
Abstract
Abstract
Objective:
To assess the feasibility, safety, and short-term outcome of a transumbilical, single-port, totally extraperitoneal (TEP) laparoscopic inguinal hernia repair, using a homemade port and a conventional instrument.
Patients and Methods:
Thirty consecutive patients with inguinal hernias (including 20% with bilateral inguinal hernias) underwent a transumbilical, single-port, TEP laparoscopic hernia (LH) repair using a homemade port composed of a segment of corrugated anesthesia tube and a pair of surgical gloves. All operation procedures were done using conventional laparoscopic instruments with manually angled shafts in the same manner as standard multiple-port surgeries, but using the reverse hand technique.
Results:
All the procedures were completed uneventfully and did not require additional ports. Operation times averaged 98.3±26.7 minutes for the unilateral LH and 121.4±13.5 minutes for the bilateral LH. There were no perioperative complications except for 2 patients (7%) who developed wound seromas, which resolved after conservative treatment. No hernia recurred during the 6-month follow-up.
Conclusion:
A transumbilical, single-port, TEP laparoscopic hernioplasty using a homemade port and a conventional instrument permitted nearly scarless surgery for the treatment of inguinal hernias. Further studies are necessary before this approach can be recommended as a standard procedure.
Introduction
The development of various ports like the Uni-X™ (Pnavel Systems, Inc., Morganville, NJ), the R-Port® (Advanced Surgical Concepts, Bray, Wicklow, Ireland), and the SILS Port (Covidien, Mansfield, MA) has allowed the introduction of multiple instruments through a single port inserted at the umbilicus. 4 However, these commercialized ports are expensive and not currently available worldwide. Consequently, we devised the Uen port, a homemade laparoscopic port composed of two pieces of equipment readily available in the operating room. 5
Patients and Methods
Between July and October 2009, 30 consecutive patients with inguinal hernias (including 6 cases of bilateral inguinal hernia) were chosen for single-port laparoscopic hernia (LH) repair using the new Uen port. Appropriate consents were obtained from the patients and the hospital ethics committee. All patients received one preoperative prophylactic dose of antibiotics (1 g of cefazoline) after anesthesia. Initially, a cured incision was made along the lower umbilical border, and a 2.0-cm-long fascial wound was made over the anterior rectus sheath. With the rectus muscle retracted, we entered the properitoneal space and further dissected with a balloon trocar. Then, the Uen port (Fig. 1) was guided into the properitoneal space, allowing for the insertion of multiple laparoscopic instruments at the same time without gas leakage. After establishing the CO2 pneumoproperitoneum in 12 mm Hg, we performed the single-port LH repair, using a 10-mm 0° laparoscopic camera and traditional laparoscopic instruments whose shafts we had bent manually. The surgery was completed in basically the same manner as the conventional approach except that we used the reverse hand manipulation technique (Fig. 2). The operation procedures are summarized in Figure 3.

Formation of the Uen port. A segment of corrugated anesthesia tube, three shortened 10-mm trocars, and a suction tube were inserted into the opened thumb and four fingers of a pair of surgical gloves:

Manipulation in the reverse hand manner.

Summary of operation procedures.
Results
All of the surgical procedures were completed uneventfully without the need for additional ports. There were no perioperative complications except for 2 patients (7%) who developed wound seromas, which resolved after conservative treatment. Operation times averaged 98.3±26.7 minutes for the unilateral LH and 121.4±13.5 minutes for the bilateral LH. Although the operation time seems longer, it decreases progressively after the learning curve (Fig. 4). The median postoperative hospital stay was 1.85 days. No hernias recurred during the following 6 months.
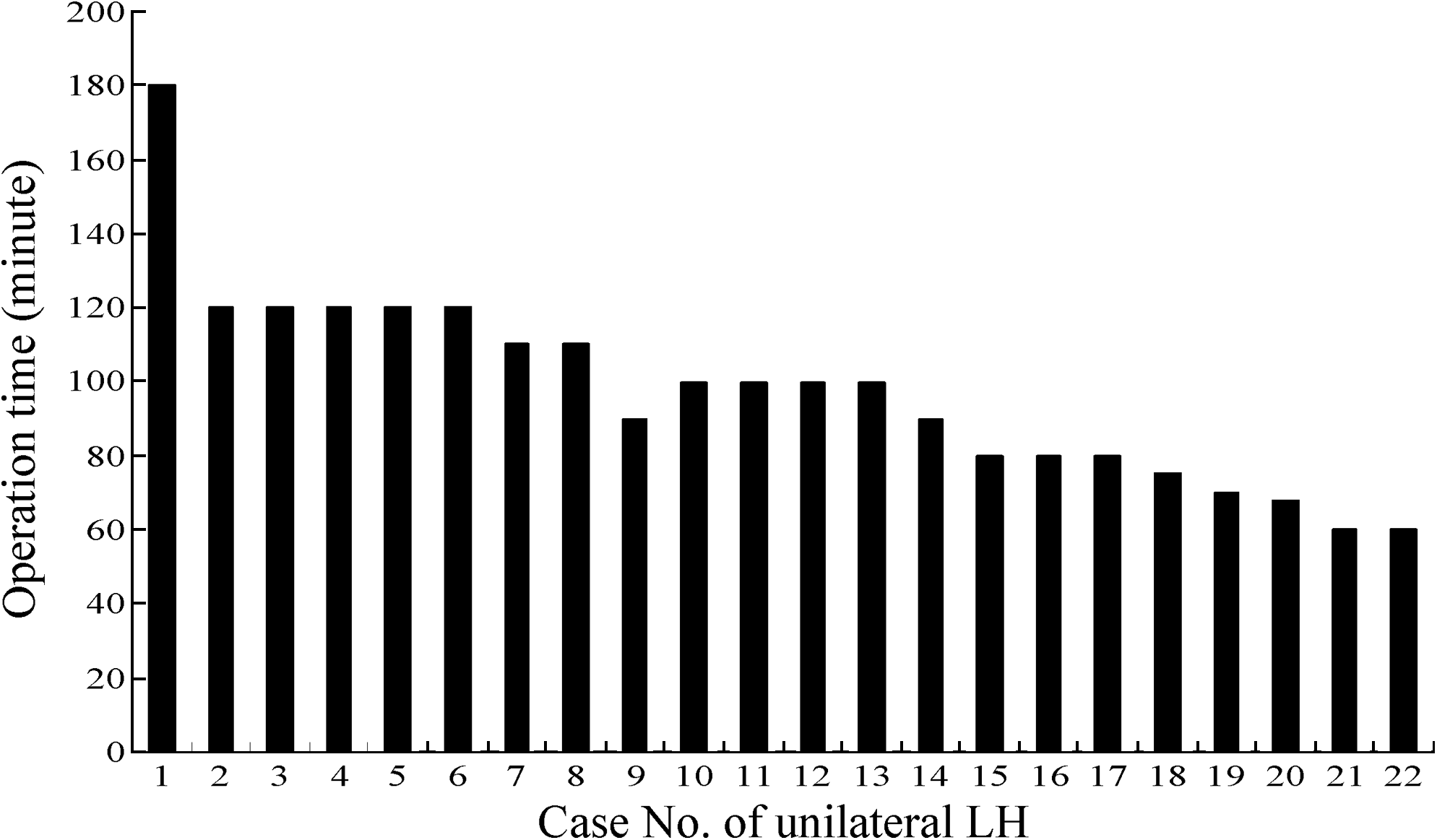
The operation time of patients undergoing unilateral single-port laparoscopic hernia (LH) repair.
Discussion
The rapid improvement in laparoscopic techniques has led to an evolution in surgical techniques. Scarless surgery is a rapidly progressing field, combining cosmetic advantages with the surgical and patient recovery advantages of minimal invasion. One of the pioneering uses of scarless surgery is the transumbilical single-port laparoscopic technique, in which the surgical scar is virtually concealed within the umbilicus.
The homemade laparoscopic access port (Uen port) reported in this study can be simply assembled with materials readily available in the operating room and has been used in many kinds of SILS operations, such as laparoscopic cholecystectomies, 5 appendectomies, etc. In comparison with the commercially available single-port devices, the Uen port has a couple of advantages, including that (1) it can be easily and rapidly inserted into or removed from the umbilical incision because it is compressible and (2) it can replace expensive single-port devices and specially designed instruments, thereby reducing overall costs.
According to the results of our study, each intraoperative step of a single-port LH repair can be accomplished with confidence using the Uen port along with traditional laparoscopic instruments with manually angled shafts. The single-port totally extraperitoneal (TEP) inguinal hernioplasty reported in this study is essentially the same as a multi-port surgery and achieved a high success rate. However, the operation time remains a problem. Improving the surgical technique or instruments to expedite the operation procedures is required before single-port TEP inguinal hernioplasty can be recommended as a standard procedure. More studies including surgical invasiveness, patient recovery, and postoperative pain scale are being carried out.
Footnotes
Disclosure Statement
No competing financial interests exist.