
Abstract
Abstract
Background:
Laparoscopic intracorporeal suturing and knot tying is a complex skill that requires repeated deliberate practice to master. A novel self-anchoring barbed suture material that does not require knot tying can eliminate knot failure and reduce operating time. The goal of this study was to compare the in vivo efficacy of two novel knotless barbed sutures (absorbable and nonabsorbable) for use with the Endo Stitch™ device (Covidien), against conventional suture (Endo Stitch device with Polysorb™ suture; Covidien) for laparoscopic closure of viscerotomies in canine stomach, jejunum, and colon.
Methods:
Following Institutional Animal Care and Use Committee approval, 24 dogs underwent laparoscopic creation of 25-mm viscerotomies, three each in the stomach, jejunum, and colon. All viscerotomies were closed with the Endo Stitch device using the absorbable or nonabsorbable barbed suture or conventional suture. Closure time for each viscerotomy was recorded. Animals were survived for 3, 10, or 21 days, at which point the viscerotomies were burst-pressure tested.
Results:
The closure leak rate in this study with 216 total viscerotomy closures was 0%. There was no statistically significant difference in mean burst pressure between viscerotomies closed with barbed suture versus control suture at any of the survival intervals. Barbed suture with the Endo Stitch device was associated with statistically significantly faster closure times than the control suture with the Endo Stitch device (P<.05), resulting in a reduction in closure time between 35% and 42%.
Conclusion:
This study reports the first use of barbed suture for the Endo Stitch device in laparoscopic gastrointestinal closure. The barbed suture for the Endo Stitch device is effective for laparoscopic single-layer gastrointestinal closure and is associated with a significantly reduced closure time.
Introduction
A novel self-anchoring barbed suture material directly addresses the issues of knot failure and operating time, as it eliminates the need to tie knots. Demyttenaere et al. recently reported the first use of barbed suture in open gastrointestinal closure. In their randomized swine study, the use of the V-Loc™ advanced wound closure device (Covidien, Mansfield, MA) resulted in comparable gastrointestinal closure to 3-0 Maxon™ and significantly faster suturing time. 2 The aim of the present study was to assess two new barbed monofilament sutures for the Endo Stitch™ (Covidien), both an absorbable (polyglyconate) device (AD) and a nonabsorbable (polybutester) device (ND) for laparoscopic gastrointestinal closure, with the following objectives:
1. To compare the in vivo efficacy of the two knotless barbed sutures against conventional absorbable suture for laparoscopic closure of canine enterotomies in the stomach, jejunum, and colon;
2. To compare the relative burst strength of enterotomies closed with barbed monofilament sutures to a control absorbable suture (Polysorb™ suture for the Endo Stitch device) at 3, 10, and 21 days postoperatively;
3. To compare enterotomy closures times with barbed suture versus conventional suture.
Materials and Methods
Institutional Animal Care and Use Committee approval was obtained prior to the commencement of this study. Twenty-four purpose-bred mongrel dogs weighing between 15 and 20 kg were the study subjects. Animals received preoperative oral magnesium citrate at intervals during the 36 hours preceding surgery. Oral intake was withdrawn 12–15 hours preoperatively. Broad-spectrum preoperative antibiotics (ampicillin 1 g IV) were given and a fentanyl patch was placed 24 hours preoperatively and replaced every 72 hours as needed.
Surgical technique
Animals were anesthetized, intubated, and placed in the dorsal recumbent position on a heating pad. Standard antiseptic preparation and draping of the abdomen was undertaken. Access to the peritoneal cavity was gained via open Hasson technique in the right lower lateral abdomen, and a 12-mm port was placed. Following insufflation, laparoscopic exploration was conducted to exclude any access-related visceral injury, and three additional ports (12 mm in right mid-abdomen, 5 mm in right upper abdomen, and another 5-mm port in the left lower lateral abdomen) were placed under direct vision.
A series of 25-mm enterotomies were created in the stomach (1 control, 1 AD, 1 ND), jejunum (1 control, 1 AD, 1 ND), and colon (1 control, 1 AD, 1 ND) for a total of nine enterotomies per animal. The gastrotomies were created transversely, ensuring adequate spacing between them, and spanning the extent of the anterior stomach between the lower esophageal sphincter and pylorus. The jejeunotomies were created parallel to the longitudinal axis of the bowel on the antimesenteric border, with the most proximal enterotomy placed 50 cm distal to the ligament of Treitz (duodenocolic fold) and the remaining two placed distal to this, ensuring a 20 cm spacing between the enterotomies. The colotomies were similarly placed on the antimesenteric border and spaced 5 cm apart. Assignment of treatment and control enterotomy was preoperatively randomized. All enterotomies were closed with the Endo Stitch device in a single-layer, simple-running fashion. Closure of assigned AD and ND enterotomies was initiated with a full-thickness (mucosa out to serosa) bite at the apex of the incision, placing the preformed anchor intraluminally. Several running bites were taken, and the suture line was completed by taking two additional bites beyond the terminal extent of the enterotomy. The suture was then cut flush to the bowel wall without a knot. The control suture line was started and ended with three square knots on both ends. A single surgeon completed all the enterotomy closures and the time taken to completely close each enterotomy was recorded.
The peritoneal cavity was routinely inspected for hemostasis and inadvertent injury. The abdomen was then desufflated, followed by the removal of all ports and closure of port sites in standard fashion. The animals were recovered from anesthesia and extubated.
Postoperative care
Pain control was achieved via a fentanyl patch as previously described. Animals remained NPO (nothing per os) until fully ambulatory. Limited access to water was allowed 6–12 hours postoperatively. A small amount of low-residue food was offered at 12 hours postoperatively and normal diet was introduced and advanced as tolerated over the ensuing 24–36 hours. Indications for early euthanasia included unrelieved pain, failure to eat for >48 hours, weight loss of over 20% at any point during the postoperative period, or uncontrolled infection.
Analysis
Animals were euthanized on postoperative days 3, 10, and 21 and an immediate postmortem examination was conducted via a midline laparotomy. Digital photographs were taken upon entry into the abdomen and of each enterotomy site. Each enterotomy was scored for adhesions using the scoring system shown in Table 1. 2
Burst testing
Pressure measurements were recorded on a laptop computer (19 dogs) with a Preclin 420LP pressure transducer (Samba Sensors AB, Gruvgatan, Sweden) or monitored on an HP Model 66 (Hewlett-Packard, Palo Alto, CA) with Pressure M1006A invasive blood pressure module (5 dogs).
Each enterotomy sample was isolated by clamping on either side of the suture line. An 18-gauge needle was inserted (away from the suture line) into the lumen of the sample to be tested and water colored with green food dye was infused by a syringe pump at 7 mL/min. The pressure transducer was inserted into a Y-connection in the tubing from the syringe pump. Pressure readings and visual observation were used to monitor the sample for leakage. The burst point and failure mode was recorded. Failure could occur from the suture repair site or native tissue or exceed the range of the pressure transducer, in which case no leak was observed.
Results
There were 14, 5, and 5 animals in the day 3, 10, and 21 groups, respectively. More animals were assigned to the day 3 group based on preliminary studies showing that the largest intra- and intergroup variability for burst pressures was seen in day 3 animals, whereas there was very little variation in the burst pressure data after day 10. The samples sizes chosen were based on those data and considered sufficient for demonstrating quantifiable differences between the treatment and control sutures at α=0.05 and β=0.20, should such differences truly exist.
Two of the 24 animals died within the first postoperative day, prior to scheduled euthanasia. Both were from the day 3 group. Necropsy revealed cause of death in both animals to be massive hemoperitoneum, although the exact source of hemorrhage was not found. Portsite hematomas were present, suggesting a possible source of hemorrhage. All enterotomy closures were intact. These animals were not included in the data analysis. There were no other postoperative complications.
Closure time
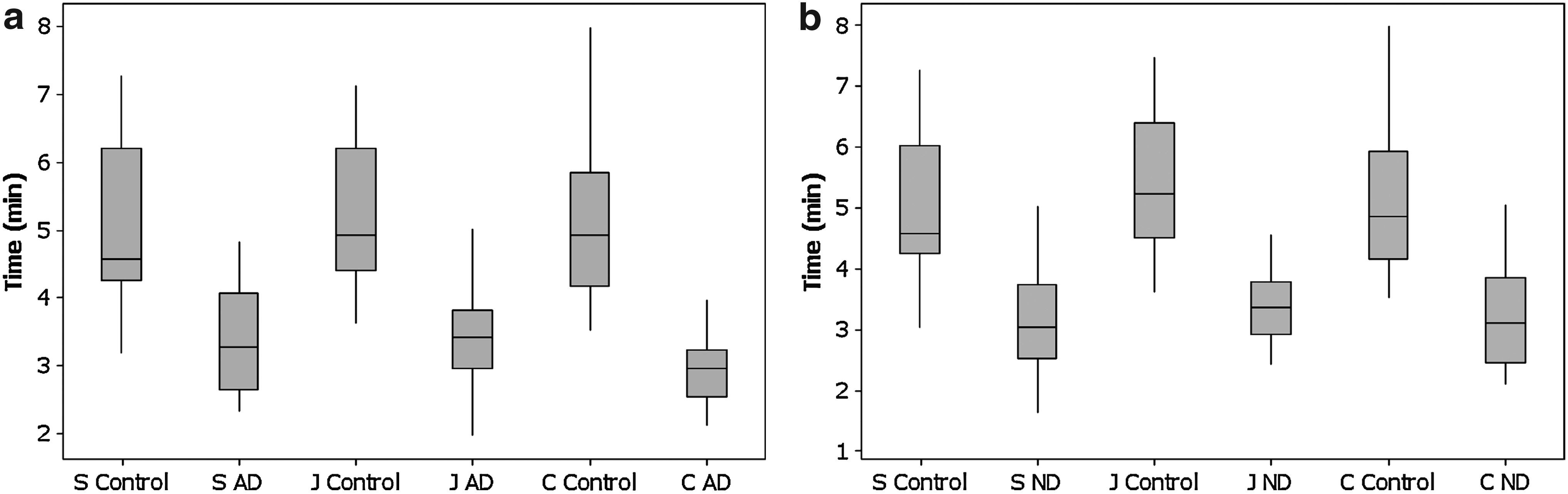
At α=0.05 there was a statistically significant difference in mean closure times between the barbed suture and the conventional, control suture, with the barbed suture being faster. Box plots depicting closure times are shown in Figure 1. The time savings associated with using barbed suture compared with conventional suture ranged from 1:47 to 2:07 (minutes:seconds), which translated to a percent reduction of enterotomy closure time between 35% and 42%.
Adhesions
Adhesions were scored on a scale of 0 to 5, with 0 representing no adhesions and 5 the highest level encountered. The Mann–Whitney test was employed to analyze results. There was no statistically significant difference in adhesion levels between the control suture and either barbed suture. The only exception to this was in the colon on day 10, where the control was associated with a statistically significantly higher median adhesion score.
Burst pressure
Day 3
Stomach: Eight of the 12 burst pressure samples in the control group, 3 of the 12 samples in the AD group, and 5 of the 12 samples in the ND group did not burst before the upper limit of the sensor (∼250 mm Hg) was reached. Additionally, four samples were disrupted during bowel clamping and rendered unusable. This did not leave a large enough sample for statistical analysis. The minimum burst pressure was 115 mm Hg in the control group, 84 mm Hg in the AD group, and 138 mm Hg in the ND group, these values being significantly higher than the mean resting intragastric pressures of ∼9 mm Hg measured by Toubanakis et al. in healthy dogs. 3
Jejunum: Day 3 burst pressures were compared with a paired t-test following the exclusion of six samples for which burst pressures were not obtained. There were 10 samples left in each of the 3 groups. There was no statistically significant difference in mean burst pressure between the control and AD groups (P=.23) or between the control and ND groups (P=.47) on day 3.
Colon: Day 3 burst pressures in the colon were compared with a paired t-test. In comparing the control and AD groups, six samples and paired data were removed from analysis because of sample disruption, leaving a sample size of four per group. Similarly, in comparing the control and ND groups, a total of four samples and paired data were excluded from analysis because of sample disruption, leaving a sample size of six per group. There was no statistically significant difference in mean burst pressure between a colotomy closed with control suture versus AD (P=.59) or between a colotomy closed with control suture versus one closed with ND (P=.64) on day 3.
Table 2 displays the overall summary results of the day 3 burst pressure testing, excluding samples that exceeded the limit of the pressure sensor.
AD, absorbable (polyglyconate) device; ND, nonabsorbable (polybutester) device; Q1, quartile #1; Q3, quartile #3.
Days 10 and 21
None of the control or AD suture lines from the stomach, jejunum, or colon burst before reaching the upper limit of the pressure sensor (∼250 mm Hg) at either the day 10 (5 samples per device and tissue) or day 21 (5 samples per device and tissue) time points. Therefore, no burst pressure data were available for statistical analysis on these samples. Similarly, none of the ND samples burst from the suture line before reaching the upper limit of the sensor at the day 10 or 21 time points. One ND colon sample burst at the upper limit of the pressure transducer from native tissue at a site away from the actual suture line.
Discussion
Clinical application of barbed suture is not extensive, with most experience found in plastic and reconstructive surgery, as well as in urology.4,5 Murtha et al. demonstrated equivalent results in terms of wound cosmesis and dehiscence in a randomized study. 4 Demyttenaere et al. reported the first known use of barbed suture in gastrointestinal closure. 2 In that swine study, enterotomy closure with the V-Loc™ advanced closure device (Covidien) was associated with significantly reduced suturing time (by about 25%) and with adhesion scores, burst pressures, and histology scores comparable to the control suture. Gastrointestinal anastomosis creation and enterotomy closure of other types represent the most relevant laparoscopic application of this suture technology.
Our study reports the first use of barbed suture for laparoscopic gastrointestinal closure. The similarities between canine and human gastrointestinal anatomy and physiology made the canine model ideal for this study. 3 The objectives were to examine the in vivo efficacy of knotless barbed suture for laparoscopic single-layer enterotomy closure by comparing the relative burst strength of enterotomies closed with barbed monofilament sutures for the Endo Stitch to ones closed with an absorbable suture (Polysorb for the Endo Stitch) at 3, 10, and 21 days postoperatively, as well as to examine the impact of this novel suture technology on operative time.
The closure leak rate in this study with 216 total enterotomy closures was 0%. There was no clinical evidence of leak in any of the animals. Two animals in the day 3 group died before reaching scheduled euthanasia. Necropsy in both of these animals showed no evidence of disrupted enterotomy closure or leak. Likewise, postmortem examination in all the remaining animals revealed healing or well-healed enterotomy closures without leak or abscess to signify a subclinical leak that went undetected. It may be important to note that the postoperative diet in these animals was not significantly limited as is common following gastrointestinal surgery in humans, creating an opportunity for early testing and potential failure of the enterotomy closures. The effect of postoperative dietary restrictions in preventing or precipitating leaks is unknown, however, so this point is difficult to stress.
Day 3 burst pressure data collection and analysis represents a limitation of this study. Several data points were rendered unusable because of the friability encountered in the tissues as well as early adhesions that needed to be disrupted to gain access to the suture lines for burst pressure testing. This was not a particularly unexpected finding, but it limits our ability to make definitive conclusions about the efficacy of the suture materials at day 3. Moreover, the detectable pressure difference at day 3 in colonic tissue for AD and ND were higher than expected based on preliminary data used to calculate study sample size and was exacerbated by the loss of samples and the arrangement of the lost data, resulting in a small paired data sample size. Nonetheless, days 10 and 21 data show no suture line disruptions during burst testing in the stomach, colon, or jejunum for any of the suture materials tested.
Overall, our data demonstrate that both the absorbable and nonabsorbable barbed monofilament sutures for the Endo Stitch are effective for laparoscopic single-layer gastrointestinal closure and are associated with a significantly reduced closure time, thus providing a viable alternative to conventional suture in laparoscopic gastrointestinal surgery.
Footnotes
Acknowledgment
This study was supported by a grant from Covidien.
Disclosure Statement
Drs. P. Omotosho, B. Yurcisin, and E. Ceppa have no conflicts of interest or financial ties to disclose. J. Miller is a full-time employee of Covidien. D. Kirsch is a full-time employee of Covidien. Dr. D.D. Portenier is a consultant for Covidien.