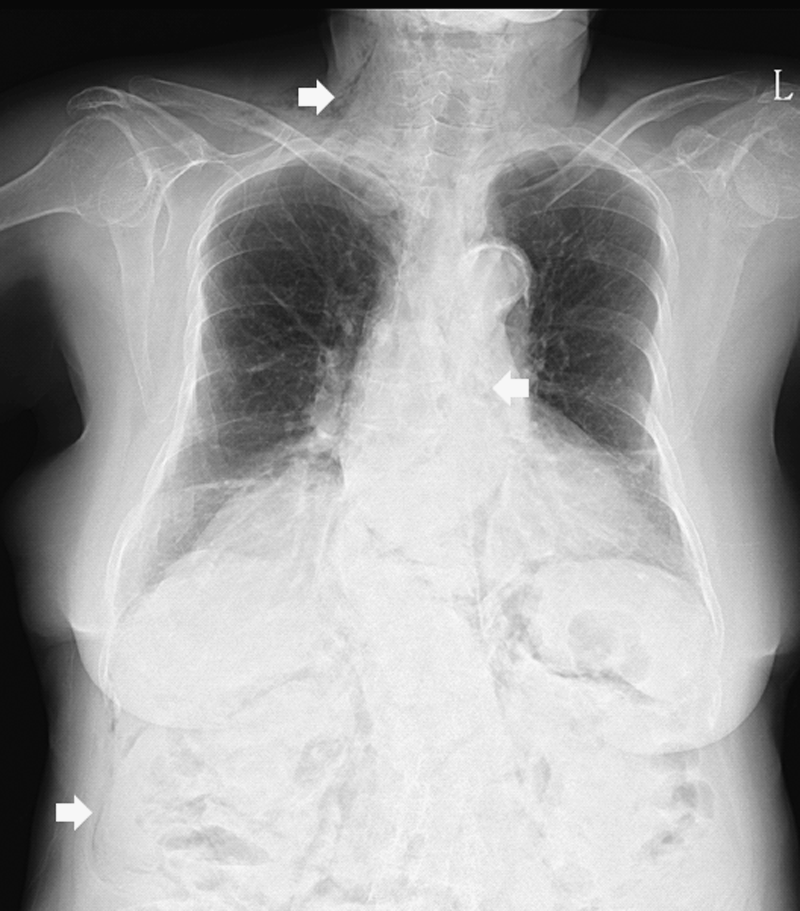
Chest radiograph showing neck emphysema, pneumomediastinum, and pneumoretroperitoneum.

Abdominal radiograph showing retroperitoneal air sharply outlining the kidneys and lateral psoas muscle margin.

Abdominal computed tomography scan showing air bubbles around the rectum.
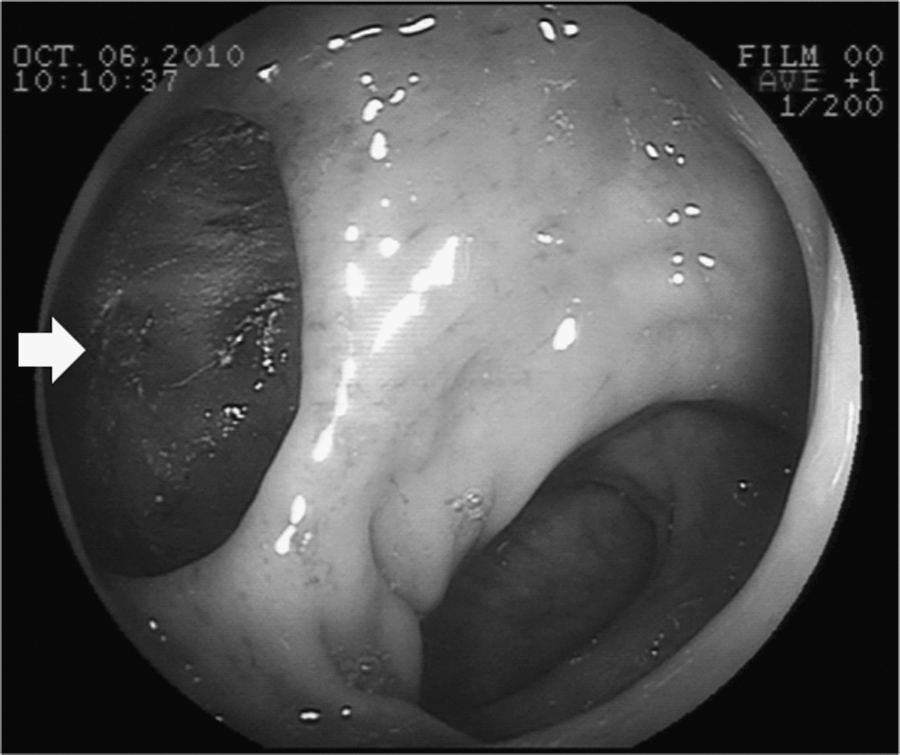
Photograph taken during colonoscopy showing adipose tissue outside a rectal diverticulum.
An extraperitoneal rectal perforation accompanying localized peritonitis was diagnosed, and we decided on conservative treatment with intravenous antibiotics and restriction of oral intake and intravenous fluids. The lower abdominal pain and flank pains gradually improved, and the localized lower abdominal tenderness disappeared 10 days after treatment. An abdominal computed tomography taken on day 11 showed that the retroperitoneal air and perirectal infiltration had almost resolved (Fig. 5). Oral diet was permitted on day 14, and the patient was discharged on day 18.

Abdominal computed tomography scan showing nearly disappeared perirectal, retroperitoneal, and mediastinal air.
Discussion
Colonoscopic perforation (CP) is a rare complication, but given the increasing numbers of procedures performed, its incidence can be expected to increase. Currently, the incidence of perforation attributable to diagnostic colonoscopy ranges between 0.03% and 0.8%, whereas its incidence after therapeutic colonoscopy ranges from 0.15% to 3%.1–3 The majority of CPs occur during therapeutic interventions such as biopsy and polypectomy. Further, CP after therapeutic colonoscopy tends to be smaller than CP after diagnostic colonoscopy, and its presentation and diagnosis are often delayed.2,4 From the diagnostic perspective, perforations are usually the result of undue pressure on the colonic wall and can be visualized immediately by an endoscopist as extra-intestinal tissue. In terms of therapeutic procedures, ischemia of the colonic wall caused by electrical or thermal injury after electrocoagulation or laser treatment can cause delayed perforation. In a review of 30,366 colonoscopies, Luning et al. found an average of 0.36 days elapsed before the diagnosis of perforation diagnosis after a diagnostic procedure, compared with 1.5 days after a therapeutic procedure. 2
The risk factors of CP include old age, the presence of multiple comorbidities, a history of diverticular disease or previous intra-abdominal surgery, colonic obstruction as an indication for colonoscopy, and female gender.4–6 Accordingly, in patients at risk, careful colonoscopy is mandatory.
The most common clinical feature of CP is the visualization of an extra-intestinal structure during an endoscopic examination. 2 In the described case, a picture taken during colonoscopy at the local hospital showed perirectal adipose tissue around a rectal diverticulum, and thus, we consider that the endoscopist might have missed the perforation, which was in the rectal diverticulum. Clinical signs and symptoms of bowel perforation after colonoscopy vary considerably and depend on size, site, amount of contamination, underlying pathology, the mechanism of perforation, and general patient condition. The most consistent symptom is abdominal pain, and the most frequent sign is tachycardia, followed by guarding and rebound tenderness, abdominal distention, leukocytosis, fever, and hypotension. Symptoms can immediately occur or be delayed for up to 72 hours after colonoscopy,1,4,7 and a small proportion of patients remain asymptomatic. 3
Retroperitoneal perforations can be clinically occult, or they may present with unusual symptoms such as hoarseness, a stabbing chest pain, dyspnea, or subcutaneous emphysema.5,8–11 Further, the propagation of gas in the retroperitoneal space (pneumoretroperitoneum) makes possible its further spread not only along muscles, fascia, blood vessels, and nerves to subcutaneous tissue (subcutaneous emphysema), but also to the retropleural space to the mediastinum (pneumomediastinum) and pleural cavity, which could be followed by the development of pneumothorax.5,11 However, these types of presentation are rare; only sporadic cases have been reported, and retroperitoneal, mediastinal, and subcutaneous emphysema due to rectal diverticular perforation during diagnostic colonoscopy has been not previously reported.
Diverticular disease occurs in the colon with great frequency. However, rectal involvement is rare and has been estimated to occur in <0.1% of cases.12,13 Most patients with rectal diverticula are incidentally diagnosed and are asymptomatic, and uncomplicated rectal diverticula are clinically insignificant, whereas the complications associated with rectal diverticula include perforation, abscess formation, a prolapsed rectum, rectal stenosis, and rectal-vesical fistula.13–15 Surgical treatments of complicated rectal diverticula include abscess drainage, diverting colostomy, resection of the diverticular mass, or abdominal perineal resection of the rectum.
The management of CP remains controversial, because it can be effectively managed both operatively and conservatively. Although most patients with CP require prompt surgery, increasingly, nonoperative approaches are used in selected patients. Naturally, the decision as to whether to choose the conservative or surgical route depends on clinical considerations. However, no definite guideline has been issued for the conservative treatment for CP, although several authors have suggested that conservative management can be used in cases with good bowel preparation, in cases resulting from therapeutic colonoscopy, and in cases with few comorbidities, in good general condition, with a retroperitoneal perforation, and a diagnosis within 24 hours of perforation.1–5,9 The conservative approach requires restriction of oral intake, intravenous fluids, and intravenous broad-spectrum antibiotics. If management is successful, clinical criteria should gradually improve within 24–48 hours, but if no clinical improvement is seen or if progressive intra-abdominal sepsis develops, prompt surgery is mandatory.1,3
In the reported patient, rectal diverticular perforation had not been recognized during diagnostic colonoscopy, and the treatment delay was around 48 hours. Further, localized tenderness and mild fever were present at admission. However, the patient was well prepared for colonoscopy, was without severe comorbidities, and responded well after treatment initiation, which all indicated a favorable outcome.
Conclusions
In the absence of generalized peritonitis, retroperitoneal perforations of a rectal diverticulum in a well-prepared bowel can be effectively managed using a conservative approach.
Footnotes
Disclosure Statement
No competing financial interests exist.