
Abstract
Abstract
Many surgeons have found it difficult to decide whether to apply percutaneous transhepatic gallbladder drainage (PTGBD) in patients with acute cholecystitis that is not responsive to initial medical management (IMMx), because the indications of PTGBD are ambiguous. The aim of this study was to evaluate the appropriate treatment for acute cholecystitis that is not responsive to IMMx. Specifically, we focused on differences in surgical outcomes between elective and emergency laparoscopic surgeries. Between March 2006 and February 2009, 738 patients with acute cholecystitis who had undergone laparoscopic cholecystectomy (LC) at our institution were retrospectively studied. We divided them into 3 groups. Group I included 494 patients who underwent elective LC without pre-operative PTGBD, group II included 97 patients who intended to undergo elective LC after preoperative PTGBD, and group III included 147 patients who underwent emergency LC without preoperative PTGBD. We compared age, sex, symptom duration, body temperature, leukocyte counts, and American Society of Anesthesiologists (ASA) class on admission as clinical characteristics. We compared the time interval from symptom development and admission to surgery, operative time, the conversion rate to open surgery, postoperative complications, the total length of stay, and the postoperative length of stay as perioperative surgical outcomes. For patients with ASA 2 and 3, the conversion rate to open surgery in group II was significantly less than that in group III (P<.05, P<.01, respectively). We recommend PTGBD as the first choice for acute cholecystitis in patients who show no improvement after IMMx, to allow the patient to undergo an elective LC rather than emergency surgery for patients with ASA 2 and 3.
Introduction
Despite the widespread acceptance of this classic algorithm, many surgeons have performed numerous diverse treatment procedures for patients with acute cholecystitis. 3 One reason for this may be the ambiguous indications for PTGBD in patients with acute cholecystitis in real clinical situations. Many physicians have difficulties in deciding whether or not to perform PTGBD in these patients.
In general, emergency surgery is a predictive risk factor for increased postoperative morbidity and mortality. 4 Giger et al. 5 reported that emergency surgery could be one of the risks for possible perioperative complications after analyzing >20,000 patients who had undergone LC.
The aim of the current study was to evaluate the appropriate treatment for acute cholecystitis that is not responsive to IMMx. Specifically, we focused on the differences in surgical outcomes between elective and emergency laparoscopic surgeries.
Materials and Methods
This study was approved by our Institutional Review Board. During the period from March 2006 to February 2009, 2384 patients underwent LC at Hallym University Medical Center, South Korea. Among them, we excluded those patients who were asymptomatic, and those with chronic cholecystitis, gallbladder polyps or malignancy on permanent pathology, and common bile duct stones. We also excluded patients with other chief complaints or main diseases such as chest pain or cerebrovascular attacks. A total of 738 patients were enrolled in this study and were retrospectively analyzed. Among them, 97 patients (13.2%) underwent PTGBD. Ninety-four of those patients (97%) successfully recovered after PTGBD and underwent elective LC. The remaining 3 patients (3%) underwent emergency LC because of symptom aggravation even after PTGBD. We included these 3 patients in the study. We divided the patients into 3 groups. Group I comprised 494 patients who underwent elective LC without preoperative PTGBD, group II consisted of 97 patients who intended to undergo elective LC after preoperative PTGBD, and group III had 147 patients who underwent emergency LC without preoperative PTGBD.
We defined “acute cholecystitis” as the presence of right upper quadrant abdominal pain (biliary colic) with a duration of >24 hours and a gallstone confirmed using imaging studies, or the presence of right upper quadrant abdominal pain (biliary colic) with a duration of <24 hours and, at least, one other indicator such as a gallbladder wall thickness of >4 mm, pericholecystic fluid collection, an impacted stone, or sonographic Murphy's sign observed using imaging studies. 6
“Improvement for initial medical management” was difficult to define. However, as a potential definition, we suggest that the patient felt the relief of pain after an injection of ordinary analgesics such as non-steroidal anti-inflammatory drugs (NSAIDs) and needed no more analgesics within 4 hours from the previous injection. We also considered the patients as showing no improvement when they showed symptoms and signs of prolonged sepsis or peritonitis during the IMMx. NPO (nothing by mouth), fluid injection, antibiotics, and analgesics composed the IMMx.
“Emergency surgery” was also difficult to define. We suggest an operation performed during the same hospital admission that was unscheduled or performed <12 hours after admission.6,7
We compared age, sex, symptom duration, body temperature, serum leukocyte counts, and American Society of Anesthesiologists (ASA) class on admission as clinical characteristics among the three groups. We compared the time interval from admission to surgery, time interval from symptom development to surgery, operative time, conversion rate to open surgery, postoperative complications, total length of hospital stay, and postoperative length of hospital stay as surgical outcomes among the three groups. We analyzed the correlation of the time to surgery with the operative time, the conversion rate to open surgery, postoperative complication, and the postoperative length of hospital stay in each group.
The statistical analysis was carried out by using SPSS for Windows, version 13.0 (SPSS Inc., Chicago, IL). Independent t test, chi-squared test, and Pearson and Spearman correlation were used. Differences were considered significant at P<.05.
Results
Clinical characteristics on admission
The mean age was 66.4 years in group II, and 55.5 years in group III (P<.01) (Table 1). There were no significant differences in gender or symptom duration between the two groups. The mean body temperature was 37.2°C in group II and 36.9°C in group III (P<.05). The mean leukocyte counts were 15,349/mm3 in group II and 12,645/mm3 in group III (P<.01). There was a greater number of high-risk patients based on ASA class in group II than in group III (P<.01).
ASA, American Society of Anesthesiologist class; group I, elective LC without PTGBD; group II, elective LC after PTGBD; group III, emergency LC without PTGBD; LC, laparoscopic cholecystectomy; PTGBD, percutaneous transhepatic gallbladder drainage; NS, not significant; WBC, white blood cell.
Perioperative surgical outcomes
1. Overall perioperative outcomes in all three groups (Table 2).
2. The mean time interval from admission to surgery was 188.4 hours in group II and 42.4 hours in group III (P<.01). The mean time interval from symptom development to surgery was 239.8 hours in group II, and 106.6 hours in group III (P<.01). The mean operative time was 119.6 minutes in group II, and 104.0 minutes in group III (P<.05). The conversion rate to open surgery was 4.1% (4 cases) in group II, and 15.6% (23 cases) in group III (P<.01). The postoperative complication rate was 3.2% (3 cases) in group II, and 5.6% (8 cases) in group III, but this difference was not statistically significant. There was one death in group III, which was caused by respiratory failure. The mean total length of hospital stay was 14.9 days in group II, and 9.0 days in group III (P<.01). However, the postoperative length of hospital stay was 7.2 days in group II, and 6.5 days in group III, not statistically significant. Correlation analysis of the time interval from admission to surgery in groups II and III revealed no significant correlations with operative time, conversion rate to open surgery, postoperative complications, or postoperative length of hospital stay. In addition, the time interval from symptom development to surgery in groups II and III did not demonstrate a significant correlation with these factors.
3. Overall perioperative outcomes between the same patients with ASA in groups II and III (Tables 3–5). We analyzed groups II and III according to the same ASA class. For patients with ASA 1, the mean leukocyte counts in group II were significantly greater than were those in group III (P<.05), but there were no significant differences in other clinical characteristics between the two groups. The mean operative time in group II was significantly longer than that in group II (P<.05). There were no significant differences in the conversion rate to open surgery, postoperative complication rate, or postoperative hospital stay between the groups (Table 3). For patients with ASA 2, the mean age and leukocyte counts in group II were significantly greater than were those in group III (P<.01, P<.05, respectively), but other clinical characteristics were similar. However, the conversion rate to open surgery in group II was significantly less than that in group III (P<.05). There were no significant differences in the operative time, postoperative complication rate, or postoperative hospital stay between the two groups (Table 4). For patients with ASA 3, no significant differences were observed in clinical characteristics between groups II and III. However, the conversion rate to open surgery in group II was significantly decreased compared with that in group III (P<.01). There were no significant differences in the operative time, postoperative complication rate, or postoperative hospital stay between the two groups (Table 5).
Discussion
Elective surgery is currently more common than emergency surgery. 8 Elective surgery can be performed after a diagnosis based on the medical history and physical examination of the patient, together with sufficient laboratory and radiological test results and the physician's overall planning of disease management. In emergency surgery, the surgeon has less information about the patient than what is routinely required. The surgeon operates on the patient under very time-dependent conditions to rescue the patient's life, to avoid severe damage or systemic deterioration, or to relieve severe pain.
There have been many reports concerning the effect of operation timing on surgical outcomes. Rattner et al. 9 reported that leukocytosis and high alkaline phosphatase levels on admission, as well as the time interval from symptom development to surgery, were significantly correlated with the conversion rate to open surgery. Bender and Zenilman 10 insisted that emergency surgery was preferable in acute cholecystitis. Koo and Thirlby 11 and Pessaux et al. 12 stated that surgery should not be delayed for acute cholecystitis. Madan et al. 13 reported that a group which underwent surgery within 48 hours of symptom development had better surgical outcomes, such as operative time, total length of hospital stay, and postoperative length of hospital stay. Tsushimi et al. 14 insisted that early surgery was necessary in acute gangrenous cholecystitis. In contrast, Knight et al. 15 reported that there was no significant differences in terms of conversion rate to open surgery between groups that underwent surgery within and after 3 days of symptom development. Tzovaras et al. 16 reported that there were no significant differences in the conversion rate to open surgery, morbidity rate, or postoperative length of hospital stay among groups that underwent surgery 3, 4–7, and >7 days after symptom development. Lee et al. 17 reported that the risk factors of conversion to open surgery were acute cholecystitis and a past history of abdominal surgery, and that the time interval from symptom development to surgery was not statistically significant. Farooq et al. 18 insisted that an experienced surgeon could safely perform the operation as much as 72 hours after the development of symptoms.
In the current study, we did not detect any significant correlations among the three groups between the time from admission (or symptom development) to surgery and the multiple factors that characterize perioperative surgical outcomes. We suggest that the optimal time to surgery in group I would be within 72 hours in accordance with the classic algorithm. 2 In group II, the advisable time to surgery would be within 72 hours or within 1 week after PTGBD, to avoid the severe thick inflammation that is commonly observed at 3–4 weeks after the development of symptoms (Fig. 1). Moreover, we suggest that surgeries in group III should be performed as soon as possible, so long as the preoperative preparation has been completed (Fig. 1).
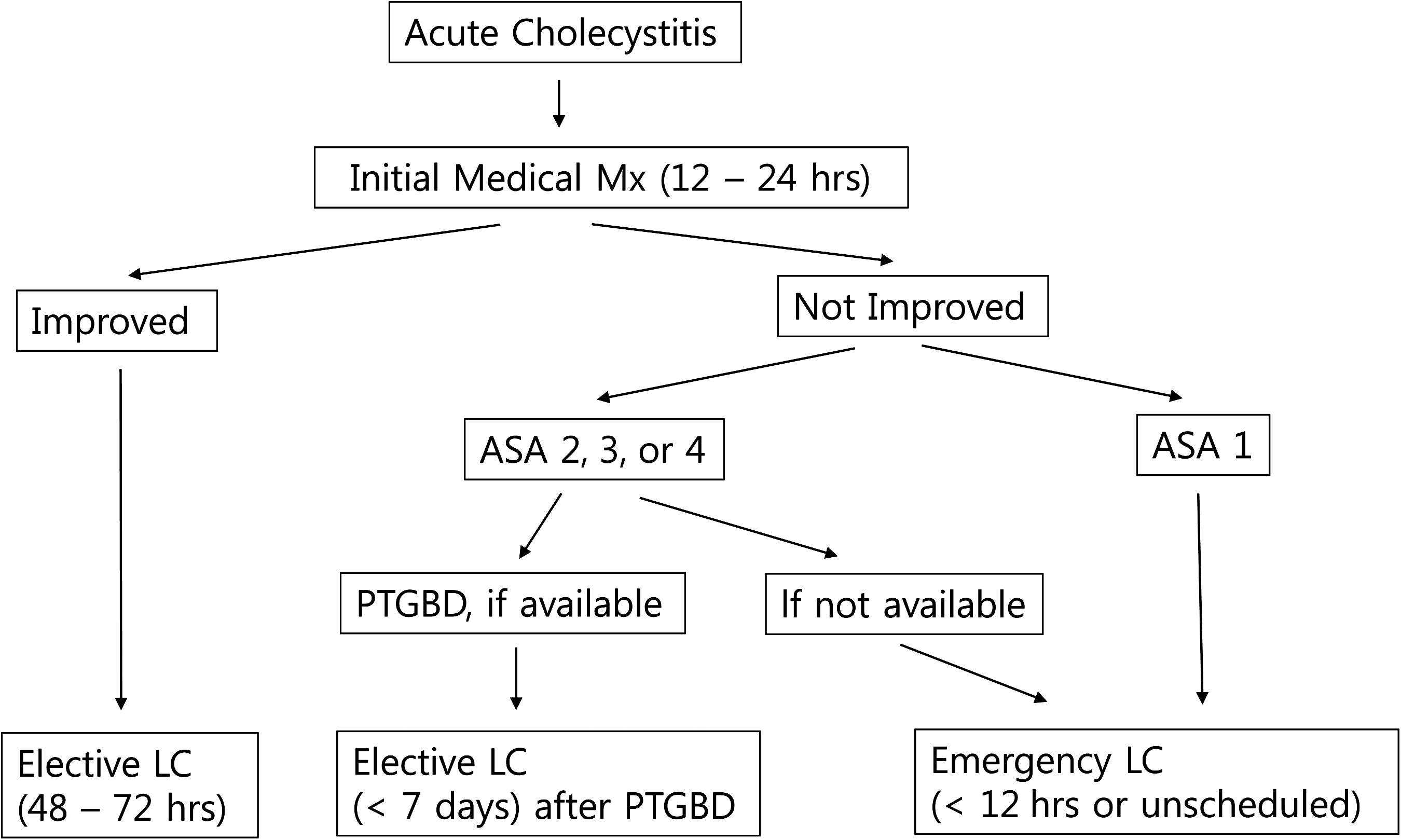
Proposed algorithm for acute cholecystitis. ASA, American Society of Anesthesiologist class; PTGBD, percutaneous transhepatic gallbladder drainage; LC, laparoscopic cholecystectomy.
Regarding the usefulness of PTGBD for patients with acute cholecystitis, Van Steenbergen et al. 1 reported better surgical outcomes of PTGBD in patients with an age of 58–92 years. Avrahami et al. 19 reported that the indications for PTGBD were an ASA class of 4 or 5, debilitated patients regardless of intensive conservative treatment at 48–72 hours after admission, unexplained sepsis, gallbladder distension, and patients with acalculous cholecystitis who require treatment in the intensive care unit. Borzellino et al. 20 reported that it was important to perform PTGBD to reduce the operative mortality rate. However, Kim et al. 21 reported longer operative times in the PTGBD group compared with the group without PTGBD. Tsumura et al. 22 reported no significant differences in surgical outcomes between groups with and without PTGBD. Kim et al. 23 reported that PTGBD could increase conversion rate to open surgery, and that it could not decrease operative time or postoperative length of hospital stay.
In the current study, there were significant differences in characteristics such as the ASA class between groups II and III. This finding is consistent with the classic algorithm showing that high-risk patients undergo PTGBD and that low-risk patients undergo emergency surgery. 2 For ASA 1 of groups II and III, none of the postoperative outcomes excluding the operative time were significantly different between the two groups (Table 3). For ASA 1 in groups II and III, whether emergency surgery or elective surgery after PTGBD is performed may depend on the policy of the individual hospital or the surgeon.
For ASA 2 and 3 in groups II and III, the conversion rate to open surgery in group II was significantly less than that in group III (Tables 4 and 5). For ASA 2 and 3 in groups II and III, we suggest that elective surgery after PTGBD may produce significantly better outcomes on the basis of the current results. The PTGBD enabled a change from emergency surgeries to elective ones. Of course, PTGBD is not available in all hospitals. However, we propose that PTGBD, if available, should be preferentially performed for the patients of ASA 2 or 3 with acute cholecystitis that requires emergency surgery (Fig. 1). We should consider the very time-dependent and, sometimes, terrible conditions faced by the surgeon as just mentioned. Moreover, the stress and anxiety of the patients and their families during emergency surgery should also be considered. We think that elective instead of emergency surgery should be selected for the patients of ASA 2 or 3, if PTGBD is available.
For ASA 4 in groups II and III, unfortunately we did not have enough cases to scientifically analyze (group II had 2 cases, and group III had none of ASA 4) in this study. More patients with ASA 4 (the sickest patients) should be helpful to analyze clinical characteristics. We expect the following report of patients with ASA 4 with acute cholecystitis by ourselves or other authors in the future.
According to such an algorithm, the indication for PTGBD in acute cholecystitis would be “not responsive to initial medical management, when the patient is in a high-risk group of ASA 2 or 3.”
In conclusion, we consider elective LC for the treatment of patients with acute cholecystitis after several days of IMMx with or without PTGBD. We also recommend PTGBD for patients with ASA 2 to 3 with acute cholecystitis who have failed to show improvement after IMMx, to achieve an elective LC rather than an emergency surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.