
Abstract
Abstract
Traumatic abdominal wall hernia in children with intact skin is rare. This type of hernia is caused by blunt trauma abdomen that does not penetrate the skin. These hernias have been repaired in adults by open repair. We report the first laparoscopic repair of this condition in a 2-year-old child with blunt abdominal trauma in emergent settings.
Introduction
Case History
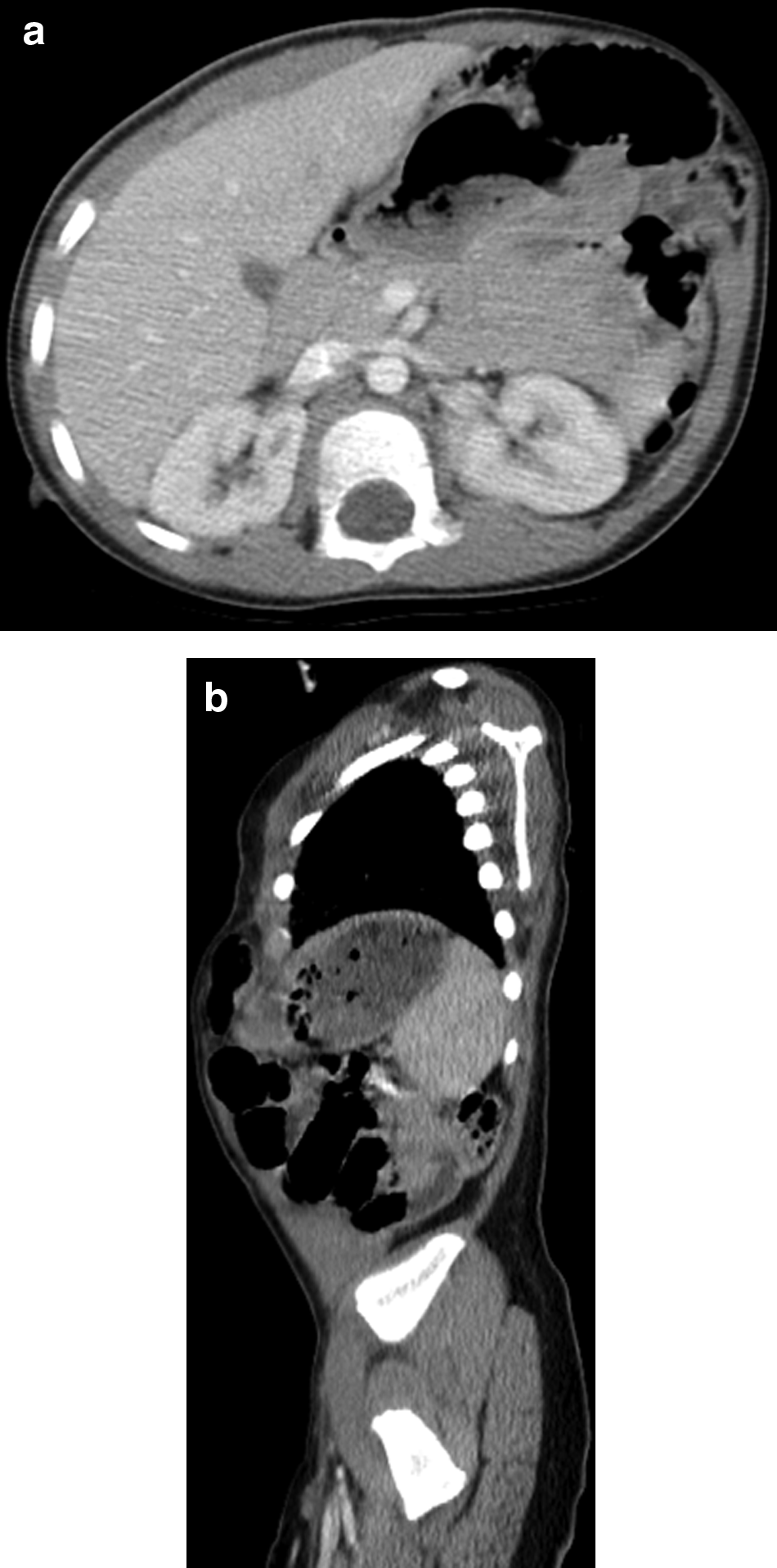
A 2-year-old boy with no previous medical history presented to the emergency room of our hospital after having been accidentally hit by his grandmother's car. He arrived hemodynamically stable with a Glasgow coma scale (GCS) of 12. On physical examination, the patient was found to have a right humeral fracture as well as abrasions that covered about 60%–70% of his abdomen. On the left side, there was palpable bowel just underneath the skin. Computed tomography (CT) imaging revealed a traumatic left anterior abdominal wall hernia that appeared to contain both small bowel and transverse colon (Fig. 1a, b). In addition, there was dilatation of proximal small bowel, suggestive of mechanical obstruction by the hernia. No gross intra-abdominal free air was noted. CT scan showed free fluid in the pelvis with no solid organ injury and some bowel wall enhancement that was suspicious for bowel injury; hence, the patient was taken for immediate exploratory laparoscopy. During surgery, a 7–10 cm defect in the abdominal wall was found extending from near the midline to the left flank. Laparoscopic exploration did not reveal any significant bowel injury or any other injury. We laparoscopically repaired the abdominal wall hernia by the technique described next.
Procedure
The patient was taken to the operating room, intubated, and anesthetized. A 5 mm incision was made in the scar of the umbilicus, and a 5 mm Step expandable port was introduced into the peritoneal cavity by using a modified Hasson's technique. Pneumoperitoneum was then achieved with CO2 of 5 L/minute with a pressure of 12 mm Hg. Once adequate pneumoperitoneum had been achieved, a 5 mm 30-degree laparoscope was introduced into the peritoneal cavity. A 2 mm stab incision was then made on the right flank, and a grasper/needle holder was directly introduced without ports. On inspection, there was a traumatic left-sided abdominal wall defect with a hernia (Fig. 2). The omentum and bowel were seen to have herniated through the defect. Once the herniated bowel had been gently reduced and pulled down, the full extent of the defect was revealed. No other abnormalities were seen.
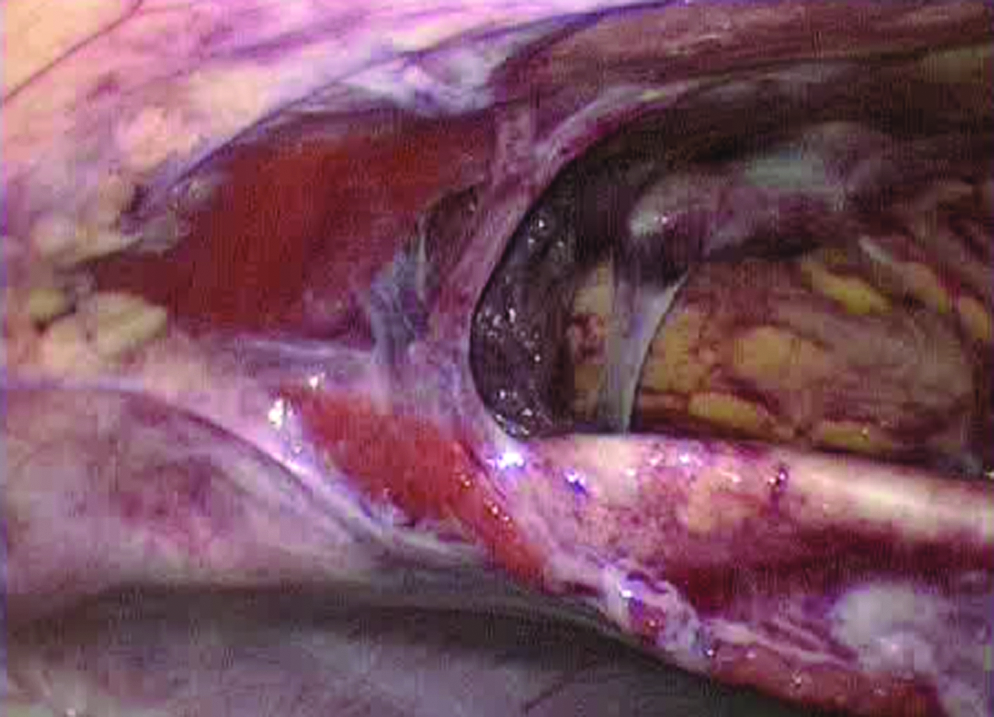
Hernia after contents reduced.
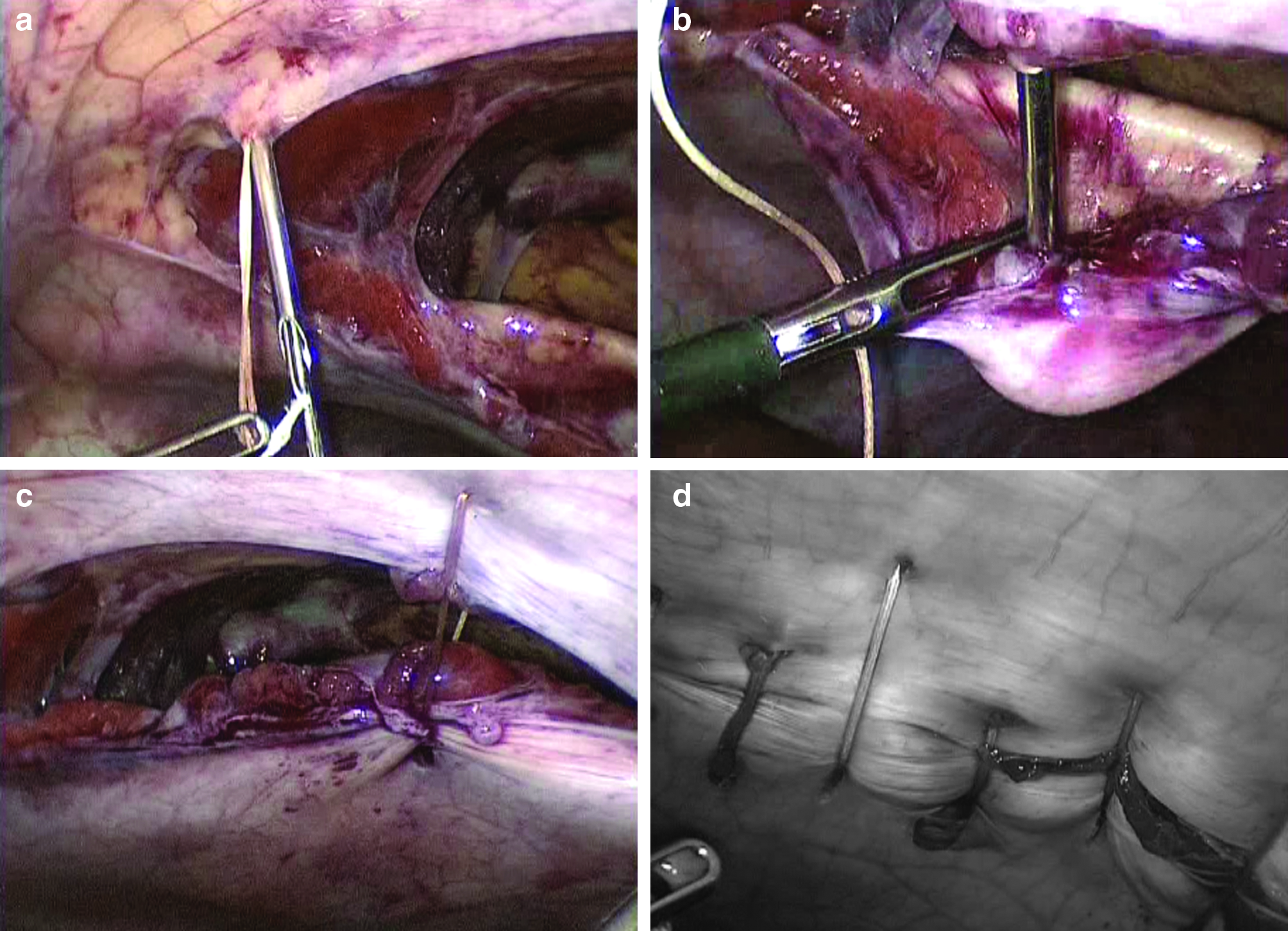
After exploratory laparoscopy had been completed, repair of the defect was started. A GraNee needle (R-Med, Inc., Oregon, OH) was used to place several sutures through the abdominal wall hernia defect (Fig. 3a–c). Using the GraNee needle technique, the two ends of the defect were brought together with subcutaneous sutures. Approximately 10–12, 2-0 Vicryl sutures were placed in total, which took about an hour (Fig. 3d).
Once the repair had been completed, the instruments were withdrawn under vision. The umbilical port was withdrawn after desufflation of the peritoneal cavity. The umbilical fascia was closed with 2-0 Vicryl on a UR6. A single suture was used. The wounds were irrigated with saline, and the port sites were closed with Dermabond glue. The abdominal wall was then covered with Vaseline gauze as a dressing. The patient tolerated the procedure well and was extubated.
Results
After the procedure, the patient did well and was discharged on postoperative day 5. At 1 and 6 months follow-up, he was in good condition, with the scars well healed and no evidence of recurrence (Fig. 4).

Excellent cosmetic results at follow-up.
Discussion
We report the first case of successful laparoscopic repair of a traumatic abdominal wall hernia in a pediatric patient. Additionally, this repair was done in an acute setting (in conjunction with an exploratory laparoscopy), which has not previously been described in a child. Subcutaneous herniation of intestinal contents after non-penetrating blunt abdominal wall trauma is most commonly reported after bicycle handlebar injuries or another severe blunt-force injury.1,4 Our patient developed a subcutaneous intestinal hernia after blunt abdominal trauma sustained after being struck by a car, but he did not suffer any visceral injury. Due to the nature of the trauma, impressive physical exam, and suspicion of bowel trauma on imaging, we were compelled to perform an exploratory surgery to visualize the suspected internal bowel injury. We decided that it would be best to perform herniorraphy at the same time as the exploration. Given the age of our patient, mesh was not considered appropriate. This approach allowed us to perform a one-step operation on the day of admission, at which point all significant internal injury was ruled out, and the traumatic abdominal wall hernia was repaired. This gave our patient the best chance for quick and complete recovery, unlike delayed approaches used in the past. The laparoscopic approach also conferred significant benefit to the patient by both decreasing hospital stay and delivering cosmetic benefit, as was noted in previous case reports in adults.2,3 We believe that this method of immediate laparoscopic repair is one that can be considered with confidence in patients with a similar type of abdominal wall injury.
Footnotes
Disclosure Statement
No competing financial interests exist.