
Abstract
Abstract
Acute pancreatitis (AP) in children usually follows a mild course but occasionally may be severally problematic. We report the case of a 12-year-old boy with severe AP who was managed with repeated laparoscopic pancreatic necrosectomy. Three weeks later he represented with a pancreatic pseudocyst that was treated with endoscopic gastrocystotomy. His abdominal pain persisted and a subsequent magnetic resonance cholangiopancreatogram showed multiple gallbladder and common bile duct (CBD) stones that were missed on previous imaging investigations. He underwent laparoscopic cholecystectomy with transcystic exploration of the CBD. The patient is currently well, more than 2 years following the definitive corrective surgery. To the best of our knowledge, this is the first case of laparoscopic pancreatic necrosectomy in a child.
Introduction
Case Report
We report the case of a 12-year-old boy who was transferred to our hospital with severe AP. He was initially admitted with a 1-week history of epigastric pain, amylase of 1360 U/L (normal, 10–220 U/L), and lipase of 602 U/L (normal, <60 U/L). Retroperitoneal collections were seen on abdominal ultrasound. On arrival he was febrile, was hemodynamically stable, and complained of severe abdominal pain. He was admitted to pediatric intensive care unit for monitoring. Empiric intravenous imipenem and morphine patient-controlled analgesia were started. An abdominal computed tomography (CT) scan showed AP with necrosis of the neck and body of the pancreas and large peripancreatic fluid collections (Fig. 1).

Abdominal computed tomography on admission. A large abdominal collection and pancreatic necrosis are apparent.
The patient's condition continued to deteriorate, and 1 week later he required mechanical ventilation and vasopressors support. A second CT scan showed that the peripancreatic collections had increased in size. However, these were not considered accessible to percutaneous drainage. At that time a positive blood culture for Candida albicans was obtained and the patient was taken to the operating room with a diagnosis of infected pancreatic necrosis for laparoscopic debridement.
Laparoscopic drainage of the collections and pancreatic necrosectomy were performed. The abdomen was openly accessed with a 5–12-mm Hasson's trocar through an umbilical incision. A 30°, 10-mm scope was used. Two working ports were inserted in the right and left flanks (10 mm and 5 mm, respectively) and an assistant port was placed in the epigastrium (5 mm). The pneumoperitoneum was set at 12 mmHg. A large 10-mm irrigation/suction shaft was used to facilitate the procedure. The stomach was lifted with an Endoclinch® grasper inserted via the epigastric port and the gastrocolic omentum was opened to gain access to the lesser sac using ultrasonic dissector (Ultrasicion®) and hook diathermy. The collection was identified and opened, with drainage of 500 mL of turbid fluid. The necrotic pancreatic tissue was removed serially with graspers and the cavity was thoroughly irrigated clean with normal saline (Fig. 2). A separate subhepatic collection was also drained. Two large bore drainage tubes were left for daily irrigation. The patient's clinical condition improved following this intervention. After 1 week, a second laparoscopic procedure was performed for further lavage and removal of residual necrotic pancreatic tissue using the same points of entry. The patient was extubated the day after, vasopressors were gradually discontinued, and enteral feeding was re-established.

Operative view. The lesser sac has been accessed and the stomach lifted up
Three weeks later, he developed a recurrence of abdominal pain. The CT scan showed a pancreatic pseudocyst. An endoscopic gastrocystotomy (Fig. 3) was successfully performed. It was not possible to stent the connecting opening because of rapid evacuation and disappearance of the collection.

Endoscopic cystogastrostomy. The pancreatic pseudocyst is bulging through the posterior gastric wall and being suctioned.
There was no obvious explanation for his pancreatitis until he represented with recurrent abdominal pain at which time his magnetic resonance cholangiopancreatogram for the first time showed several gallbladder and CBD stones, measuring 2–3 mm (Fig. 4). An endoscopic retrograde cholangiopancreatogram (ERCP) was attempted, but cannulation of the ampulla was not technically possible even after a papillotomy. At laparoscopic cholecystectomy with an intraoperative cholangiogram, the CBD stones were flushed into the duodenum with a transcystic catheter. The patient recovered well and has remained totally asymptomatic for over 2 years following surgery.
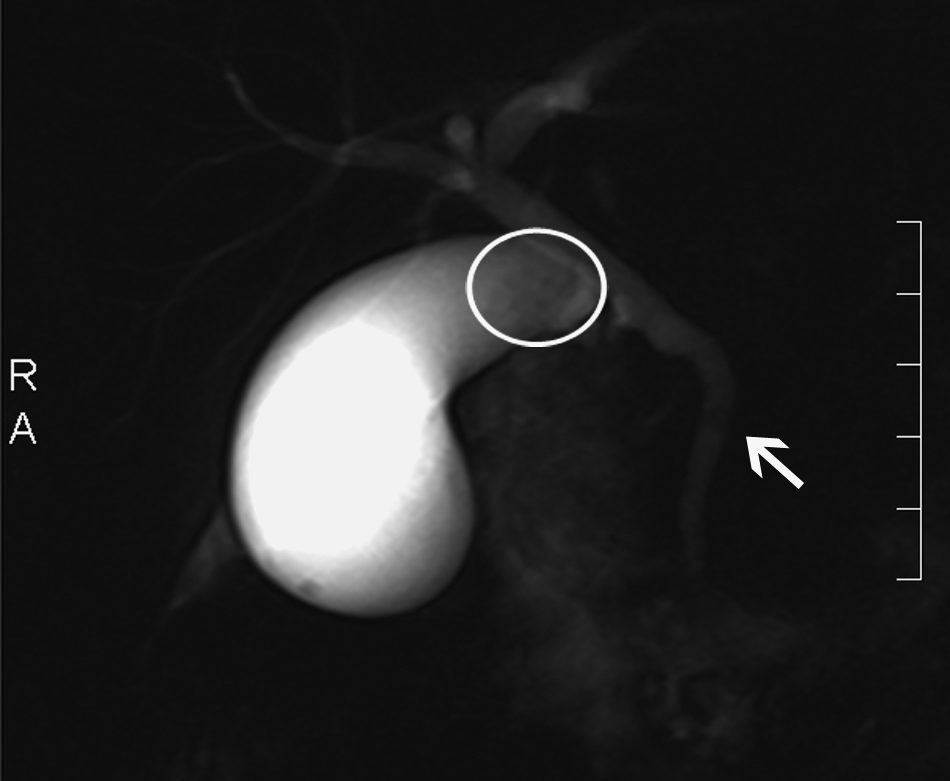
Magnetic resonance cholangiopancreatogram showing multiple small stones in the gallbladder (circle) and CBD (arrow). The absence of dilatation of the CBD is noteworthy. CBD, common bile duct.
Discussion
Even though most of the children with AP present with a mild course, 1 AP may have a high morbidity and mortality. The mortality was as high as 21% in the past 2 and has been recently reported as 9.7%. 3 The etiology of AP in children differs from that of the adults. The most common causes of AP in children are idiopathic pancreatitis, secondary to systemic disease, and trauma, 3 whereas in adults the most common causes are biliary stones and alcohol.
This case report confirms the importance of using, and if necessary repeating, the appropriate imaging investigation in order to identify the cause of AP in children, especially if choledocholithiasis is strongly suspected as happens in the Chilean population. 4 Initial ultrasound missed the gallstones in this case, and there was no obvious CBD dilatation. Unfortunately, ultrasonic examinations are notoriously operator dependant, with sensitivity ranging from 84% to 97%. 5 This case also highlights the usefulness of abdominal CT scans in grading AP and determining its complications, but also its lack of sensitivity in diagnosing gallstones. It has been reported to be unreliable in over three-fourths of patients with CBD stones.5,6
Current indications for surgery in AP are mainly limited to the treatment of its complications. It is interesting to note that 16% of children with AP are diagnosed as an incidental finding during laparotomy. 2 In our patient, the indication for surgery was based on the suspicion of an infected collection that was not amenable to drainage by interventional radiology. The infection was confirmed later with a positive culture for C. albicans of the peripancreatic fluid and pancreatic tissue.
In 1987, Synn et al. 7 reported an incidence of open surgery in 38% in pediatric patients with AP, the indications being drainage of collections, debridement of pancreatic necrosis, drainage of pseudocysts, and pancreatectomy. To the best of our knowledge, this is the first case of a laparoscopic pancreatic necrosectomy and drainage of collections performed in a pediatric patient with severe AP. Previously, there has been reports of laparoscopic interventions in children with idiopathic and trauma-associated AP.8–12 In 2006, Seitz reported the laparoscopic drainage of a pancreatic pseudocyst with a cystojejunostomy in a child with traumatic pancreatitis. 12 Also, cystogastrostomy is feasible in children, as reported by Saad et al. in 2 cases in which complete drainage of pseudocysts was achieved. 8
In adults, the outcome using a laparoscopic approach to perform drainage of infected collections and debridement of pancreatic necrosis is similar to open surgery, with equal incidence of complications. The success rate after the first laparoscopic drainage is approximately 75%. 10 The smaller size of pediatric patients is the main concern with the endoscopic approach, as the procedure can be technically demanding. Laparoscopic necrosectomy is highly efficient, with a shorter operative time, minimal complications, and low mortality when compared with open necrosectomy. 11
Acute biliary pancreatitis in childhood, although rare, is a good example of a disease that benefits from minimally invasive surgery. Recent reports show the possibility of simultaneously combining laparoscopic and endoscopic procedures (ERCP and laparoscopic cholecystectomy). The effectiveness in terms of stone clearance is about 97%–100%. 13 Alternatively, performing a transcystic exploration and clearance of the CBD at the time of cholecystectomy is safer, considering the increased risks of AP, bleeding, papillary stenosis, and sclerosing cholangitis associated with ERCP and papillotomy in children. In a report of 13 cases, two-thirds were managed only with transcystic exploration and led to good results; in a follow-up period of 28 months, all patients were symptom free. 14
Most of the knowledge of AP in children has been extrapolated from the adult population, especially regarding the severity, outcome, and management of this condition. 15 As laparoscopic intervention has been highly effective in the management of this problem in adults, one would expect that similar outcomes can be achieved in children. Unfortunately, because of the very small number of children needing this intervention in any individual pediatric institution, a large multicenter cooperative study will need to be done to substantiate this sentiment.
In conclusion, the present case report helps to illustrate the current surgical management of AP in children. Minimally invasive surgery can play a role in resolving the complications and etiology of AP in childhood.
Footnotes
Acknowledgment
The authors thank Dr. Albert Shun, from the Royal Alexandra Hospital for Children, Westmead, Australia, for his help in preparing and reviewing this manuscript.
Disclosure Statement
No competing financial interests exist.