
Abstract
Abstract
Purpose:
To test the hypothesis that during laparoscopic hernia repair, partial resection of the distal sac along with suture ligation of the neck is better than simple transection and ligation.
Methods:
The following two techniques of laparoscopic hernia repair were compared: Group I, circumferential incision of peritoneum at the deep ring and partial resection of the distal sac and suture ligation at the neck; versus Group II, circumferential incision of the peritoneum at the deep ring and suture ligation at the neck. Twenty-five cases of inguinal hernia were randomly selected in each group between the age group of 6 months to 12 years. The outcome measures were recurrence, intra- or postoperative complications, and time taken for surgery.
Results:
There were no recurrences in either group. Other parameters for comparison were also not statistically different between the two groups. There was no conversion.
Conclusions:
Although partial resection of the sac has been an essential step in open hernia repair over five decades, its value has been questioned by our study, because omitting this step during laparoscopic repair has not adversely affected the outcomes. Partial resection of the sac is not a necessary component of hernia repair. It is a technical necessity of the open approach. Therefore, omitting this step in laparoscopic repair does not adversely affect the outcome.
Introduction
We believe that there is a need to develop a standard technique of laparoscopic hernia repair in children that incorporates the essential steps of herniotomy—that is, division of the sac, partial excision of the sac, and suture ligation at the neck of the sac. The aim of our study was to test the hypothesis that during laparoscopic hernia repair, partial resection of the distal sac along with suture ligation of the neck is superior to transection and ligation alone.
Subjects and Methods
Fifty pediatric patients with indirect inguinal hernias in the age range of 6 months to 12 years were randomized into two groups for laparoscopic repair by two different techniques: Group I (n=25) received repair by circumferential incision of the peritoneum at the deep ring and partial resection of the distal sac and suture ligation at the neck; and Group II (n=25) received circumferential incision of the peritoneum at the deep ring and suture ligation at the neck.
The diagnosis of hernia was made by history and physical examination. Patients were also included on the basis of history alone if the history was reliable but examination could not confirm a hernia.
Patients with ascites, connective tissue disorders, ventriculoperitoneal shunt, recurrent hernia, and incarcerated hernia were excluded from the study.
Operative technique
Open cannulation at umbilicus with a 5- or 10-mm port was used in all cases. Two working ports (3–5 mm), one in each flank, were inserted under vision. Inguinal anatomy was visualized on both sides to define the defect, contents, and the contralateral side (Fig. 1A). The contents, if any, were reduced. To protect the vas and vessels, the peritoneum at the deep ring was sharply incised circumferentially. This was achieved by lifting the peritoneum between the vas and vessels and making a small nick. This opening was gently widened, and the vas and vessels were swept away under direct vision for a span of about 5 mm (Fig. 1B). Once the vas and vessels were free from the peritoneal attachment, the incision of the peritoneum was completed all around the circumference (Fig. 2A). No electrocautery was used in the immediate vicinity of the vas and vessels. In Group I, after circumferential incision of peritoneum at the deep ring, the distal sac was held with a pair of Maryland forceps in the lateral location (away from the vas and vessels) and pulled back into the abdominal cavity (Fig. 2B). It was gently separated from the vas and vessels for about 5–10 mm, and this freed portion of the sac was also excised, taking care to keep the vas and vessels always under vision and safe. Adequacy of this step was judged by complete disappearance of the distal sac in the scrotum. The proximal edge of the incised peritoneum was then closed with one or two sutures of 4/0 polyglactin (Vicryl®, Ethicon, Johnson and Johnson) (Fig. 3). The testis was confirmed in the scrotum. In Group II, after circumferential peritoneal incision, the step of partial excision of the sac was omitted. The proximal edge of the incised peritoneum was closed as in Group I. Therefore, the two groups differed only in one aspect (i.e., partial resection of the sac): It was performed in Group I and not performed in Group II. All other aspects of the technique were the same in both groups.


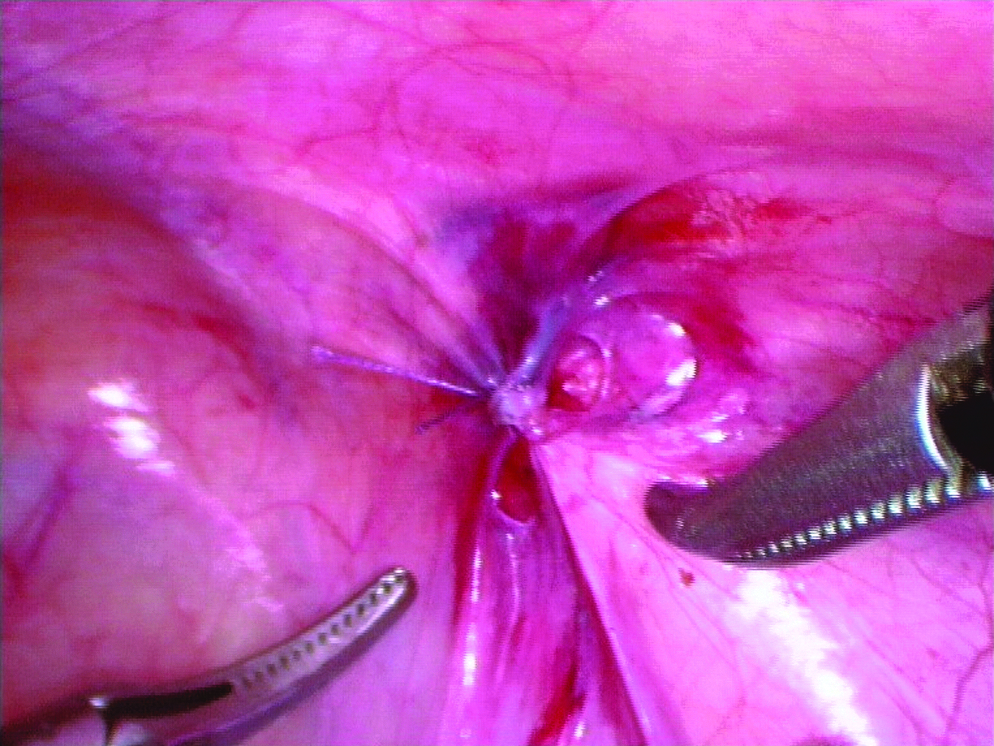
Peritoneum sutured.
Postoperative pain was assessed by either the Face, Leg, Activity, Crying, and Consolability Scale 14 in patients below 7 years of age or the Visual Analogue Scale 15 in patients above 7 years of age. Assessment was performed every 2 hours for a maximum of 24 hours. Analgesics were administered as per the score. Any breakthrough pain also received similar analgesics. The first dose was given as a suppository on the operating table itself after recovery from anesthesia. Further doses were given orally. The patient was considered fit to be sent home if he or she remained pain-free or in mild pain for 4 hours continuously and had accepted an oral feed.
The outcomes were measured using the following parameters: recurrence, intra- or postoperative complications, duration of surgery, analgesic requirements, and time for discharge from the surgery center.
The variables were analyzed with the help of SPSS (Chicago, IL) statistical software version 12.0. The significance of differences in various variables between the two groups was measured by chi-squared test and Fischer's exact test.
Results
There were 19 boys and 6 girls in Group I and 21 boys and 4 girls in Group II. Clinically, 24 patients had right-sided hernia, 22 had left-sided hernia, and 4 had bilateral hernia. Seven of the 22 (31.8%) clinically left hernia cases turned out to be bilateral on laparoscopy. Four of the 24 (16.6%) clinically right hernia cases turned out to be bilateral on laparoscopy. Of the 4 clinically bilateral hernias, only 3 were confirmed bilateral on laparoscopy; the fourth had a hernia only on the left side. Among the girls, of 6 clinically left hernias 2 were found to be bilateral laparoscopically; all 3 clinically bilateral cases were proved to be so on laparoscopy. Among the boys, of 16 clinically left hernias 4 were found to be bilateral on laparoscopy; of 23 right hernias 4 were found to be bilateral on laparoscopy. The single patient with clinically bilateral hernia turned out to have only left-sided hernia on laparoscopy. The change in the distribution of side intraoperatively from unilaterality to bilaterality was evaluated statistically. In boys, preoperatively only 2.5% were suspected as bilateral, but intraoperatively this figure rose to 22.5%. This was statistically significant (P=.036 by McNemar's test).
Operative time was defined as time taken from skin incision to application of Steri-Strips (3M) for skin closure at the port sites. Mean operative time per patient in Group I was 46.74 minutes, and that in Group II was 40.70 minutes. The difference in the mean operative time per patient in the two groups was statistically not significant (P=.186 by Student's t test). The mean time for hospital discharge after surgery was 8 hours 47 minutes for Group I and 8 hours 23 minutes for Group II. In 5 patients the sac contained omentum; in 4 it could be reduced easily into the abdominal cavity, but in one case it had adhered and therefore had to be cut with a harmonic shear. Follow-up ranged from 6 months to 18 months (mean, 12.4 months). No recurrences were observed in either group. No other complications occurred except minor port site infection in 1 case in the early postoperative period.
When pain scores and analgesics requirement were evaluated, all the patients had scores indicative of either mild pain or moderate pain. In accordance with the pain scores, all received paracetamol, diclofenac, or ibuprofen or a combination for postoperative pain. No patient, therefore, required opioids for pain relief, as it was reserved only for severe pain on the scales. Caudal analgesia with bupivacaine was given in 7 patients (3 in Group I and 4 in Group II). The decision to give or not to give caudal analgesia was with the anesthetist. However, almost equal numbers from both groups received this form of analgesia (3 and 4, respectively). If a patient had received caudal analgesia, further requirement of analgesia was limited to an average of 1.1 doses of paracetamol/nonsteroidal anti-inflammatory drug. If a patient had not received caudal analgesia, the average analgesic requirement was 1.84 doses. There was no difference in the analgesic requirement of the two groups. The first dose was given as a suppository on the operating table itself after recovery from anesthesia. Further doses were given orally.
A summary of observations is shown in Table 1.
Discussion
The role of laparoscopy in the management of pediatric hernia has evolved from a simple diagnostic tool (to diagnose a contralateral hernia) to an effective therapeutic option. There have been many reports of successful laparoscopic repairs.2–13,16,17 It is projected to be the future gold standard for hernia care. 1 Despite so much enthusiasm, a standard technique of laparoscopic repair of hernia in children is still elusive. There are at least 16 different techniques reported in the world literature. On the other hand, there is a fairly uniform standard technique of open hernia repair accepted universally for over 50 years.18,19
Our working hypothesis that during laparoscopic hernia repair, partial resection of the distal sac along with suture ligation of the neck is better than simple transection and ligation has been proven wrong by the study. We therefore reviewed the techniques of open hernia repair as described in prominent textbooks and contemporary publications. The books reviewed included Pediatric Surgery (edited by Grosfeld et al.), 20 Operative Pediatric Surgery (edited by Ziegler et al.), 21 and Operative Pediatric Surgery (edited by Coran and Spitz) 22 and the landmark article by Potts et al. 18 In all the descriptions of pediatric hernia repair the essential step has been high ligation of the sac. In all illustrations the sac was separated from the cord structures at a site distal to the neck and divided there. Then the proximal portion of the sac was clear off the vas and vessels until the retroperitoneal fat, which is considered a landmark for the deep ring and where the sac is transfixed. The portion of the sac between the transfixation suture and the point of initial division of the sac is excised. Surgeons universally have followed this technique as originally described by Ladd, Gross, Ferguson, and Potts. Although there have been minor modification adapted by different surgeons at different times, the key element of the technique has remained the same (i.e., high ligation of the sac and resection of the part of the sac immediately distal to the ligature). The importance of these key steps can be judged from the fact that failure to do so (i.e., not ligating the sac high enough) has been believed to be the major cause of recurrence. 23 Even though in the introductory paragraph in the chapter on inguinal hernia in Operative Pediatric Surgery 21 Lloyd writes “some such as Potts and colleague in 1950 supported the principle of high ligation and removal of the hernial sac, an embellishment no longer considered necessary,” the illustrations in the chapter indicate that partial resection of the sac is an inherent necessity to achieve high ligation—the key step. The illustrations in other books also support this.
The need for partial resection of the sac has been questioned by our study. Our data demonstrated that omitting this step during laparoscopic repair has not adversely affected the outcome. Rather, its inclusion increased operative time and, at least theoretically, put the vas and vessels at added risk of injury while the sac is dissected. Reviewing the existing textbooks and contemporary literature on open hernia repair, it becomes evident that most describe partial resection of the sac. While performing laparoscopic repair this “technical step” is completely unnecessary because the hernia is approached from the peritoneal end and tackled just at its origin (i.e., the neck at the deep ring). The cord structures are minimally disturbed and remain visible at all times.
There was no case of recurrence (maximum follow-up of 18 months) observed in any of our patients. All the complications reported were considered minor and did not require any reoperation. There were no complications related to testicular position, size or fixation.
Conclusion
Partial resection of the sac is not a necessary component of hernia repair. It is a common step of the open approach. Therefore, omitting this step in laparoscopic repair does not adversely affect the outcome.
Footnotes
Disclosure Statement
No competing financial interests exist.