
Abstract
Abstract
Purpose:
To report our surgical technique and initial experience with robot-assisted laparoscopic radical cystectomy (RARC) with total intracorporeal urinary diversion compared with an extracorporeal method.
Subjects and Methods:
In total, 42 patients underwent RARC by a single surgeon at our institute for clinically localized bladder cancer. Among these, 4 patients underwent RARC with complete intracorporeal urinary diversion. An ileal conduit was achieved in 3 patients, and an orthotopic neobladder was created in 1 patient. Our surgical technique is presented in detail, and the intracorporeal cases were compared with 38 previous extracorporeal diversion cases for perioperative outcome, postoperative oncologic outcome, and complications.
Results:
Three men and 1 woman underwent complete intracorporeal urinary diversion. In patients receiving ileal conduits the mean total operative time was 510 minutes, and the estimated blood loss was 400 mL. In the patient receiving an ileal neobladder the total operative time was 585 minutes, and the estimated blood loss was 500 mL. Mean time to flatus was 60 hours, and no intraoperative or postoperative major complications occurred. Surgical margins were negative with no positive lymph nodes. Compared with extracorporeal cases, the mean total operative time for RARC was significantly longer, but perioperative outcomes of estimated blood loss, time to flatus, and postoperative oncologic outcomes were not significantly different.
Conclusions:
Our initial experience showed that RARC with complete intracorporeal urinary diversion is feasible based on perioperative data and oncologic features. However, in this small case series, we observed no definite benefits associated with intracorporeal urinary diversion over extracorporeal urinary diversion except for better cosmesis. Long-term, large-scale, prospective comparative studies will be needed to demonstrate the benefit of intracorporeal urinary diversion.
Introduction
ICUD using pure laparoscopy is associated with higher complication rates, whereas robotic-assisted laparoscopic intracorporeal diversions appear to be more favorable, with acceptable operative and short-term clinical outcomes, although only a few cases have been reported.3,4 Along with three-dimensional vision, use of EndoWrist® (Ethicon Endo-Surgery) instruments makes laparoscopic suturing easier than it is in pure laparoscopy, and it is expected that reconstructive surgery involving suturing can be performed robotically. The merits of robot-assisted surgery can be maximized in reconstructive operations such as urethrovesical anastomosis in robotic prostatectomy. Robotic systems can make total ICUDs safer and more feasible, maximizing the advantages of robotic systems. In this article, we report our surgical technique and initial experience with RARC with total ICUD, comparing it with our previous extracorporeal method.
Subjects and Methods
Patients
The study involved a consecutive series of 42 patients who underwent RARC with pelvic lymph node dissection (PLND) by a single surgeon (S.H. Kang) from August 2007 to April 2011. Among these was a consecutive series of 4 recent patients (3 men and 1 woman) who underwent RARC and a total ICUD between February and April 2011 for recurrent T1, high-grade transitional cell carcinoma of the bladder. None of the patients underwent preoperative radiotherapy or chemotherapy. The ICUD group (n=4) was compared with an ECUD group (n=38). Perioperative outcomes including mean operative time, estimated blood loss, postoperative oncologic outcomes, and postoperative complications were compared.
Surgical technique
The surgical technique used for RARC with PLND, including basic positioning and port placement, was previously described.5,6 At our institute, RARC is usually performed after PLND. In this study, we describe only the surgical technique for total ICUD.
Total ICUD
Orthotopic neobladder-modified Camey pouch
Before urinary diversion, a 60-cm segment of bowel was identified approximately 15 cm proximal to the ileocecal valve. The midportion of the loop, which reached the urethra without tension, was selected (Fig. 1). After it was ensured that the mesentery was long enough for the bowel to reach the urethra, a tag was introduced at the distal end of the ileum and hung on the anterior abdominal wall. The selected ileum was resected with an Endo GIA™ stapler (Covidien Surgical), and small bowel mesentery dissection was performed to the medial portion using LigaSure™ (Covidien) (5 mm) without destroying the mesenteric vasculature. Trimming was performed robotically at the antimesenteric corners of both staple lines to re-establish bowel continuity. The ends of the small bowel were secured together with silk stay sutures at the antimesenteric sites 5 cm from the stapled ends. Bowel continuity was achieved intracorporeally with a side-to-side anastomosis using the Endo GIA stapler (Fig. 2). Then, another transverse firing was used to overlap the original rows of staples over the remaining opening. To imbricate the staple lines, interrupted sutures were inserted using the robotic arms.
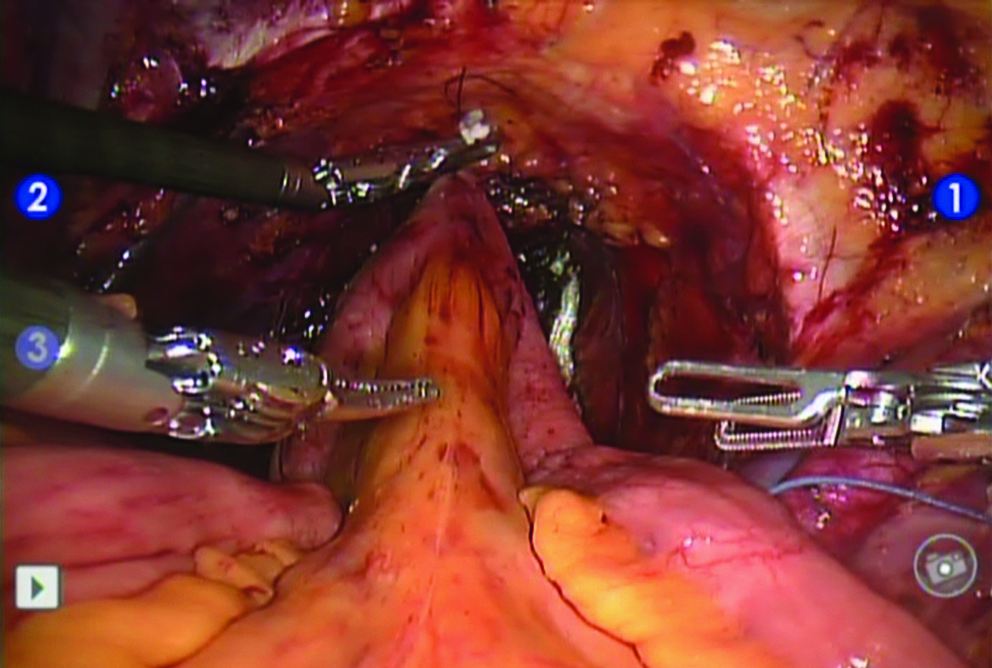
The midportion of the loop, which reached the urethra without tension.
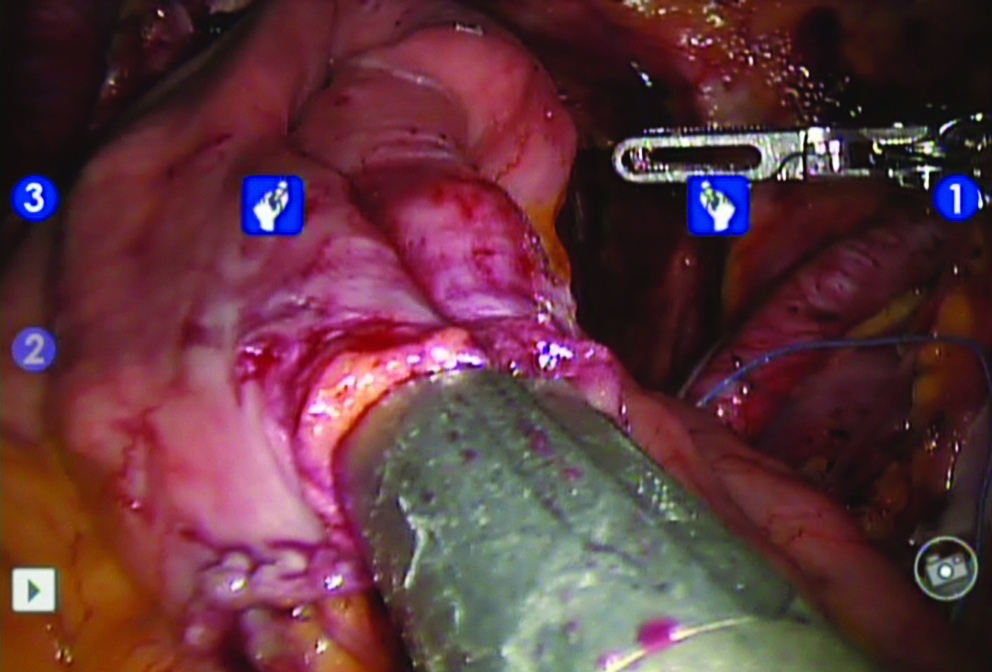
A side-to-side anastomosis using the Endo GIA stapler.
The isolated ileum was placed near the urethral opening against gravity in an inverted U-shape. A urethral neobladder anastomosis was performed before ileal tubularization. A 20 French opening was made in the antimesenteric portion of the top of the inverted U-shaped isolated rim. Then, a van Velthoven running anastomosis was performed using a double-armed suture with knots (Fig. 3). Next, an 18 French Foley catheter was inserted into the neobladder before the anastomotic suture was tied. The stapled ends of the isolated segment were excised, and the ileal segment was opened on the antimesenteric border and folded into an inverted U-shape. The inner edges of the U-shape were sutured with running 3-0 Vicryl™ (Ethicon) sutures. The lateral edges of the ileal U-shape were reapproximated starting near the urethroneobladder anastomosis to form a large-bore tube. Before the ileoureteral anastomosis, the cephalad 6 cm of the anterior wall was left open.
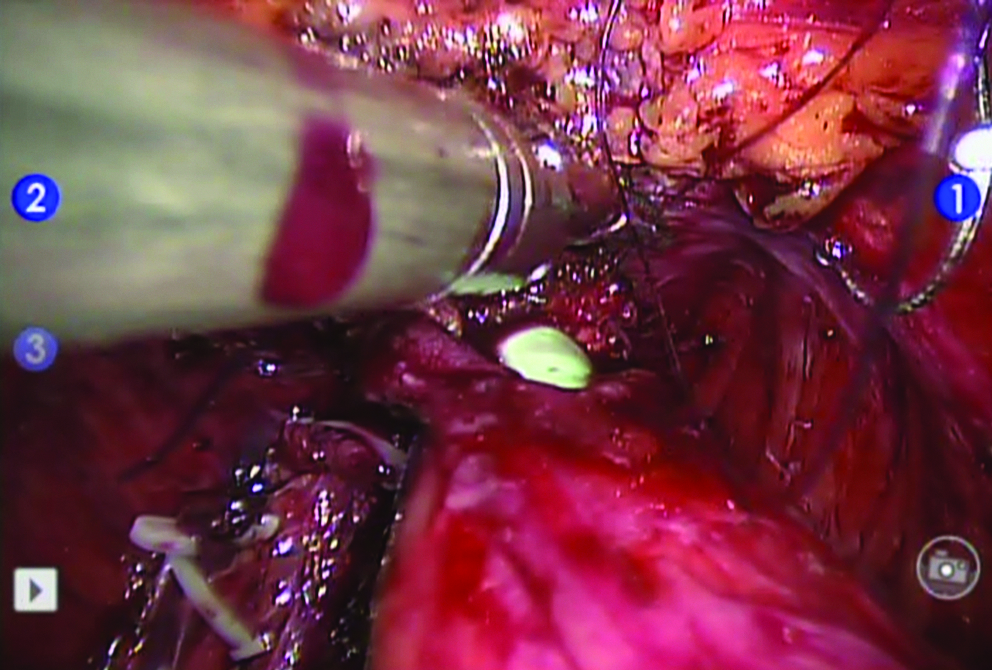
Urethroileal anastomosis in an orthotopic ileal neobladder.
The ureter was transected and spatulated, and the ileoureteral anastomosis was made in a refluxing manner at the posterior wall of the pouch. After a hole was created in the ileum, an interrupted 4-0 Vicryl suture was used for the anastomosis. Before the anastomosis was finished, a ureteral catheter was inserted into the ureters. They were then extracted out of the abdomen through the remaining opening in the anterior wall of the pouch (Fig. 4). The remainder of the anterior wall was closed to fasten the ureteral catheters. The remainder of the pouch was subsequently closed.

Postoperative image from a totally intracorporeal neobladder case.
Irrigation of the pouch and filling were performed to confirm a watertight anastomosis and pouch closure. The specimen was extracted through the camera port at the umbilicus, which was extended to 4 cm (Fig. 4).
Ileal conduit: Bricker (separate) ureteroileal anastomosis technique
After the ileocecal valve was visualized, bowel resection was performed for 15 cm in the same manner as described for the neobladder using an Endo GIA stapler. The stapling line at the proximal end of the ileal conduit was removed to reduce stone formation, and the proximal end was closed with a continuous suture. The seromuscular layer of the bowel was opened at the site where the left ureter was to be implanted. Each end of the spatulated ureter was approximated at the bowel opening and placed with stay sutures. While the stay sutures were held by the third robotic arm and an assistant, three or four interrupted sutures were placed between the two stay sutures. Using the stay sutures, the opposite site was exposed, and before suturing, a double J catheter was inserted into the ureter. In the case of the left ureter, a double J catheter was inserted through the assistant's right hand port with minimal resistance. The left ureter implantation was then completed. A double J catheter was then inserted in the right ureter through the assistant's left hand port with minimal resistance.
Ileal conduit: Wallace (conjoined) ureteroileal anastomosis technique technique
After a 15-cm ileal conduit was created, both of the stapled lines were removed using scissors. While both ureters were pulled with the third arm, spatulation of the ureters was performed. The posterior sides of the ureters were conjoined side to side. One side of the conjoined ureters was sutured to one side of the proximal site in the conduit. Then, before the opposing side was closed, the ureteral catheters were inserted through the distal end of the conduit and out the proximal end into the ureters. Finally, one side of the conjoined ureters was approximated at the conduit.
Results
In total, 42 RARC procedures were performed at our institution during the study period. This included 25 ileal conduits, with 3 recent cases of ileal conduits performed through total ICUD. Two were performed using the Bricker method and one using the Wallace method. In total, 15 cases of orthotopic neobladder were performed, the most recent using the intracorporeal method (Table 1).
RARC, robot-assisted radical cystectomy.
Table 2 outlines patient characteristics. No significant differences were observed between the intracorporeal and extracorporeal group, although based on mean age the intracorporeal group seemed to be relatively older than the extracorporeal group. Except for age, no significant differences were observed in sex, body mass index, or American Society of Anesthesiologists score. No patients underwent preoperative radiotherapy or chemotherapy in the intracorporeal cases. All four patients in the intracorporeal group received an extended PLND, beginning at the inferior mesenteric artery or aortic bifurcation and including the common iliac, external iliac vessels, and presacral and obturator fossa.
ASA, American Society of Anesthesiologists; RT, radiation therapy; PLND, pelvic lymph node dissection.
For the ileal conduit cases, the total operation time for intracorporeal diversion was 510 minutes, and the mean time for urinary diversion was 200 minutes. Table 3 compares perioperative outcomes between the two groups. Compared with the 22 extracorporeal cases, the mean operation time in the intracorporeal group was significantly longer. However, except for the mean total operative time, no significant differences were observed between the groups for the mean time for cystectomy plus PLND, perioperative parameters including estimated blood loss, mean time to flatus, or mean hospital stay (Table 3).
EBL, estimated blood loss.
The mean total operation time in the intracorporeal diversion for the neobladder case was 545 minutes, and the mean time for cystectomy plus PLND was 200 minutes. Compared with the 14 extracorporeal cases, the mean operation time seemed to be shorter in the extracorporeal method (Table 4). However, comparison with extracorporeal cases is difficult because only one neobladder patient underwent the intracorporeal method.
Time for intracorporeal neobladder pouch formation and intracorporeal urethroileal anastomosis.
Time for extracorporeal neobladder pouch formation and intracorporeal urethroileal anastomosis.
Pathologic stage was significantly lower in the intracorporeal group (P=.008). The patients in the intracorporeal cases were all transitional cell carcinomas with no other type of cancer. The mean retrieved number of lymph nodes was 29.7, with more in the intracorporeal group, although this was not a significant difference. No positive surgical margins occurred among the intracorporeal cases. In the first 6 postoperative months, no intra- or postoperative major complications in the intracorporeal group occurred, as shown for the extracorporeal cases. One patient in the intracorporeal group showed a paralytic ileus, which was resolved by supportive care (Table 5).
Figure 4 shows postoperative wounds in the intracorporeal neobladder case. The specimen was withdrawn through the extension of the umbilical port, requiring no midline incision for bowel extraction. Figure 5 shows the female ileal conduit case.

Postoperative image from a totally intracorporeal ileal conduit case in a female.
Discussion
Radical cystectomy (RC) is the standard treatment for muscle-invasive and high-risk superficial bladder cancer, but it is a formidable operation that is associated with a high complication rate. 7 When laparoscopy is applied to RC, it may result in less blood loss, decreased postoperative pain, and quicker bowel recovery.8,9 However, the use of LRC has been limited and is performed by only a few expert laparoscopic surgeons.8,9 Reports in which ICUD was performed with pure laparoscopy are rare.9–12 In these reports, the RC portion of the procedure is feasible and safe. All the major complications in these reports were related to ICUD. Haber et al. 9 reported on their experience with 17 patients who underwent LRC with pure laparoscopic urinary diversion. They reported that 5 patients (29%) had major complications that required reoperation for bowel leakage and urine extravasation and sepsis, so a pure laparoscopic approach was abandoned. Cathelineau and Jaffe 8 reported that the main role of laparoscopy in RC is the removal of the bladder and that ECUD should be considered the optimal technique for LRC.
Recently, several studies have reported RC using the da Vinci® Surgical System (Intuitive Surgical) robot, and RARC is already superseding LRC.1,6 The robot system complements laparoscopy with superior visibility, achieved by magnification and stereotactic vision, and fine EndoWrist instruments, allowing easier intracorporeal suturing. These robotic advantages can be maximized when performing reconstructive surgery. This offers ease of urethrovesical anastomosis in robot-assisted radical prostatectomy. Therefore, in contrast with pure LRC, total ICUD using the da Vinci Surgical System robot is expected to be accomplished safely without major morbidity. Pruthi et al. 3 reported on their initial experience with robotic-assisted laparoscopic ICUD, in which it appeared to have favorable short-term clinical results in carefully selected patients. The complication rates in the ICUD group were similar to those in the ECUD group, and narcotic requirement decreased in the ICUD group. Guru et al. 13 also reported that overall operative time and intraoperative complications between the ICUD and ECUD groups were similar. However, most of the reported urinary diversions in the RARC series were performed through extracorporeal methods. 2 We previously reported results from our experience with ECUD.5,6
Urinary diversion performed using a total intracorporeal method can have additional benefits, including less incisional pain, decreased bowel exposure and desiccation, and the potential for decreased fluid imbalances.3,9 However, determining whether to create a completely ICUD versus performing the reconstruction extracorporeally is still a controversial and critical issue. Haber et al. 9 reported outcomes of pure LRC with intracorporeal diversion versus an open-assisted approach. The reason they abandoned pure LRC was its higher major morbidity. The authors also commented that a single surgeon typically remained in place and performed the entire procedure, so prolonged operation time might have contributed to the complications. However, recent comparative studies using the da Vinci Surgical System robot showed different results with pure LRC. Pruthi et al. 3 compared 12 RARC with ICUD cases with 20 ECUD cases: Short-term (within 30 days of surgery) complication rates were similar between ICUD (n=5 patients) and ECUD (n=8 patients). Although the operation time was longer in ICUD patients (5.3 hours) compared with ECUD patients (4.2 hours), the authors did not feel that these were excessive lengths and posed excessive complications. Guru et al. 13 reported a comparison between 13 ICUDs and 13 ECUDs, with four complications in the intracorporeal group and five in the extracorporeal group in a 3-month follow-up. The authors found no significant difference in diversion time between ICUD and ECUD (159 minutes versus 120 minutes) and saw a trend toward lower operation times for ICUD. In our ileal conduit cases, the total operation time in the ICUD group was longer than in the ECUD group, and the time for ICUD was about 200 minutes (3.3 hours). The time for ICUD was comparable to the 3 hours reported by Pruthi et al. 3 and 159 minutes reported by Guru et al. 13 We did not feel that our initial experience led to the complications or the morbidity. In addition, no patients in our study in the intracorporeal group had major complications within 6 months. We anticipate that the duration of operation will shorten as we gain experience in ICUD and refine our techniques. Our initial neobladder case showed comparable results with previous initial reports. Beecken et al. 14 reported the first case, with an 8.5-hour operation time and 200 mL blood loss. Sala et al. 15 reported a longer operation time (12 hours) and a 100 mL blood loss. Our operation time was about 9 hours, and the estimated blood loss was 500 mL. We believe that the acceptable results of our initial experience are due to our previous experience with over 40 cases of RARC.
Several different techniques and operation steps have been described for orthotopic neobladders and performing urethroneovesical anastomosis using ECUD or ICUD. Menon et al. 16 reported an extracorporeal neobladder formation technique in 2003. After neobladder formation was performed extracorporeally through the midline small incision used for retrieving the specimen, the reconstructed neobladder pouch was placed in the pelvis, and the abdominal incision was closed. Urethroneobladder anastomosis was then performed intracorporeally after the robotic system was redocked. Another method is exteriorizing the bowel through the suprapubic incision, and urethroneovesical anastomosis is done manually without redocking the da Vinci Surgical System robot. 6 This technique was used to solve the tension-against-gravity issue that results from the urethroneovesical anastomosis. As described in a previous report, we performed urethroneovesical anastomosis after redocking the robot. 6 During this procedure, we felt tension in several extracorporeal cases when the urethroneovesical anastomosis was performed robotically in the steep Trendelenberg position after extracorporeal neobladder formation. These cases took longer because of tension created by gravity during the urethroneovesical anastomosis. However, in our initial intracorporeal neobladder case, we had already performed the urethroileal anastomosis in the tension-free position before formation of the neobladder. Therefore, the urethroileal anastomosis was easier. Although this was the first case of total intracorporeal orthotopic neobladder, the total operation time difference between the ICUD and the ECUD groups for orthotopic neobladder cases (545 minutes versus 497 minutes) was less compared with the ideal conduit cases (510 minutes versus 420 minutes). This might be because the time for releasing docking and redocking can be omitted and the urethroneovesical anastomosis was easier. ICUD might be able to solve the tension-against-gravity issue that results from the urethroneovesical anastomosis.
Different orders of surgical steps are used between bowel recontinuity and urethroileal anastomosis in total intracorporeal orthotopic neobladder cases. Wiklund et al. 17 performed urethroileal anastomosis before the bowel harvest. However, the techniques used by Pruthi et al. 3 and Sala et al. 15 had urethroileal anastomosis after bowel harvest and restoring bowel recontinuity. Similar to the latter studies, we restored the bowel continuity early and then performed complete urethroileal anastomosis. Whether performing anastomosis before bowel harvest is beneficial compared with performing the procedures in the reverse order is unknown. We hypothesized that performing the urethroileal anastomosis in advance would cause a more difficult surgical procedure. Greater precision and care would be required not re-disrupting the urethroneobladder anastomosis site for the entire duration of the bowel harvest. Our technique involves using the stay suture to preset the anastomosis site, thereby eliminating any tension, and reducing the possibility of disruption during bowel harvest, thus creating a safer, efficient surgery environment. However, further discussion about this matter is needed.
Our study did not show the previously mentioned potential benefits from ICUD such as less incisional pain, decreased bowel exposure and desiccation, and the potential for decreased fluid imbalances.3,9 However, there was no increase in the major complications related with ICUD such as sepsis from the internal soiling, and prolonged operative time did not lead to an increase in morbidity. In addition, we might have solved the tension-against-gravity issue. Finally, ICUD has a cosmetic advantage. In particular, the specimen is extracted through the vagina in women, so an extension of the umbilical incision was not needed.
There are several limitations to this study. First, it was not a randomized, comparative study. Thus, biases in the selection of patients for the initial ICUD group were possible. Indeed, the ICUD group had a lower stage of bladder cancer, had no experience of either radiation therapy or chemotherapy, and had no history of prior abdominal surgery. Our study also had a relatively short follow-up period, which might not have allowed enough time for complications to become apparent.
As shown in our comparison with ECUD, although the oncologic and perioperative outcomes were comparable, no definite benefit was observed except for the cosmetic aspect. For the practical application of intracorporeal neobladder formation, more global data with respect to long-term outcomes and larger series of cases are required.
Conclusions
Robot-assisted ICUD can be accomplished safely with acceptable operative times, even in our early experience with the technique. Larger series and long-term favorable outcomes will be required to support the addition of this technique to the current repertoire of minimally invasive surgeries for bladder cancer.
Footnotes
Acknowledgments
This study was supported by a research grant from Korea University Medical College (Seoul, Korea).
Disclosure Statement
No competing financial interests exist.