
Abstract
Abstract
Placement of a ventriculoperitoneal (VP) shunt may increase intraabdominal pressure and lead to an abdominal or genitourinary complication. We report on a 2-month-old boy with complex congenital neurologic and cardiac anomalies who had a VP shunt migrate into the left inguinal hernia. This report demonstrates how a laparoscopic approach can be successfully used to reposition the VP shunt, identify a contralateral inguinal hernia, and repair both without any additional incisions.
Introduction
Case Report
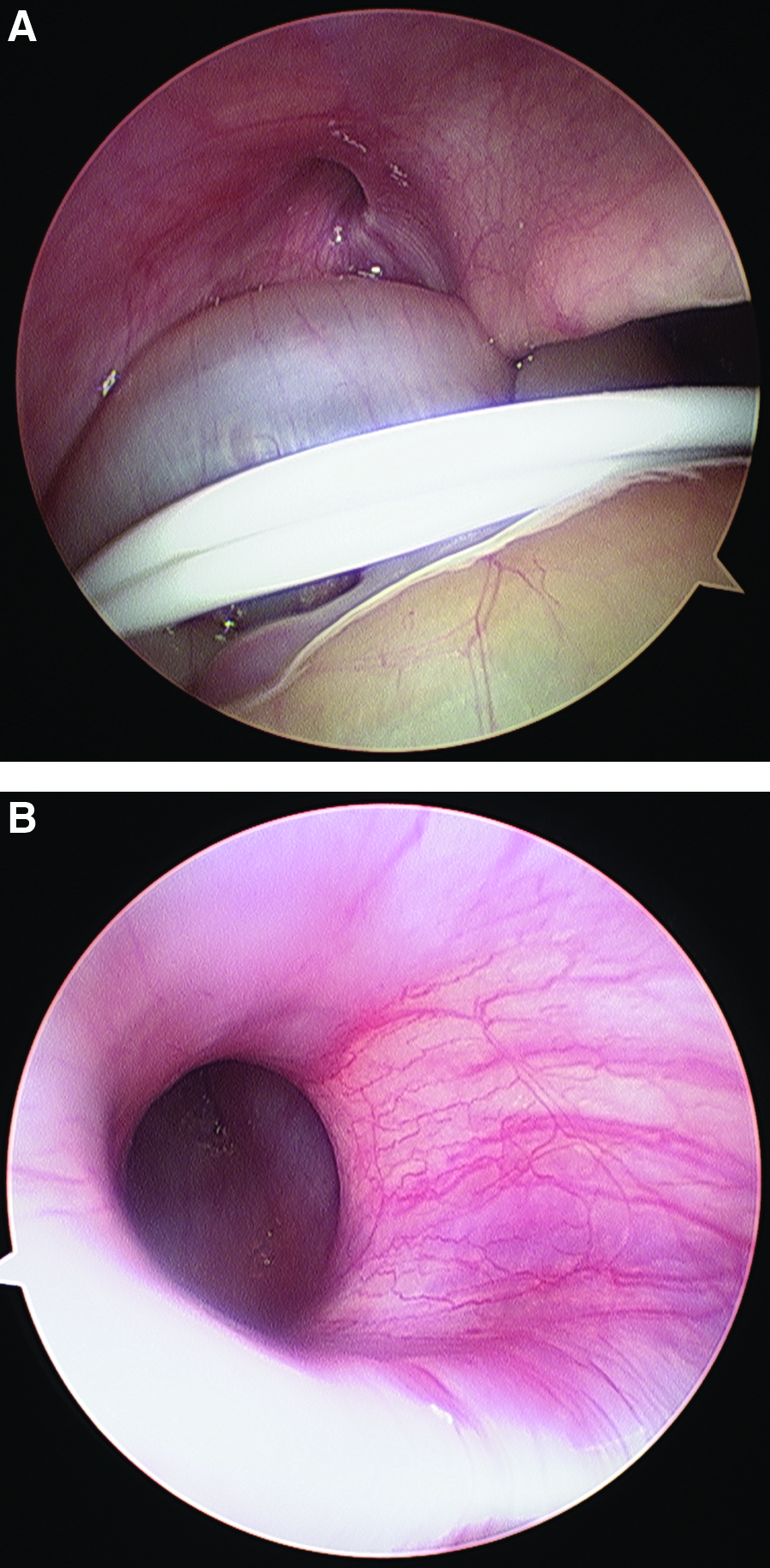
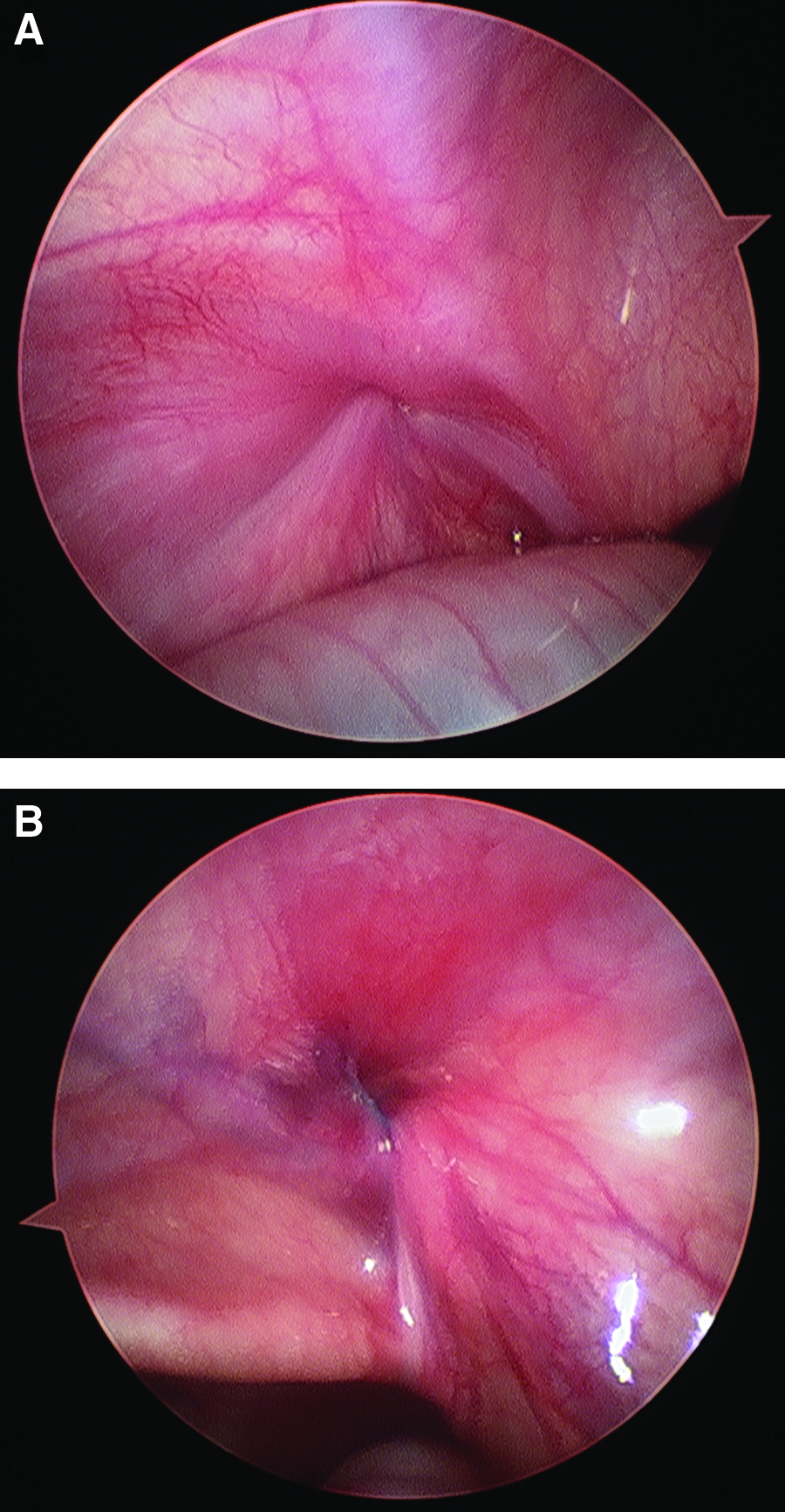
A 2-month-old boy had been born at 38 weeks' gestation with bilateral porencephaly, double-outlet right ventricle with transposition of the great arteries, patent foramen ovale, intrauterine growth retardation, and laryngomalacia. At a follow-up examination by his pediatrician, his head circumference measured greater than the 95th percentile. Additional workup revealed obstructive hydrocephalus secondary to an aqueduct stenosis in the setting of porencephaly for which he underwent placement of a VP shunt. Because of the rapid growth expected of the child, a long peritoneal catheter was left in the abdomen. However, a routine shunt series on postoperative day 1 revealed the distal peritoneal catheter to have migrated into his left scrotal sac (Fig. 1). On physical examination, the peritoneal catheter was palpable within the left inguinal canal and scrotum but was unable to be reduced back into the abdomen (incarcerated). Plans were made for a laparoscopic intervention to reposition the catheter back into the peritoneal cavity, repair the left inguinal hernia, and assess the contralateral side for a patent processus vaginalis (PPV). A transverse umbilical incision allowed the placement of a 3-mm port and a 30-degree laparoscope. The abdomen was insufflated gradually to a pressure of 6 mm Hg in order to minimize potential hemodynamic changes. Upon inspection of the abdominal cavity, the peritoneal shunt was identified and had been reduced by creation of the pneumoperitoneum. The shunt catheter length seemed appropriate to accommodate the child's growth and was left intact. The internal inguinal rings on both sides were easily visualized and were noted to have patent inguinal canals (Fig. 2). Our standard laparoscopic-assisted percutaneous technique to ligate both internal inguinal rings was used to repair the hernias (Fig. 3).
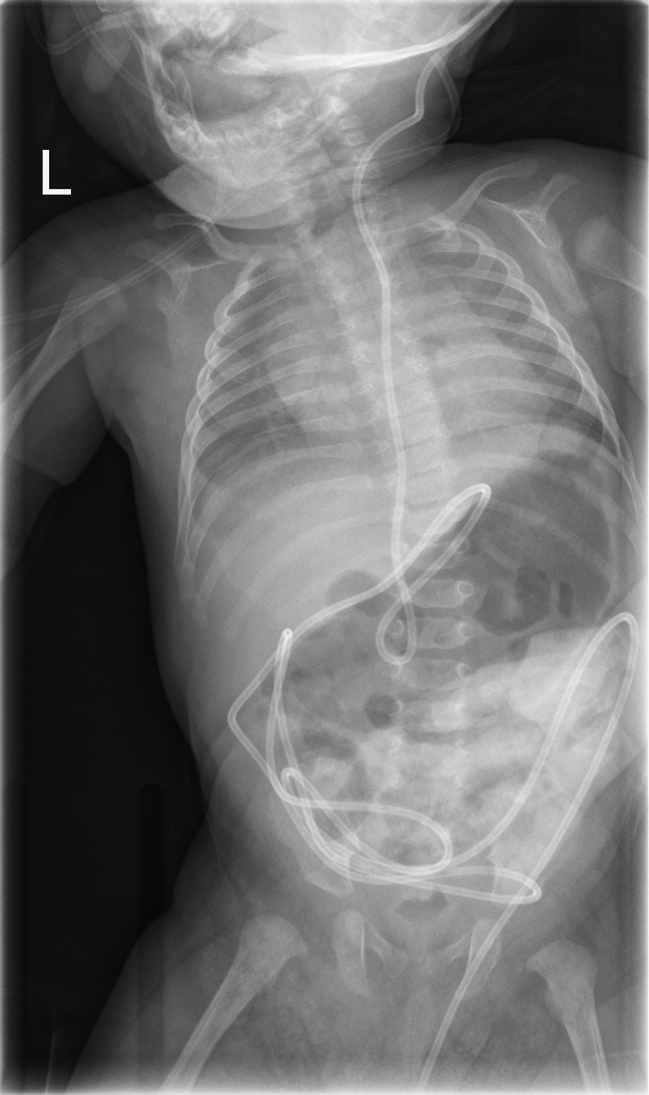
Abdominal x-ray demonstrating the shunt catheter present in the left scrotum.
Despite the cardiac anomalies, the baby had no perioperative hemodynamic events and was able to be extubated at the conclusion of the procedure. He had no postoperative complications, and at a 2-week follow-up visit, there were no recurrent hernias on examination; the incision was well healed with an excellent cosmetic result.
Discussion
A PPV is a common finding at birth but obliterates naturally, resulting in two-thirds of hydroceles resolving by 1 year of age. 4 VP shunts have been associated with a 15% increased incidence of indirect inguinal hernias and hydroceles. 5 The predominant mechanism proposed for this finding is increased intraabdominal pressure due to diverted cerebrospinal fluid that accumulates in excess of the peritoneal absorption rate. 6 This can potentially lead to a delayed closure of the PPV, thereby increasing the risk of shunt migration into the scrotum.
When operating for a migrated VP shunt, numerous reports have been published on whether to explore the contralateral groin for a PPV. The main advantage is avoiding migration of the VP shunt into a contralateral inguinal hernia after repair of the initial hernia. Repairing a contralateral hernia also avoids herniation of visceral organs and their subsequent incarceration and avoids potential risks of a second operation and anesthetic associated a metachronous contralateral hernia. 7
This case demonstrates the benefits of a laparoscopic approach, which include the ease of assessing the contralateral internal ring, a potentially improved cosmesis, and eliminating the need to dissect the vas deferens and spermatic cord vessels, possibly reducing testicular atrophy. 8 As in this case, the creation of pneumoperitoneum may also spontaneously reduce the shunt and other involved sac contents back into the abdominal cavity, thereby making the operation technically easier and faster.
Conclusions
In patients with VP shunt migration into the scrotum, the contralateral side should be assessed for hernia in this high-risk population. Laparoscopy, a powerful tool in the armamentarium of a minimally invasive surgeon, allows easy reduction of the shunt, allows evaluation of the contralateral internal ring, and repair without any additional incisions. A laparoscopic repair also avoids dissection of the vas deferens and spermatic cord vessels and may also provide better cosmesis. In cases of a migrated VP shunt, we conclude that a laparoscopic reduction, examination, and inguinal hernia repair should be considered instead of an open exploration.
Footnotes
Disclosure Statement
No competing financial interests exist.