
Abstract
Abstract
Introduction:
Inguinal herniotomy in children is still dominated by conventional open inguinal herniotomy (COIH) as laparoscopic techniques have yet to demonstrate clear advantages. A technical modification that minimizes the incision of COIH in selected children can offer another minimally invasive alternative. A comparative analysis of safety, efficacy, and parental attitudes between mini-scar inguinal herniotomy (MSIH) and COIH was performed.
Materials and Methods:
All inguinal herniotomy cases performed between January 2008 and April 2010 were reviewed. Patients who were younger than 6 months, presented with complicated hernias, or had an associated hydrocele were excluded. In the MSIH group the final scar length was prospectively measured and then retrospectively compared with a matched group of COIH. Parents in both groups were then interviewed using a standardized questionnaire to inquire about operative outcomes, their satisfaction level, and perception of the incision size.
Results:
Of the 145 patients identified, 113 (79%) had completed the parental phone interview at a mean interval of 275±212 days. Forty (35%) underwent MSIH with a mean final incision length of 7.7±2 mm, and 73 (65%) underwent COIH. The two groups were similar in age, sex, and hernias' sides. Postoperative complication including recurrence rates did not differ between MSIH and COIH (2.5% versus 6.8%, P=.4). However, parents in the MSIH group were more likely to notice that the scar was smaller than what they have expected (odds ratio, 4.9; 95% confidence interval, 2.1–11.9) and were more likely to be very satisfied (odds ratio, 10.8; 95% confidence interval, 3.1–38).
Conclusion:
The safety and efficacy of MSIH are comparable to those of COIH. However, in the MSIH group, parents are more likely to notice the smaller scar, which might improve their satisfaction.
Introduction
Patients and Methods
Between January 2008 and April 2010, 281 children underwent inguinal herniotomy at our hospital. Children younger than 6 months and those presenting with an associated hydrocele or complicated or large inguinoscrotal hernias were excluded. Of 281 patients, 145 (51.6%) met our inclusion criteria; 43 underwent MSIH, and 102 had COIH concurrently. After the necessary Institutional Review Board approval was obtained, the records of both groups were reviewed, and the required data were recorded.
The techniques
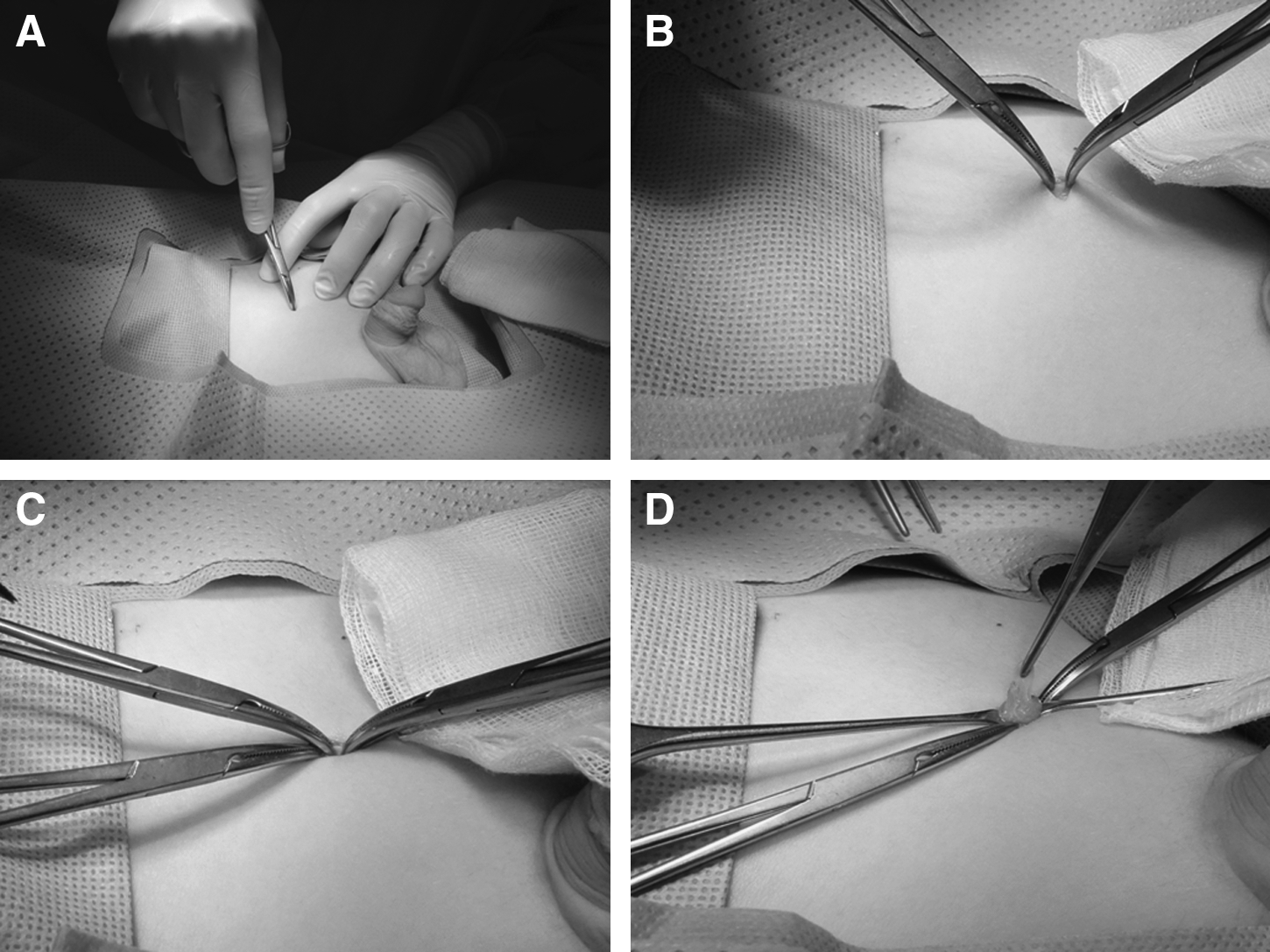
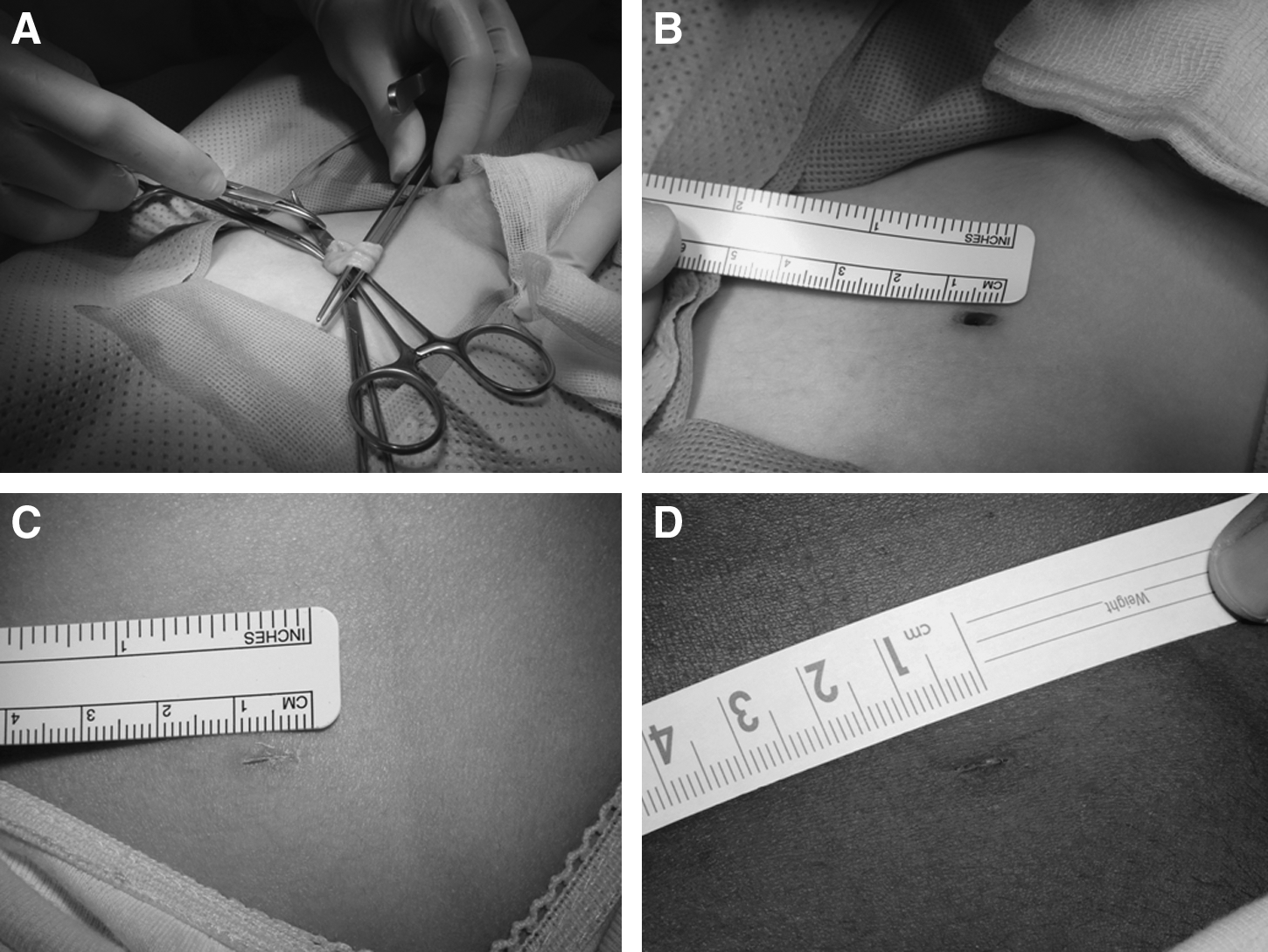
MSIH was performed through a standard 6-mm initial incision placed lateral to the pubic tubercle, just superior to the inguinal ligament. If difficulties were encountered, particularly in the earlier cases, the incision was enlarged in stepwise fashion to an extent that permitted safe completion of the procedure. The final incision was prospectively measured and documented at the end of each procedure. Using fine-tip inverted clamps (Fig. 1A), the subcutaneous fat was spread to gain access to Scarpa's fascia, which was then picked up, identified, and cut between two clamps (Fig. 1B). The same procedure was followed to pick up, identify, and create a small cut in the external oblique (Fig. 1C). Fine-tip DeBakey's forceps was used to grasp the sac or the overlying cremasteric muscle to exteriorize the cord, which was identified as the most inferior structure in the inguinal canal. Once identified, the attached cremasteric fibers were teased away from the sac and pushed back inside the small incision to provide additional space (Fig. 1D). While the forceps was closed, its tip was then passed under the cord's structures from the lateral to the medial sides and then lifted. Successful forceps passage under the cord structures involved repeated attempts of passing and upward lifting movements. Once the cord was completely hooked (Fig. 2A), in males, the sac was isolated from the vas and vessels, followed by high ligation, similar to the COIH technique. Gentle pull on the sac moves the incision laterally aligning it with the internal ring, permitting high ligation at the neck. The external oblique was then closed with a single figure of eight absorbable stitches, while the Scarpa's fascia was left open. After subcuticular incision closure, Steri-Strips were trimmed to the incision length, then applied, and covered with a transparent adhesive dressing. COIH procedures were performed in accordance with previous descriptions.5,9 Because of the retrospective nature of the study the incision was not routinely measured for COIH; however, all operating surgeons agreed that the usual length was significantly longer than that of the MSIH incision. Because of the relative novelty, this initial series of MSIH represented a single surgeon experience, whereas COIH procedures were performed by the other four senior surgeons. All patients were discharged the same day and were given similar postoperative instructions.
Follow-up and parental interview
All patients were scheduled for a routine postoperative follow-up visit 2 weeks after surgery and provided free access to surgical service in case of any postoperative concerns. When postoperative complication was suspected longer follow-up was provided. Using a standardized questioner, parents in the two groups were called and interviewed by phone at variable postoperative intervals. They were asked open-ended questions about any postoperative complications and recurrences, and closed-ended questions were used to measure the parents' perception of the scars length and their overall satisfaction (Table 1).
CI, 95% confidence interval; OR, odds ratio.
Statistical analysis
In our analysis, Fisher's exact and chi-square tests were used to compare categorical variables and estimate risks, and the Mann–Whitney U test was used to compare the continuous variables. Levels of parental satisfaction and their perception about the scar length were converted to continuous variables and then correlated. Similarly, to identify the impact of learning curve, all unilateral MSIH cases were ranked according to their chronological orders, and the resulting variable was then correlated with the duration of surgery and final scar length. Pearson's correlation was used to identify the relationships between these continuous variables. The confidence interval was estimated at 95%, and P values <.05 were considered significant.
Results
Among the 145 identified patients, 48 MSIHs were performed on 43 patients (5 bilateral and 38 unilateral), compared with 107 COIHs performed on 102 patients (5 bilateral and 97 unilateral). Of all the patients, 113 (79%) had parents who successfully completed the interview. The interval between the date of surgery and the phone interview was significantly longer for the COIH group (351±208 days) than for the MSIH group (137±139 days, P<.0001). There was no significant difference between the MSIH and COIH groups with respect to the ratio of boys to girls (27:13 versus 54:19, P=.5), the location of the hernia (right:left:bilateral 16:19:5 versus 40:31:2, P=.07), and the mean age in months (56.2±38.4 versus 60.1±8.3, P=.5).
Operative outcomes
The mean final incision length among MSIH patients was 7.7±2 mm. When only unilateral cases were included, the operative time was significantly shorter for MSIH than for COIH (27.6±9.3 versus 33±13.2 minutes, P<.03). Postoperatively, 1 patient in the MSIH group developed a scrotal hematoma that resolved spontaneously leaving a normal-sized testis at 6-month follow-up. In the COIH group, 3 recurrences were reported, and 2 patients had persistent postoperative pain. However, there was no statistically significant difference in the complication rate between the two groups (P=.09) (Table 1). The chart review and phone interview were consistent in regard to the number and nature of complications.
There was a significant negative correlation between the experience, represented by the chronological order of the unilateral MSIH cases, and the final scar length (r=−.35, P=.038); however, similar correlation could not be demonstrated with the operative time (Table 2).
Experience represents the chronological order of mini-scar inguinal herniotomy cases.
NS, not significant.
Parental attitudes
The interviewed parents of children in the MSIH group were more likely to report that the scar was smaller than what they had expected (77.5% versus 41.1%), with an odds ratio of 4.9 and a 95% confidence interval of 2.1–11.9. They were also more likely to be very satisfied (92.5% versus 53.4%), with an odds ratio of 10.8 and a 95% confidence interval of 3.1–38 (Table 1). Furthermore, a positive relationship was found between the parents' perception of a smaller scar and their higher satisfaction level (r=+.45, P<.0001). Despite the presence of significant difference in the phone interview interval between the MSIH and COIH groups, this difference did not seem to influence the parents' satisfaction level (r=−.125, P=0.095).
Discussion
Despite continuous efforts to introduce laparoscopy by various inguinal herniotomy techniques,10–14 its use is still not seen as a practical alternative to effectively challenge the popularity of COIH. The advantage of leaving multiple 3–5-mm laparoscopic scars may not seem significant by many surgeons, particularly when the cost of the required instruments, the additional skills required, and the increased setup time are considered. In addition, the possibility of higher complication rate such as recurrences and injury to the gonadal vessels,4,10,15 compared with an already established safe and effective procedure, could further deter many surgeons from adopting any of the described laparoscopic techniques. Furthermore, the advantage of routine laparoscopic exploration and repair of patent processus vaginalis at the contralateral side is still debatable and not widely practiced.5,16,17 Our study demonstrates that in selected patients, surgeons can modify the existing open herniotomy technique to be less invasive and leaves a smaller scar, hence sharing the main advantages of laparoscopic hernia repair and avoiding some of its drawbacks.
The safety and efficacy of our technique were comparable to those of COIH; however, leaving a noticeably smaller scar might have led to the reported positive impact on patients' satisfaction, which is an essential element in measuring quality of care.18,19 As we predicted, parents were able to notice that the inguinal scar was smaller than what they had expected preoperatively. It is possible that their preset expectations about the possible scar length were related to the actual hernia size or their experience with previous pediatric and adult hernia repair. It was not surprising that their appreciation of the smaller scar was proportionate to their satisfaction level. Others have similarly demonstrated parents' appreciation of smaller scars associated with laparoscopic procedures. 20
Picking up and exteriorizing the cord through the small incision can be viewed as risky; however, similar to COIH, what is picked is the sac and cremasteric fibers, which are the most superficial components of the cord. A similar step is performed through a smaller incision in selective sac extraction; 21 however, in such a technique the vas and vessels are separated in situ without adequate visualization, which might increase their injury risk. Leaving small clamps attached to the edges of the opened layers facilitates the visualization and dissection of the underlying structure without the need of excessive skin retraction. We found that the procedure was much easier to perform in leaner patients, whereas overweight or obese children might require a slightly larger incision. We also believe that a large part of the procedure success is attributable to the careful exclusion of potentially difficult cases. In these patients, the extensive adhesions and the large sac associated with large incarcerated inguinoscrotal hernias are very difficult to tackle through the tiny incision. In addition to having thinner sacs, children younger than 6 months have tissues that are less differentiated, and therefore it would be difficult to clearly identify the tissues and complete the procedure safely. Similar difficulties in smaller babies have been described by others when using smaller incisions. 21 Because of the inability to effectively evacuate and lay open the distal sac through the small incision, patients with hydroceles were also excluded, similar to what has been reported by some in laparoscopic herniotomy. 22 Despite the wide exclusion criteria, more than 50% of our cases could have benefited from the smaller incision.
As expected, the ability to minimize the scar size in MSIH cases tended to improve with experience. This is demonstrated by the negative correlation between the final scar size and the chronological order of cases. We could not demonstrate similar impact of experience on operative time, probably because the surgeon is less motivated to improve operative time compared with the value of maintaining patients' safety and minimizing the scar size.
Using a single stitch to close the external oblique, leaving Scarpa's fascia open, and only a few millimeters of skin to close could explain the significantly shorter operative time for MSIH. The smaller incision in MSIH could have caused remarkably less postoperative pain, which we have noticed frequently in our children; unfortunately, the retrospective nature of the study rendered pain evaluation difficult and inaccurate. This issue could be better addressed in future prospective studies.
One of the main limitations of this study is the surgeons' distribution, which might introduce bias when evaluating outcomes. However, similar to the situation with other surgical techniques, practicing surgeons tend to resist adopting newly introduced techniques particularly for such commonly performed procedures, which explains our single surgeon experience. Once more findings accumulate more surgeons might feel comfortable in modifying their practice. Moreover, the performing surgeon had the least years in practice, making it less likely that some of the difference in outcomes could be attributed to the surgeons' experience. Finally, although the incision length was prospectively measured in MSIH, it was impossible to retrospectively estimate the length of incision for the COIH group; however, most surgeons would agree that the incision length in COIH is significantly larger than 7.7 mm. Despite that, we still believe that the addition of a matched control or comparative group adds to the validity of our findings, unlike most recently published LIH technical reports that are limited to a single intervention group.4,5,11–15
This comparative analysis demonstrates that in selected patients, MISH is not only effective and safe, but parents frequently appreciated the smaller scar, which might have a positive impact on their overall satisfaction, a major tool in assessing outcomes in children's health care. Furthermore, MSIH can be another minimally invasive alternative to laparoscopic technique, particularly for surgeons who still prefer the popular COIH. However, this is still a preliminary report that has set the groundwork for future prospective randomized trials needed to confirm this conclusion.
Footnotes
Disclosure Statement
No competing financial interests exist.