
Abstract
Abstract
Purpose:
The management of juvenile idiopathic scoliosis (JIS) in young children can be challenging. Vertebral body stapling (VBS) is a new alternate to bracing and is intended to reduce or eliminate the need for subsequent spinal fusion. In concept, VBS of the anterior spine inhibits curve progression, thus stabilizing the spine as the child grows. There is a paucity of data in the pediatric population on its effectiveness. Therefore, we reviewed our experience with thoracoscopic VBS in children with juvenile scoliosis.
Subjects and Methods:
After Institutional Review Board approval was obtained, a retrospective study was conducted on all patients who underwent thoracoscopic VBS for scoliosis from January 2007 to December 2010. Only patients with a follow-up of at least 2 years were included in this study group. Data obtained were demographics, indications for VBS, degree of curvature, treatment, complications, and follow-up. Cobb angle was used to measure the initial degree of curvature on a standing posterior–anterior spine radiograph.
Results:
During the study period, 11 patients underwent thoracoscopic VBS for JIS using single lung ventilation in a lateral position. Of those, 7 patients ages 8–11 years (mean, 9 years) with a mean body mass index of 17 kg/m2 (±2.9 kg/m2) had at least a 2-year follow-up and make up the study group for this review. Indications for stapling in these 7 patients were progression of scoliosis (n=3), noncompliance with brace (n=3), and double curve with progression (n=1). The mean preoperative Cobb angle was 34.1±5° (range, 25°–41°), and the mean immediate postoperative Cobb angle was 23±5° (range, 16°–30°). The staples encompassed a mean number of 6.4 vertebral bodies. The mean duration of chest drainage was 2.7 days (range, 2–6 days), and the mean length of hospitalization was 3.9 days (range, 3–7 days). The mean operative time was 156.2±39.5 minutes (range, 101–214 minutes). There were no intraoperative complications or mortality. Postoperatively, 1 patient developed a pleural effusion on the contralateral side that required drainage. These 7 patients have been followed up for a mean of 34 months (range, 29–44 months). The mean Cobb angle at last follow-up was 24.7° (range, 15–38°). No patient has required postoperative bracing or spinal fusion.
Conclusions:
Thoracoscopic VBS is a safe and effective method of treatment for progressive scoliosis in young children. Pediatric surgeons may be asked to assist their spine surgeons with this new approach to juvenile scoliosis.
Introduction
VBS involves the placement of Nitinol (nickel–titanium Naval Ordnance Laboratory) metal staples between two vertebral bodies on the convex side of the anterior spine that tethers the end vertebra growth plates, which slows the lateral growth progression and potentially allows the curvature to resolve. As juvenile scoliosis over 30° has a high chance of needing traditional corrective surgery, VBS is a reasonable option for these children when brace treatment has failed or is not possible. There is a scant amount of data in the pediatric population on its effectiveness. Therefore, we reviewed our experience with thoracoscopic VBS in children with JIS.
Subjects and Methods
After Institutional Review Board approval was obtained, a retrospective study was conducted on all patients who underwent thoracoscopic VBS for scoliosis from January 2007 to December 2010. In total, 11 patients were identified as having VBS for scoliosis. Four were excluded from the analysis (2 with open lumbar procedures, 1 with a previous posterior growth rod in place, and 1 with less than 2 years of follow-up). Only data from patients with a primary thoracoscopic procedure with follow-up of at least 2 years are included in this report. Data included demographics, indications for VBS, degree of curvature, treatment, complications, and follow-up. Cobb angle was used to measure the initial degree of curvature on a posterior–anterior spine radiograph.
Operative technique
The procedure is performed as a collaborative effort among pediatric surgeons, spine surgeons, and anesthesiologists. The patient is intubated with a double-lumen endotracheal tube, which allows the ipsilateral lung to collapse. He or she is then positioned on a flat radiographic operating table in the lateral decubitus position with the convex side of the scoliosis in the up position. VBS is performed thoracoscopically by an anterior approach, and access is obtained by the pediatric surgeon. An initial 10-mm incision is made in the anterior axillary line at the level of the apex of the curve (Fig. 1). Using a cut-down technique, a 10-mm port and telescope are introduced. CO2 insufflation is initiated at 8–10 torr to further collapse the lung. The correct vertebral bodies are confirmed using fluoroscopy. A 2-cm incision is needed at a 90° angle to the vertebral column to introduce the staples and other instruments needed to deploy the staples. Usually, two or three staples can be inserted through one 2-cm incision. In the patient seen in Figure 1, two 2-cm incisions have been marked preoperatively in preparation for placing six staples. Usually five to seven staples are needed. At each vertebral interspace, a trial device is inserted to ensure the correct staple size and used to create preliminary pilot holes. Segmental vessels may need to be cauterized if they will be pierced by the staple. The staple is temperature sensitive and is made from Nitinol, composed of 50% nickel and 50% titanium. The chilled staple has a U shape and is inserted spanning two adjacent vertebral bodies (Fig. 2). When it is warmed by the body's temperature, it assumes a C shape and secures the vertebral bodies tightly. Proper position of each staple is assured using fluoroscopy in both an anterior and lateral plane (Fig. 3). Usually, the first staple placed is the most caudal staple, typically at T12 or T11, and the surgical team works superiorly to about T5 or T4, depending on the limits of the primary structural curve. The procedure takes about 3 hours to perform. A small pliable chest drain is inserted upon completion of the operation and is generally removed 2–3 days later. The child is typically discharged 3–4 days after surgery and can return to school in about 2–3 weeks. Patients are instructed to avoid sports and physical activities for 6 weeks.
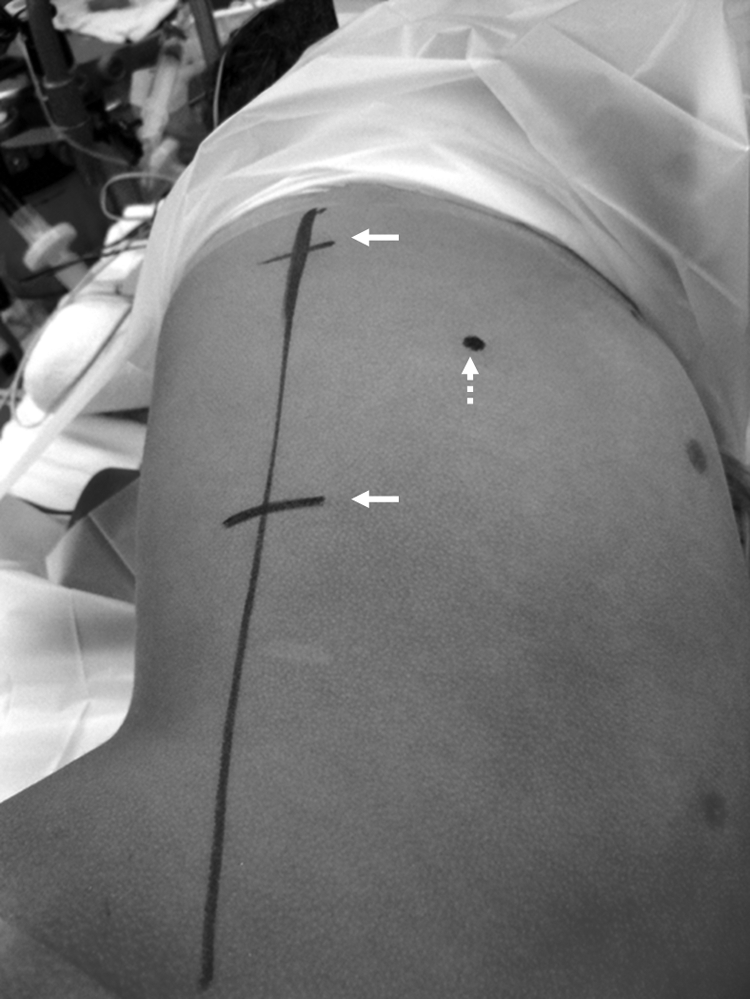
The patient is positioned in the lateral decubitus position with the convex side of the scoliosis in the up position. Using fluoroscopy, the vertebral column has been identified and marked externally with the long vertical line. The dotted arrow shows the planned position of the initial 10-mm cannula in the anterior axillary line through which the telescope attached to the camera will be introduced. The two solid arrows indicate the planned location of the two 2-cm incisions through which the staples will be inserted. Generally, two or three staples can be introduced through one 2-cm incision.

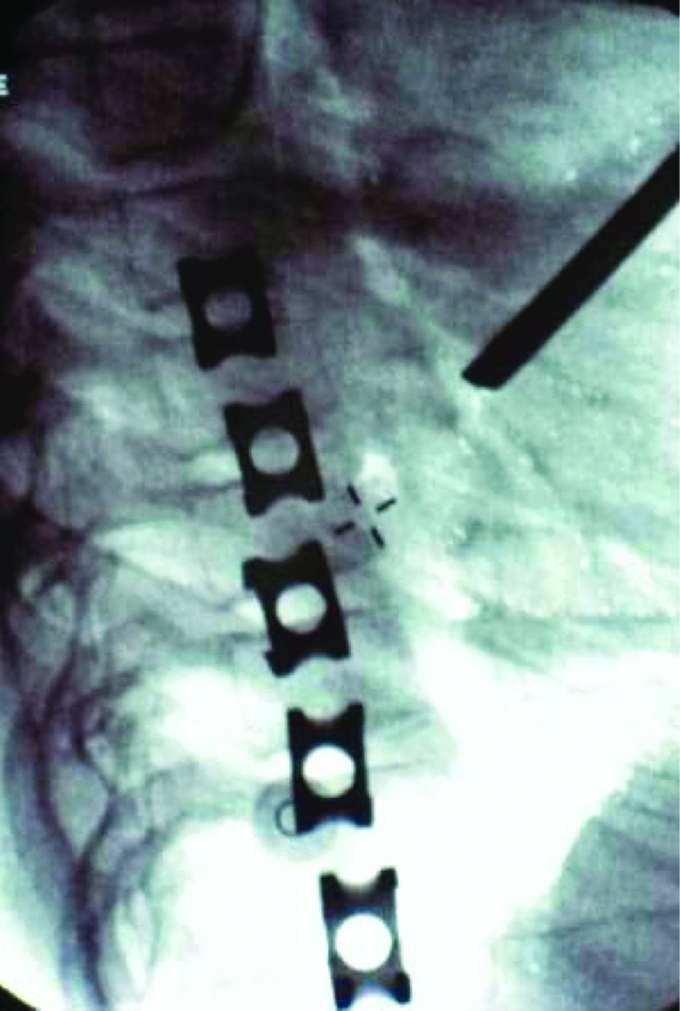
This intraoperative lateral fluoroscopic image shows good alignment of the five staples used in this young child with significant juvenile scoliosis.
Results
The study group comprised 7 patients, with a minimum of 2-year follow-up, who underwent VBS between January 2007 and December 2009. These 7 patients ranged in age from 8 to 11 years, with a mean age of 9 years, at the time of their surgery. There were 4 girls and 3 boys. The mean body mass index was 17 kg/m2 (±2.9 kg/m2). There were several indications for stapling, which included progression of scoliosis (n=3), noncompliance with brace (n=3), and double thoracic curves with progression (n=1). All patients either progressed their deformity despite bracing or were unable to wear the brace. In total, 45 staples were inserted, encompassing a mean number of 6.4 vertebral bodies. The majority of patients (5 [71%]) required right-sided staples. The mean preoperative Cobb angle was 34.1±5° (range, 25°–41°), and the mean immediate postoperative Cobb angle was 23±5° (range, 16°–30°).
A small soft chest drain was placed in all patients. The mean duration of drainage was 2.7 days (range, 2–6 days). The mean length of hospitalization was 3.9 days (range, 3–7 days). The mean operative time was 156.2±39.5 minutes (range, 101–214 minutes). There were no intraoperative complications or mortality. Postoperatively, 1 patient developed a pleural effusion on the contralateral side that required drainage. The etiology of this effusion is unclear.
These 7 patients have been followed up for a mean of 34 months (range, 29–44 months). The mean Cobb angle at last follow-up was 24.7° (range, 15–38°) as measured on standing posterior–antererior plain radiographs.
Improvement was defined as correction of the preoperative Cobb angle of >10°. A change in the preoperative Cobb angle of +10° to −10° was considered to be no change, while progression of disease was defined as worsening of the curve by >10° from the preoperative Cobb angle. Improvement was obtained in 5 patients (71.4%), while there was no change in the postoperative Cobb angle in 2 patients (28.6%). The mean Cobb angle percentage correction for the total group was 36% (range, 16.2%–56% correction). No patient demonstrated curve progression postoperatively. There were no staple dislodgements, and no patient has required subsequent spinal fusion.
Discussion
The tendency for JIS to spontaneously resolve is very infrequent as most progressive curves are within the thoracic spine. 3 Moreover, a younger age at the time of onset and at the time of curve progression usually correlates with a worse deformity and with the greatest functional disability. 3
Historically, spinal bracing has been the initial treatment for juvenile scoliosis. Children are instructed to wear a thoraco-lumbo-sacral-orthosis spine brace for 20 hours a day, although the greatest effectiveness is obtained if worn for up to 23 hours per day. 4 The usefulness of a thoraco-lumbo-sacral-orthosis brace and its success in achieving cessation of curve progression are contingent on overall compliance with wearing the brace for an extended amount of time each day. Generally, very young children adapt better to the brace, while older children, boys, and obese children may have less success with a thoraco-lumbo-sacral-orthosis brace. Some children may not tolerate the brace or have a poor self-image, becoming withdrawn and depressed. Additionally, the child may have to wear the brace for several years until he or she is fully grown, and there is still no guarantee of successful treatment of the scoliosis. Moreover, the benefits of bracing may be overestimated as compliance is often difficult to ascertain accurately.
Unfortunately, over 50% of juveniles will have progressive scoliosis even with bracing and compliance. 1 It has been reported that the best correction of bracing was 38% in the first year and 43% after 2 years with a slow deterioration of 1° per year. 3 After 5 years of bracing, a more rapid deterioration often occurs, noting a mean correction of only 11%. 3
Curves of more than 30° have a very high chance of requiring operative correction. When bracing becomes ineffective or when the children are not wearing the brace, an operative approach is warranted. Traditionally, growing rods or spinal fusion have been the two most common surgical treatment options for JIS. Growing rods are implanted and surgically extended every 6 months until growth stops at skeletal maturity. For children younger than 11 years of age (before the onset of puberty) and with curves between 25° and 40°, VBS is an ideal alternative to bracing, growing rods, and spinal fusion. VBS involves placement of staples across the end vertebral growth plate to modulate the asymmetrical growth of the spine by slowing the growth of the convexity. The staples also allow the concave side of the scoliosis to grow and catch up, thus preventing worsening of the deformity and potentially improving it. Once the child reaches maturity, the growth of the spine ceases, and the curvature does not progress.
Curves in the thoracic spine, as well as the lumbar spine, have been successfully stapled. The reported success rate for thoracic curves that are less than 35° has been documented at 79%. 1 An 86% success rate is reported if the first standing radiograph following surgery demonstrates the curve to be less than 20°. 1 VBS is more successful if the child has several years of growth remaining; hence success may be limited in older children. Children with curves greater than 35° and those with extensive kyphosis are less successfully corrected with VBS. For children with more severe scoliosis, with curves over 45°–50°, VBS is less likely to be successful alone, and other surgical modalities, such as posterior growing rods, may also need to be implemented. Also, patients with a nickel allergy are not candidates for this approach at this time.
The surgical approach and management of scoliosis can be challenging. For patients with progressive JIS or those unable to wear a brace, thoracoscopic VBS is an alternative treatment. Thoracoscopic VS is a safe and effective method of treatment for progressive scoliosis in young children. Pediatric surgeons may be asked to assist their spine surgeons with this new approach to juvenile scoliosis.
Footnotes
Disclosure Statement
No competing financial interests exist.