
Abstract
Abstract
Chronic obstructive lung disease (COPD) is a high-risk factor for pulmonary complications in esophageal surgery. We reported a case of esophageal gastrointestinal stromal tumor (GIST) in a patient with severe COPD. Upper gastrointestinal endoscopy and computed tomography revealed a 3×2-cm submucosal tumor at the lower esophagus, and positron emission tomography showed a hypermetabolic mass (SUVmax=5.6). Forced expiratory volume in 1 second (FEV1) was 33.0% of predicted and FEV1/forced vital capacity ratio was 40.7%. Taking the patient's lung function into account, we performed a thoracoscopic enucleation for the esophageal GIST while the patient was in a prone position. The postoperative course was uneventful and no significant change was observed in the patient's respiratory condition. Performing thoracoscopic surgery on COPD patients in a prone position is a good therapeutic alternative for reducing the occurrence of pulmonary complications.
Introduction
Chronic obstructive lung disease (COPD) is a high-risk factor for major pulmonary complications in transthoracic surgery, and patients with severe COPD (forced expiratory volume in 1 second [FEV1] <50% of predicted) develop more postoperative pulmonary complications than those with moderate or mild COPD.5,6 Therefore, treatment of esophageal GIST in patients with severe COPD must be selected very carefully.
In recent years, thoracoscopic enucleation of the esophageal submucosal tumor has attracted attention as an alternative to conventional enucleation by thoracotomy.7,8 Thoracoscopic enucleation is less invasive, leaves a smaller incision, and reduces the postoperative rate of pulmonary complications. 9 However, in several institutions, performing thoracoscopic surgery on patients in the prone position has been adopted. Yatabe et al. 10 showed that using a prone-position approach provided better oxygenation to patients and reduced the development of pneumonia compared with a lateral decubitus position.
Herein, we report on a patient with severe COPD who developed esophageal GIST. The GIST was enucleated through right thoracoscopic surgery with the patient in a prone position to avoid pulmonary complications.
Case Report
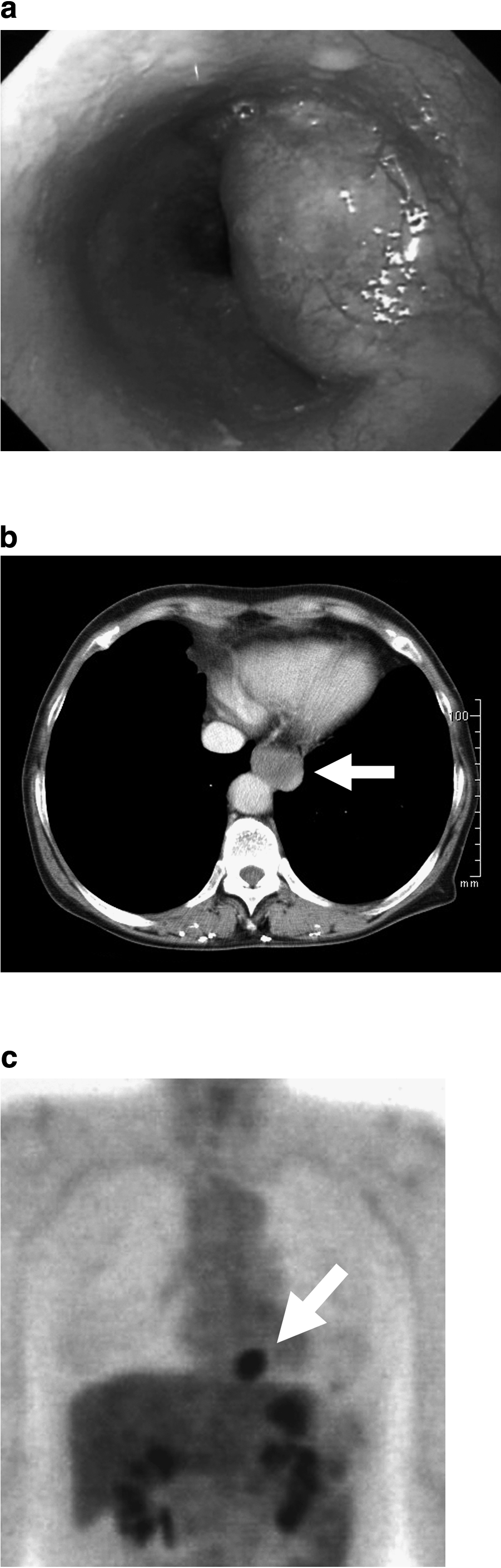
A 67-year-old woman underwent upper gastrointestinal endoscopy as part of a general examination, revealing a submucosal tumor at the right wall of the lower esophagus. On endo-ultrasonography (EUS), a slightly hypoechoic tumor arising from the muscle layer was seen (Fig. 1a). The tumor measured about 3×2 cm on computed tomography (CT) and was hypermatabolic, with the maximum standardized uptake value (SUVmax) of 5.6 on positron emission tomography (PET) scan (Fig. 1b, c). The lesion was diagnosed as GIST, and was considered suitable for resection in accordance with GIST guidelines. 11
The patient had suffered from severe asthma for 30 years and was treated with several medications, including corticosteroid. The severity of her lung function was stage III according to the Global Initiative for COPD criteria 12 (i.e., FEV1 [% predicted], 33.0%; FEV1/forced vital capacity [FVC] ratio, 40.7%).
Operative Procedure
Considering this patient's lung function, thoracoscopic enucleation was determined to be the best surgical option.
Anesthesia was given using a double-lumen endotracheal tube for single-lung ventilation. The patient was placed in the prone position. Her right arm was raised cranially and her face was turned to the right. An operator, assistant, and camera assistant stood at the right side of the patient's chest, and a video monitor was set up on her left side. A 12-mm trocar was carefully inserted into the 5th intercostal space (ICS) on the posterior axillary line using an open technique to confirm the absence of pleural adhesion. Another 3 trocars were inserted thoracoscopically: a 5-mm trocar in the 7th ICS on the scapular angle line, a 5-mm trocar in the 7th ICS on the posterior axillary line, and a 12-mm trocar in the 9th ICS on the scapular angle line for the flexible thoracoscope (Fig. 2). Carbon dioxide pneumothorax was induced at a pressure of 5 mmHg to collapse the right lung.

Right thoracoscopic surgery in prone position. Placement of surgical ports.
The tumor was not recognized initially, as it was located behind the descending aorta. After the mediastinal pleura was incised longitudinally using a bipolar scissors, the tumor, which covered the musculature of the esophagus, became visible. The muscle on the summit of the tumor was split longitudinally and the tumor was then identified by its smooth surface (Fig. 3). The tumor was then separated from the musculature of the esophagus. After cauterizing some blood vessels on the tumor, it was enucleated without mucosal injury. After enucleating, the muscle layer was approximated with a few interrupted 3-0 absorbable stitches intracorporeally to avoid mucosal bulging that might produce a pseudodiverticulum.
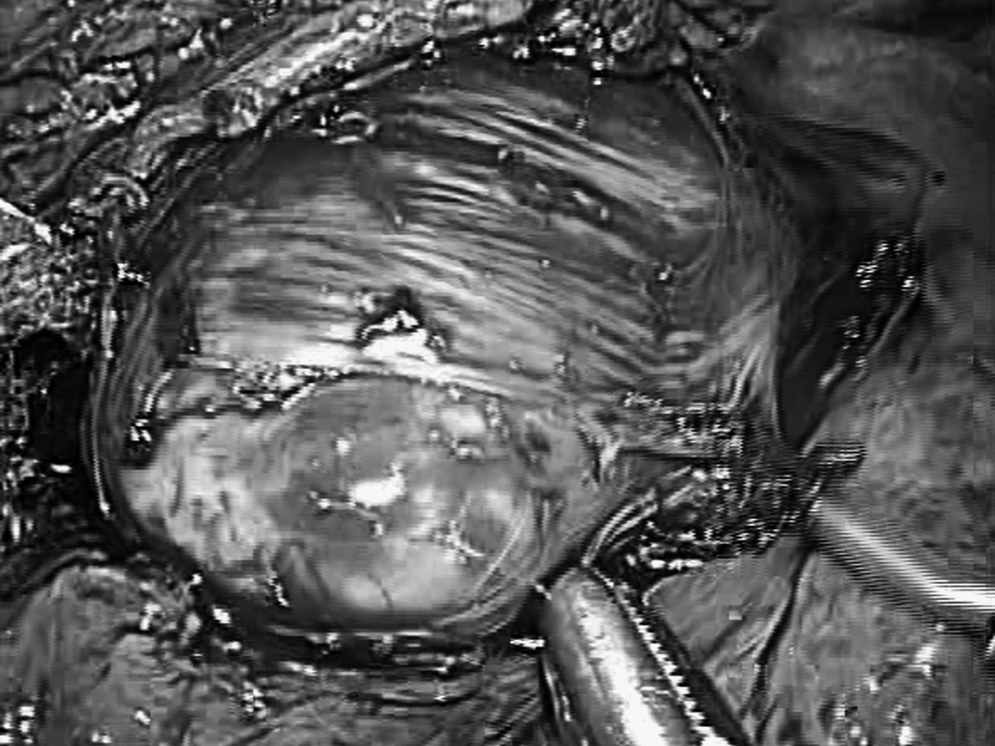
Esophagus muscle was split by bipolar scissors longitudinally and smooth surface of tumor was identified.
The specimen was placed in an endobag and retrieved through the 5th ICS trocar site. A single 20F chest tube was inserted through the 9th ICS trocar site.
Total operative time was 152 min and blood loss was estimated at <10 mL. Intraoperative respiratory condition was almost even, and arterial oxygen saturation and end-tidal carbon dioxide were 94%–98% and 29–40 mmHg under FiO2 of 0.5, respectively.
Postoperative Course
Immediately after the operation, an endoscopic examination was performed and confirmed no mucosal injury. Although abundant sputum was secreted, extubation was performed after establishing steady spontaneous respiration. Temporarily tachypnea developed after extubation, but the patient's respiratory condition stabilized after several minutes and wheezing was not audible. She was able to discharge expectoration firmly by herself. Blood gas analyses revealed that the partial pressure of oxygen and carbon dioxide was 113.0 and 39.4 mmHg, respectively, under oxygen inhalation.
The postoperative course was uneventful. Ambulation was started on postoperative day 1; oral intake was recommenced and the chest tube was removed on postoperative day 2. The patient was discharged from hospital on postoperative day 10. Neither dyspnea nor asthma attack was encountered.
The submucosal tumor was immunohistochemically confirmed as GIST. Mitotic count for the tumor was below 5/50 high-power fields; thus, the patient was placed in the low-risk category.
Discussion
GIST is the most common mesenchymal tumor of the gastrointestinal tract; however, GIST arising from the esophagus is rare. Several clinicopathological studies have evaluated the prognostic factors in patients with gastric GIST13,14; however, less is known about esophageal GIST. Although resection of GIST of the stomach with clear margins is recommended, 11 the treatment options for esophageal GIST are fairly controversial due to the high mortality rate of esophagectomies.3,4 On the other hand, the disease-modulating drug imatinib mesylate, a selective tyrosine kinase inhibitor, has provided a new approach in the treatment of GIST. 15 Imatinib mesylate inhibits KIT phosphorylation and tumor cell proliferation in GIST. Further, Sunitinib malate, another tyrosine kinase inhibitor, has been approved for the treatment of patients with imatinib mesylate-resistant GIST. 16 Therefore, currently, we have many different treatment options to choose from.
After esophagectomy, pulmonary complications are the most frequent type of complications, with a reported incidence ranging from 20% to 35%.17,18 These complications can bring prolonged hospital stay, increased cost, and a substantial operative mortality. COPD is significantly associated with the risk of pulmonary complications. Jiao et al. 6 reported that 33.7% of patients with COPD had pulmonary complications, whereas 13.2% of those without COPD and 67% of severe COPD patients developed pulmonary complications after transthoracic esophagectomy. Further, postoperative respiratory hypofunction can affect COPD patients' quality of life. Ikeguchi et al. 19 reported that the average values of vital capacity, FVC, and FEV1 were 78%, 78%, and 72% of preoperative average values, respectively, at 6 months after transthoracic esophagectomy. Therefore, operative procedures for esophageal GIST in COPD patients must be carefully chosen so as to avoid intra- and postoperative complications. Several authors agree that extended surgery could increase the intra- and postoperative morbidity and mortality rates, as negative macroscopic margins often require excessively invasive procedures.20,21 Enucleation may be a valid option for esophageal GIST for those patients with severe COPD who might develop pulmonary complications. In 2007, the National Comprehensive Cancer Network introduced a set of criteria that ultimately established negative microscopic margins as the key objective in surgical treatment. 22 Further, DeMatteo et al., 2 reporting on 200 GIST patients, did not find microscopic-margin status to be a predictor of survival and suggested that recurrence was due more to the biological behavior of the tumor itself. Nevertheless, the efficacy of enucleation for esophageal GIST has not yet been proven.
In recent years, thoracoscopic surgery has increasingly become the treatment of choice for esophageal disease, as it improves the patient's quality of life in the early postoperative phase. It has been documented that thoracoscopic procedures also reduce invasiveness, resulting in reduced operative blood loss, fewer pulmonary complications, and preservation of vital respiratory capacity.23,24 However, when a patient is in the left lateral decubitus position, causing the mediastinal organs and structures to shift to the left and the right lung to cover the esophagus, it is difficult to achieve operative exposure in a thoracoscopic procedure. Therefore, for a good operative view in the left lateral decubitus position, the right lung must be excluded by forceps. Further, the ventilation lung is then pressed by the mediastinum and the nonventilated lung, leading to atelectasis. On the other hand, in a prone position, mediastinal organs and structures are spontaneously exposed by both gravity and artificial pneumothorax without any manipulation to the lung. Minimal manipulation of the right lung could lessen the impairment of lung function and may be beneficial in preventing pulmonary complications. Matthews et al. 25 reported that the prone position does not negatively affect respiratory mechanics and improves lung volume. Kim et al. 26 reported that the functional residual capacity and ventilation/perfusion matching in the prone position were satisfactory. Thus, a prone position may help to maintain intraoperative oxygenation and lung function.
Miettinen et al. 27 reported that 71% of esophageal mesenchymal tumors were leiomyoma and 17% were GIST. Diagnosis of esophageal submucosal tumor can be made by endoscopy, CT scan, and EUS, but a specific diagnosis of GIST before surgery is quite difficult. Ultrasonically guided fine-needle aspiration (FNA) biopsy may be helpful for diagnosis 28 ; however, there is a risk of hemorrhage and increased tumor dissemination. In fact, it is impossible to assess the mitotic index from a small specimen. Further, FNA biopsy obscures the dividing line of dissection between the tumor and the overlying mucosa and increase the risk of intraoperative mucosal injury. Markedly increased 18 F-fluorodeoxyglucose (FDG) uptake in GIST has been documented in several studies.15,29 Kamiyama et al. 30 reported that the sensitivity of GIST by FDG-PET was 100%. Several reports have suggested that the degree of FDG uptake is a useful indicator of the GIST risk category.31,32 Yamada et al. 32 showed that the cut-off values of FDG SUV in gastric GIST were 2.2, 4.2, and 6.5 for the very low-, low-, intermediate-, and high-risk groups, respectively. However, SUVmax of our case was 5.6, which is in the low-risk category. The relationship between FDG uptake and risk category in esophageal GIST may differ from that of gastric GIST.
Conclusion
Some authors report good results with more conservative procedures such as enucleation7,33; however, as there are no sufficient reports regarding the natural course of esophageal GIST, no definitive treatment recommendations have been made. When determining the operative procedure for patients with severe COPD, intra- and postoperative pulmonary complications should be considered. We concluded that thoracoscopic enucleation in a prone position would be most appropriate for these patients in light of potential complications and quality of life. On the other hand, the administration of imanitib mesylate dramatically improves prognosis of GIST. Therefore, a prospective clinical study focusing on the outcomes of esophageal GIST following different surgical and pharmacological treatments is required.
Footnotes
Disclosure Statement
No competing financial interests exist.