
Abstract
Abstract
Introduction:
Although laparoscopy has now become the procedure of choice for removal of gallbladder, complications especially injury to cystic artery and ducts are thought to be higher. We describe a technique that avoids handling and injury of cystic artery and resultant duct injuries. The video length is 2 minutes 13 seconds.
Materials and Methods:
From October 7, 2005, to December 31, 2010, 17 patients were successfully operated by the cystic artery sparing technique. In this technique, dissection begins distal to cystic lymph node on the gallbladder wall using hook cautery, thereby clears the Calot's triangle without even touching the cystic artery. This maneuver eliminates the risk of injuring thus causing bleeding and any subsequent complications. Age, sex, and operative outcomes including follow-ups were evaluated.
Results:
Age of the patients ranged from 3.4 years to 16 years with an average of 10.12 years. Males were predominant (10:7). Average operative time was 40 minutes. There were no intraoperative or immediate postoperative complications. Patients were allowed feeding 4–6 hours after operation and discharged the following morning. Patients were asked to come for follow-up at 1 week, 1 month, 3 months, 6 months, and 1 year and thereafter yearly. Follow-up period ranged from 6 months to 5 years. There were no operation-related complications other than minor abdominal pain in 3 patients and port-site pain in 2 patients which resolved on conservative treatments.
Conclusion:
During laparoscopic cholecystectomy, if handling of the main cystic artery is avoided then complications of hemorrhage and bile duct injuries can be minimized.
Introduction
Materials and Methods
From October 7, 2005, to December 31, 2010, 19 laparoscopic cholecystectomies were performed by Hannan and Hoque. In one case, the cystic artery was running parallel to the cystic duct, and in another case, it was on the under surface of the neck of gallbladder. On both these occasions the cystic artery needed clipping and division. In the remaining 17 cases, cystic artery sparing technique was employed and studied retrospectively. Diagnoses in all of our cases were confirmed by Ultrasonogram. We followed a modified French technique in which the surgeon stands in front of low-down suspended legs instead of between the legs. The assistant stands on the left side of the patient. The following four ports were used by the surgeon: supraumbilical port for camera, epigastric port for gallbladder retraction, left hypochondriac, and right iliac fossa ports (Fig. 1). Except the 10-mm camera port, all other three ports are 5 mm. The assistant's left hand holded the camera and right hand holded and pushed the gallbladder fundus upward and laterally with a grasper. The surgeon's left hand used a grasper to pull the Hartman's pouch downward and laterally to expose the Calot's triangle. Dissection began distal to the lymph node using monopolar hook cautery (Fig. 2). All the minor branches of cystic artery along the adjacent border of gallbladder were cauterized. And the lymph node along with the cystic artery beneath and proximal to it was pushed away creating clear a window (Fig. 3). This maneuver clearly defines the cystic duct for clipping (Fig. 4) and there is minimal chance of touching the main cystic artery and hepatic or common bile ducts. Age, sex, and operative outcomes including follow-ups were evaluated.
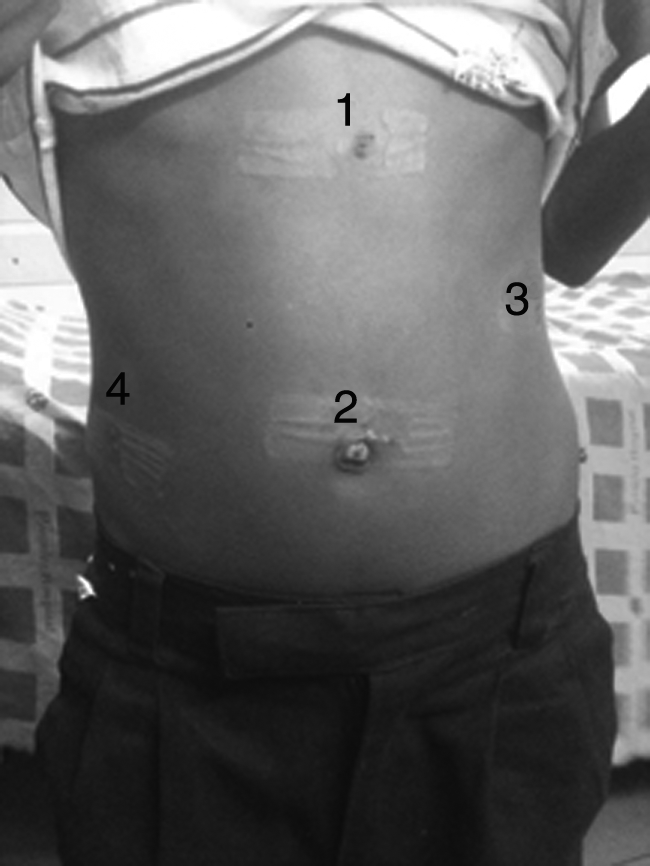
Placement of ports.

Dissection starts distal to lymph node of Lund.
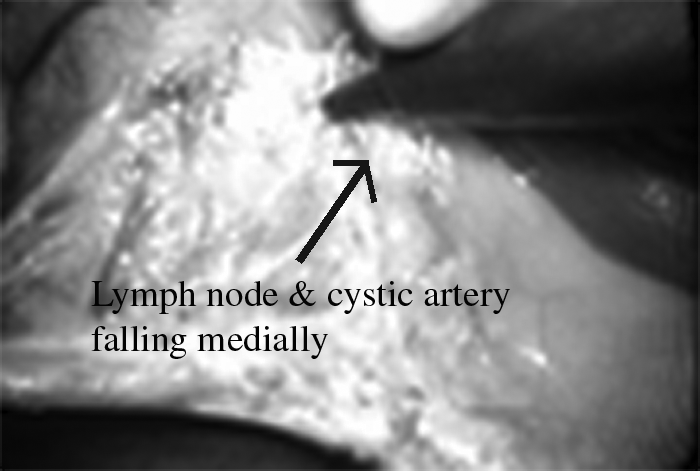
Dissection in progress.

Calot's triangle and cystic duct clearly definable.
Results
Age of the patients ranged from 3.4 years to 16 years with an average of 10.12 years. Males were predominant (10:7) (Table 1). Common complaints that were presented by the patients were right upper quadrant pain, recurrent nonspecific abdominal pain, and dyspepsia (Table 2), and four cases of thalassemia were diagnosed during routine Ultrasonogram (Table 2). Average operative time was 40 minutes. There was no intraoperative or immediate postoperative complication. Feeding was allowed to the patients 4–6 hours after operation and they were discharged the following morning. Patients were asked to come for follow-up at 1 week, 1 month, 3 months, 6 months, and 1 year and thereafter yearly. Follow-up period ranged from 6 months to 5 years. There were no operation-related complications other than minor abdominal pain in 3 patients and port-site pain in 2 patients which resolved on conservative treatments.
Discussion
Bleeding is one of the most alarming complications during laparoscopy and the contributing factors are inadequate exposure, inflammation, adhesions, rough handling, and so on.6,14 To prevent this complication, which may subsequently lead to conversion 15 and injury to bile ducts, dissection in the Calot's triangle must be done very carefully and meticulously. Various methods were described to avoid such complications including “Fundus First” technique16,17 and Triangle of safety technique. 7 In both these methods, dissection begins from above and the cystic artery is handled during the last part of dissection. In some acute cases where we followed “Fundus First” technique, we found that the cystic artery did not need to be handled. So in our subsequent cases we adopted this new approach and succeeded. In this technique not only bleeding from the cystic artery and its resultant complications were avoided, but also cystic duct came into view so early and clearly that any aberration in its anatomy could be detected and handled properly. Further, the bile ducts are kept away from the field of dissection and were protected.
Conclusion
During laparoscopic cholecystectomy, if handling of the main cystic artery is avoided, then complications of hemorrhage and bile duct injuries can be minimized.
Footnotes
Disclosure Statement
No competing financial interests exist.