
Abstract
Abstract
Introduction:
The single-incision laparoscopic approach may be suitable for several intra-abdominal surgical interventions, but its usefulness for treating gastric cancer has not been established. The aim of this study is to compare the perioperative outcomes of single-incision laparoscopic distal gastrectomy (SIDG) and conventional laparoscopic distal gastrectomy (LDG) by using a porcine model.
Methods:
Ten pigs were used to compare the perioperative outcomes of SIDG and LDG. All were subjected to the same distal gastrectomy with D1+β lymph node dissection method. Specimens retrieved during the operation were subjected to manual lymph node picking and counting. To evaluate the inflammatory reactions, white blood cell (WBC) counts and C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor (TNF)-α levels were measured before and 1 hour, 1 day, and 5 days after surgery. The pigs were sacrificed 1 week after surgery.
Results:
The procedures were successfully performed in all pigs. The SIDG group lost more weight than the LDG group, but this was not statistically significant (3.34±2.36 kg versus 1.94±1.61 kg, P=.305). The SIDG group was associated with a significantly longer operation time (140±14.14 minutes versus 93±4.47 minutes, P<.001), but it had a similar mean number of resected lymph nodes (25±2.45 versus 22±4.87, P=.393). Variance analysis failed to detect significant WBC, CRP, IL-6, or TNF-α differences. At sacrifice, one pig from each group exhibited anastomosis narrowing.
Conclusions:
This animal study shows that SIDG can be applicable for treating gastric cancer with similar inflammatory reaction and complication rates when compared with LDG. Comparative human study is necessary to demonstrate the benefits of SIDG compared with standard laparoscopic surgery.
Introduction
Single-port transumbilical laparoscopic surgery offers better cosmetic results, less incisional pain, and the possibility of conversion to multiport surgery if required.4–6 The recent advances in laparoscopic instruments and skills have resulted in the single-incision laparoscopic approach being proposed for several intra-abdominal surgical interventions such as appendectomy, cholecystectomy, and adrenalectomy.7–9 However, at present, it is not known whether single port laparoscopic surgery can be used to treat malignant disease; in particular, it is unclear whether it compromises oncologic principles and would reduce morbidity, although its cosmetic benefit is clear.
In the current study, we used a porcine survival model to determine the feasibility of single-incision laparoscopic distal gastrectomy (SIDG) for gastric cancer in terms of surgical outcomes; for this, it was compared with laparoscopic distal gastrectomy (LDG).
Materials and Methods
The study was approved by the Animal Care and Use Committee of the Seoul National University Bundang hospital. Fifteen pigs weighing 30 to 36 kg were used. Five pigs were used for practicing the SIDG procedure. Ten pigs were used to compare the peri- and postoperative outcomes of SIDG and LDG. The animals were quarantined and allowed to acclimate in the animal facility for a minimum of 1 week before surgery. Before surgery, all pigs were fasted for 24 hours, and their weight was measured. Under general anesthesia maintained by 2% Enflurane, SIDG and LDG were performed along with D1+β lymphadectomy (D1 plus No. 7, 8a, 9 and 12a) (n=5 per group). Lymph node dissection was performed based on the Guidelines of the Japan Gastric Cancer Association. 10 As prophylaxis against infection, cefazolin 0.3 mg/kg was intravenously injected just before the procedure. Antibiotic treatment was not continued after the operation. The ten pigs in the comparative study all resumed sipping water immediately after surgery. All of them also started to eat a soft diet composed of commercial products on postoperative day 2 and progressed to a normal diet on postoperative day 3.
Operative methods
For the SIDG procedure, a longitudinal 2 cm-long transumbilical skin incision was made. A commercial three-lumen single-port trocar (OCTO™, Dalim surgent, Seoul, Korea) was then placed, and the abdominal cavity was insufflated with carbon dioxide at a pressure of 12 mm Hg. The OCTO trocar system consists of a self-retractor that covers a 10–50-mm incision and a detachable port cap that contains one, three, or four channels of various diameters along with one insufflation and one smoke exhaust valves. We used the three-port system that has two 12-mm and one 5-mm channels. A 2-mm trocar was introduced into the peritoneal cavity in the left subcostal area to provide counter-traction during dissection. This was followed by the insertion of a 5-mm version rigid videoscope with 30° directional view (EndoEye camera system; Olympus Medial Systems Corp., Tokyo, Japan). Prototype curved instruments (Olympus Medical Systems Corp.) and a Harmonic Scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH) were used to facilitate dissection (Fig. 1).
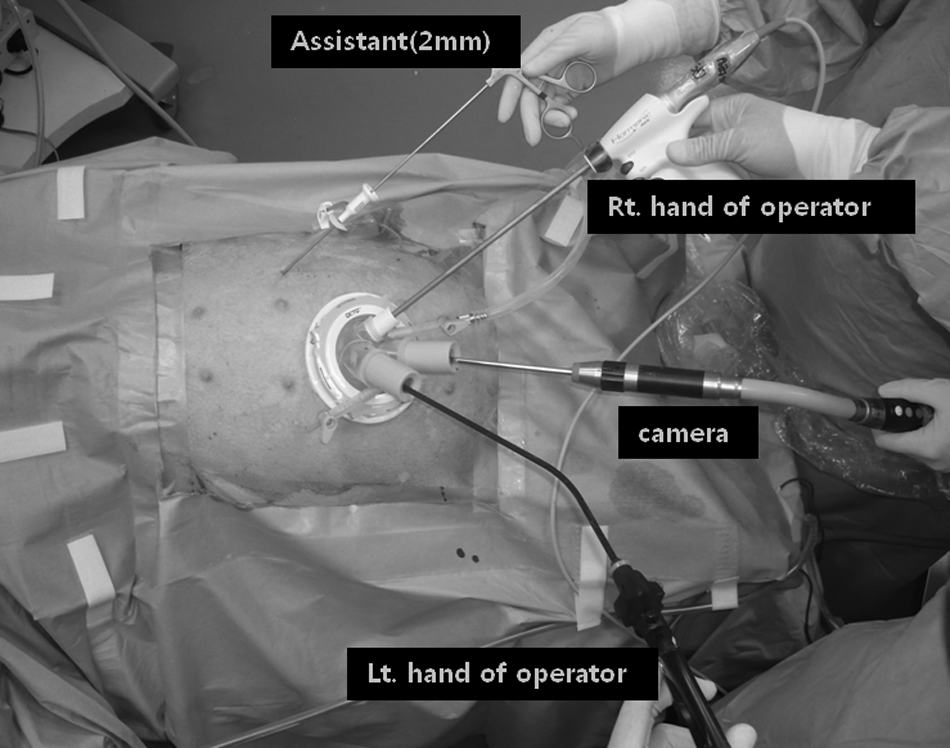
Position of the surgeons and the instruments. The operator is using prototype curved instruments (Olympus Medical systems Corp.) in the left hand and a Harmonic scalpel (Ethicon Endo-Surgery, Inc.) in the right hand. The camera operator is located between the right and left hands of the operator. Rt., right; Lt., left.
The procedure commenced with the division of the omentum 3 to 4 cm from the gastroepiploic arcade, which includes lymph node 4d. Since the common bile duct of the pig enters the distal antrum of the stomach, the right gastroepiploic artery was saved at the root, and lymph node 6 dissection was continued along this vessel to save the common bile duct and maintain the blood supply of the distal antrum. The right gastric artery and the proper hepatic artery were exposed to dissect lymph nodes 5 and 12a, and the right gastric artery was then divided at its origin. The distal antrum was divided at just the proximal of the site where the common bile duct inserts into the antrum. Lymph nodes 8a and 9 were dissected along each artery. The left gastric artery and vein were exposed and individually divided to allow dissection of the No. 7 lymph nodes. Lymph nodes 1 and 3 were dissected, and the upper third of the lesser curvature was skeletonized. The stomach was transected by using linear staplers.
For intracorporeal anastomosis, we used endoscopic flexible linear staplers (Echelon flex60–3.5 and 4.5; Ethicon Endo-Surgery). To make a side-to-side anastomosis, a small incision was made on the greater curvature of the stapled line of the stomach and the antimesenteric side of the duodenum, 6–7 cm from the stump. After step-by-step insertion of the linear stapler forks, the posterior wall of the stomach and the antimesenteric side of the duodenum were put together, and an anastomosis was made with the linear stapler. The common incision was closed with one or two additional staples. Specimens were retrieved through the umbilical port site.
For the LDG procedure, five trocars were used. Intracorporeal anastomosis and D2 minus 14v lymph node dissection were performed as just described. Specimens were retrieved after extension of the umbilical incision by 2 or 3 cm.
To evaluate the adequacy of lymphadenectomy, the specimens retrieved during the operations were subjected to manual lymph node picking and counting.
Comparison of the inflammatory reactions associated with SIDG and LDG
To compare the inflammatory reaction induced by each operation, white blood cell (WBC) counts and C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) levels were measured before surgery and 1 hour, 1 day, and 5 days after surgery. To measure the cytokine levels, porcine serum was prepared by centrifuging clotted blood for 10 minutes at 3000 rpm; the serum was then stored in aliquots at −80°C. After collecting all specimens required for experimentation, TNF-α and IL-6 were quantitatively measured by the ELISA method [R&D Systems (Quantikine), Minneapolis, MN], and CRP was quantitatively measured by the immuno-nephelometry. The colored product formed at the end of the assays was measured according to the manufacturer's instructions, and the concentrations of TNF-α and IL-6 in the test samples were determined from their standard curves. Interassay precision was ensured by testing two samples of each serum specimen that had been collected.
Necropsy
All ten comparative study pigs were kept alive for 1 week and then sacrificed. The weights of the pigs were assessed at this stage. A midline laparotomy was performed, and the extent of adhesion, anastomosis leakage or stricture, and other complications were assessed (Fig. 2).
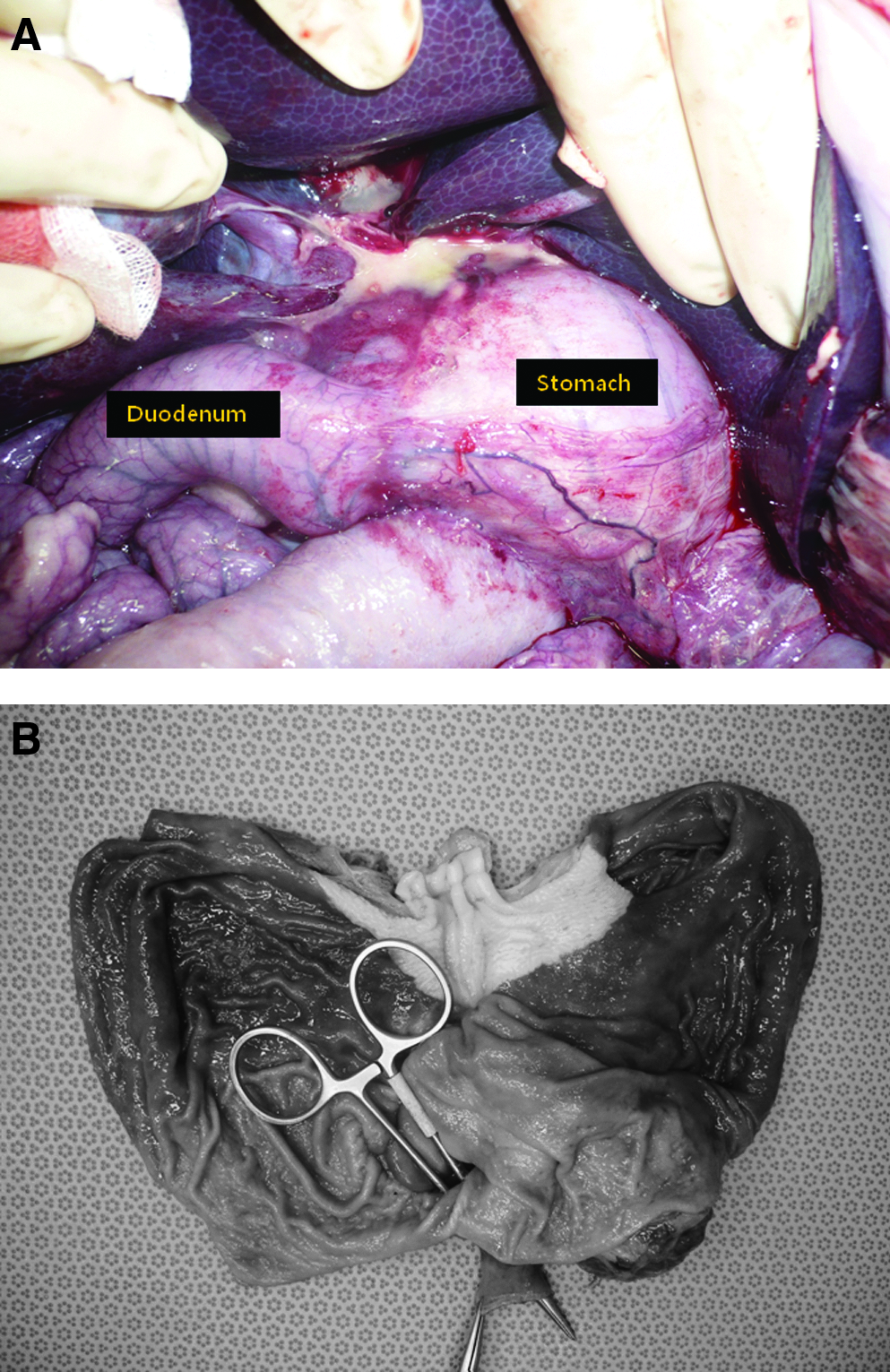
Necropsy.
Statistical analysis
Statistical analyses were performed by using SPSS version 15.0 (SPSS Inc., Chicago, Illinois). WBC counts and CRP, TNF-α, and IL-6 levels were expressed as means±standard error of the mean. Independent Student's t-test was used to compare the two groups. Repeated measures ANOVA test was used to compare changes in inflammatory indicators between the two groups.
Results
The procedure was successfully performed in all 10 pigs without intraoperative complications. The perioperative outcomes are shown in Table 1. All pigs lost weight. Although the SIDG group lost more weight than the LDG group, this difference did not achieve statistical significance. The SIDG group was associated with a significantly longer operation time, but the mean number of resected lymph nodes did not differ significantly. There was no mortality. At sacrifice, one pig from each group exhibited an anastomosis narrowing. Apart from the TNF-α levels on postoperative day 5, the two groups did not differ significantly in terms of mean WBC counts or TNF-α, IL-6, and CRP levels, regardless of when the measurements had been performed (Table 2). Moreover, variance analysis of the WBC count and CRP, IL-6, and TNF-α level means over time failed to detect statistically significant differences between the two groups (Fig. 3).
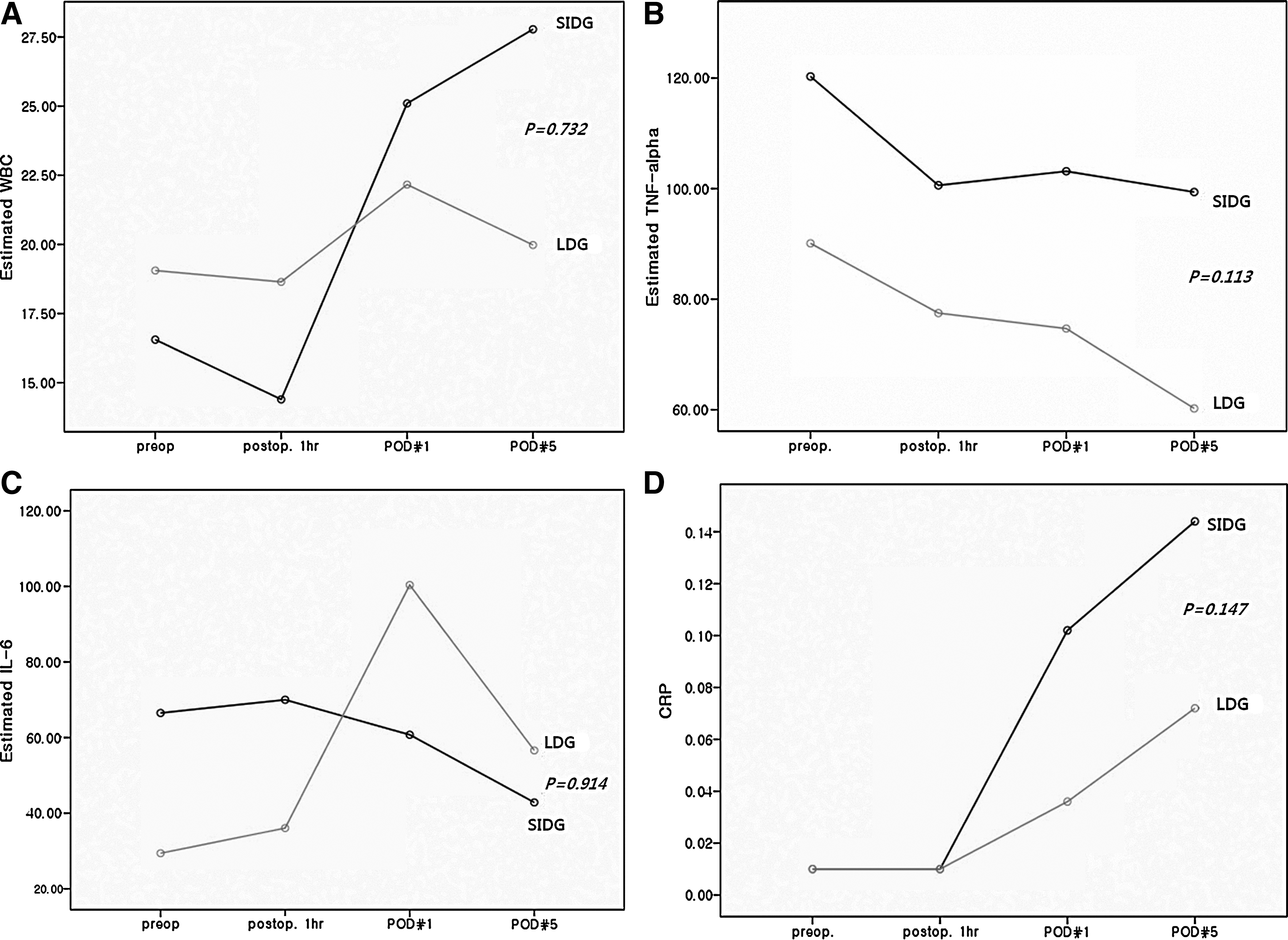
The SIDG and laparoscopic distal gastrectomy (LDG) groups do not differ significantly in terms of the variance of postoperative inflammatory responses.
LDG, laparoscopic distal gastrectomy; LN, lymph nodes; SD, standard deviation; SIDG, single-incision laparoscopic distal gastrectomy.
CRP, C-reactive protein; IL, interleukin; SD, standard deviation; TNF, tumor necrosis factor; WBC, white blood cell.
Discussion
The development of NOTES worldwide is progressing very quickly, but the advantages of this approach over laparoscopic surgery have not yet been identified. There are also some limitations that have to be overcome. These include the requirement for specialized instruments, the spillage of bowel contents during entrance via the stomach or colon, and the potential risk of leakage after difficult repairs of the visceral lumen. 11 A recently proposed surgical approach that shares the basic concept of NOTES is single-port trans-umbilical laparoscopic surgery, which has the advantage that existing laparoscopic instruments can be used, and viscerotomy is not needed. Moreover, additional trocars can be included if needed. These advantages have meant that single-incision laparoscopic surgery is gaining popularity in general surgery as a complement to standard laparoscopic surgery and as a safe alternative to NOTES. Recently, several authors reported the clinical application of this procedure to colorectal and gastric cancer, with adequate lymph node extraction.12–14 However, it still remains unclear whether this procedure can also be used to treat gastric cancer and how its outcomes can be compared with those of standard laparoscopy. To address these issues, the current animal study was performed before clinical application.
We found that the SIDG procedure was associated with a few practical limitations. In particular, major problems encountered early in the learning curve associated with this procedure were external crowding and the clashing of instruments. We used a 5-mm rigid EndoEye camera system (Olympus Medical) with a 30° view. The advantage of this camera system is its streamlined light cable (as opposed to the standard laparoscopic light cable, which enters the lens at 90°). This limits camera bulkiness and, thus, minimizes extracorporeal clashing. The use of curved instruments with differential overall lengths was also helpful. A prototype curved instrument (Olympus Medical) was operated by the left hand of the operator. This minimized both external clashing and internal conflicts. However, despite the recent introduction of bent and flexible instruments, clashing is still a major issue. Motorized instruments may solve this problem. Flexible multichannel robotic systems and intracorporeal mobile devices such as a mobile internal camera are likely to be developed soon. Once these technologies become widely available, then both single-port surgery and the NOTES procedures will advance even further.
Another limitation of SIDG is that using the umbilicus as the portal of entry limits the candidates who are suitable for this approach. In particular, obese patients with a large abdominal girth are not suitable for SIDG, as the distance to the target organ rises as the degree of adiposity increases. This issue should be considered in the clinical setting. However, obesity is not a contraindication if the operator has accumulated sufficient technical facility and experience and new instruments are developed for these patients.
Another limitation was that we had used an additional assistant 2-mm trocar for retraction. For an advanced procedure such as SIDG, retraction is needed for sufficient exposure of the operative field. Retraction can be achieved by either static intra-abdominal sutures affixed to the parietal peritoneum or percutaneous sutures that are grasped and extracorporeally manipulated to maintain variable traction. Some authors have shown that these techniques are useful for some procedures.15,16 As previously reported, this suture retraction procedure is also useful for exposing the hepatoduodenal ligament, the lesser omentum, and the gastroesophageal junction for purposes of lymph node dissection in the clinical setting. 17 Deployable instruments for retraction, such as magnetic retractors and deployable tissue retractors, may help solve this problem in the future.
The same gastroduodenostomy method was performed in both groups, and there was one case of anastomosis narrowing in each group. In both cases, the stomach was dilated and filled with food even though the animals had fasted for 24 hours before being euthanized; moreover, the patency of the anastomosis at necropsy was reduced to the maximum diameter achieved by just one mosquito clamp. These anastomotic failures were due to the fact that pigs have a narrower duodenum than humans. In the clinical setting, this method would be safely performed. BII gastrojejunostomy18,19 or “Delta-shaped” BI anastomosis 20 may also be an option for intracorporeal anastomosis as totally laparoscopic surgery.
Compared with open surgery, laparoscopic procedures are associated with significantly lower host inflammatory responses, namely TNF-α, IL-1, IL-6, and other inflammatory markers.21–23 However, although the lower degree of trauma induced by single-port transumbilical surgery suggests that this procedure might be associated with lower perioperative inflammatory responses than LDG, we found no significant difference between the SIDG and LDG groups in terms of postoperative inflammatory responses. This may reflect our inexperience with regard to SIDG and the consequent longer operation time. It is also important to recognize that this study had a small sample size and involved an animal model. Larger sample numbers and human study may reveal additional statistical differences between the SIDG and LDG groups.
This study was designed to evaluate the technical feasibility of SIDG for gastric cancer in a pig model. Appropriate lymphadenectomy could be performed during SIDG in this animal model. The two groups did not differ significantly in terms of the number of resected lymph nodes. Although this outcome has been achieved in a pig model and only involves the number of resected lymph nodes, we conclude that SIDG may be useful for treating gastric cancer, albeit in a limited range of indications.
In conclusion, this study shows that the inflammatory reactions associated with SIDG are comparable to those associated with standard five-port LDG. In addition, we demonstrated that SIDG may be a safe procedure without compromising adequate lymphadenectomy that is associated with reasonable complications. Although the cosmetic benefit is apparent, SIDG may require a longer operative time and greater technical expertise than LDG, and the impact of this procedure on perioperative pain is not known. This indicates the need for further validation using randomized control trials in humans.
Footnotes
Acknowledgment
This study was supported by Seoul National University Bundang Hospital (Project no. 03-2009-011).
Disclosure Statement
No competing financial interests exist.