
Abstract
Abstract
Background:
During liver resection, bleeding remains the most important challenge. A reduction in blood loss and avoiding the need for a blood transfusion are important objectives for liver surgeons today. The authors compared the intra- and postoperative course of patients undergoing laparoscopic liver resections under intermittent total pedicle occlusion (IPO), hemihepatic vascular occlusion (HVO), and selective vascular occlusion (SVO).
Subjects and Methods:
Retrospective analysis was conducted of patient data from 41 cases of laparoscopic liver resection in three groups of patients under different occlusion methods, including 15 cases of IPO, 15 cases of HVO, and 11 cases of SVO. The advantages and disadvantages of the various methods were compared, as well as blood loss, operation time, changes in postoperative liver function, and complications.
Results:
There was no operative death in any of the 41 patients. Generally, there was no significant difference among the three groups in blood loss, clamping time, or operative time. After the operation, the effect on liver function for the HVO and SVO groups was significantly less severe than that for the IPO group (P<.05). The incidence of postoperative complications was mainly related to IPO and the larger amount of bleeding.
Conclusions:
Both HVO and SVO are feasible in laparoscopic hepatectomy and have the advantage of reducing liver remnant ischemia injury and modality rate over IPO. HVO is easy to do for left lateral lobe or resection of the left half of the liver. SVO is suitable for right lobe resection.
Introduction
Compared with open liver resection, laparoscopic liver resection requires a longer time in surgery and causes more bleeding, and bleeding is more difficult to stop; therefore, it is essential to choose the correct portal triad clamping method.10,11 This study retrospectively analyzed the intraoperative and postoperative results of 41 cases of laparoscopic liver resection, from October 2004 to October 2010, in which different methods of hepatic portal triad clamping were implemented and examined vessel occlusion methods for laparoscopic liver resection.
Subjects and Methods
Patients
From October 2004 to October 2010, in total, 268 patients underwent liver resection at our institution (Northern Jiangsu People's Hospital), including 41 patients who underwent laparoscopic liver resection. Retrospective analysis was conducted of patient data from the 41 cases of laparoscopic liver resection in three groups of patients treated with different occlusion methods, including 15 cases of intermittent hepatic pedicle occlusion (IPO), 15 cases of hemihepatic vascular occlusion (HVO), and 11 cases of selective vascular occlusion (SVO). The advantages and disadvantages of the various methods were compared, including blood loss, operation time, changes in postoperative liver function, and complications.
Surgical procedure
Body positioning and trocar placement
All patients underwent surgery under general anesthesia. Patients were in a supine position with the head elevated higher than the feet and with legs apart and tilted 30° to the left or right according to the lesion locations (e.g., if lesions were on the right side, the surgeon would be on the patient's left side), with CO2 pneumoperitoneum pressure of 13 mm Hg. The trocar was placed in a position similar to that used for the four-hole laparoscopic cholecystectomy method, and appropriate adjustments were made based on tumor location. If lesions were located in the left liver, the primary incision should run from under the xiphoid process to under the left costal margin on the midclavicular line.
In brief, the procedures were performed with CO2 pneumoperitoneum, and abdominal pressure was electronically maintained below 13 mm Hg. A 30° laparoscope was used in all cases. The liver was examined visually and by intraoperative ultrasonography to confirm the number and size of the lesions and define their relationship with the intrahepatic vascular structures.
Hepatic inflow occlusion
The methods used in the study included intermittent IPO, HVO, and SVO. IPO, also called the Pringle maneuver, was applied with 15-minute clamping and 5-minute release periods (Fig. 1A). HVO, which is similar to a half Pringle maneuver, occluded the lesion-lateral portal vein and hepatic artery (Fig. 1B). Methods of vascular occlusion for SVO are occlusion with the portal vein and lesion-lateral hepatic artery. In this process, the ipsilateral hepatic artery was first exposed, and then a tape was placed around the portal vein and the lesion-lateral hepatic artery, which were occluded except for the contralateral hepatic artery (Fig. 1C).
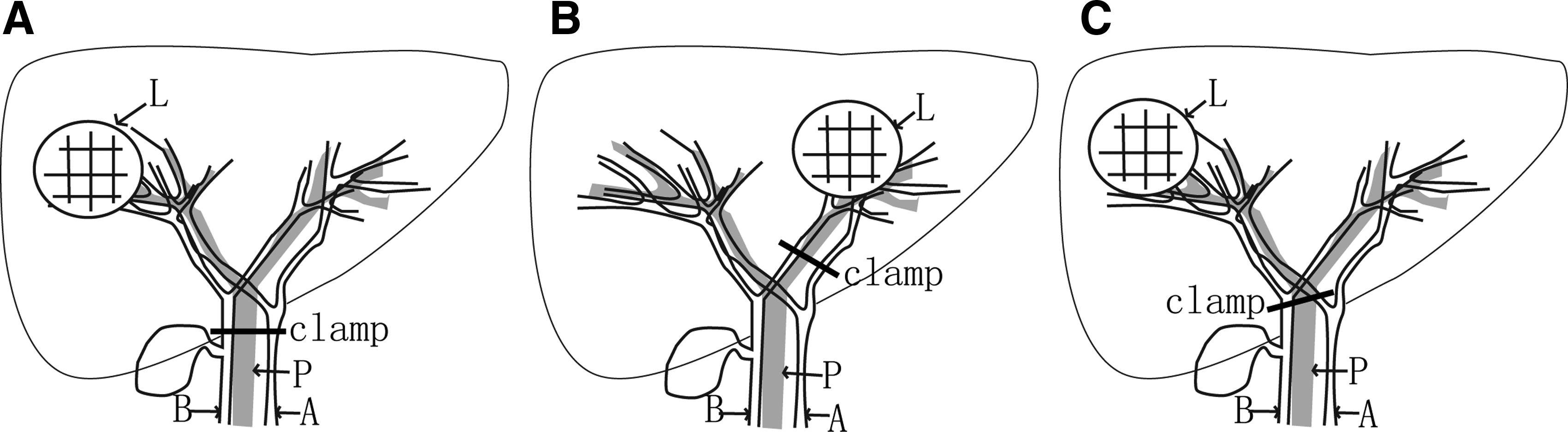
Schematic drawing of hepatic inflow occlusion:
Transection of liver parenchyma
We turned on the high-frequency electrocoagulation device so that the output power was 70–80 W and then used the electrocoagulation scalpel (Tianjin Hana Gongshi, China) to perform liver resection. After the resection line for the liver was determined, the liver was cut to a depth of 0.5–1.0 cm along the resection line by direct use of the electrocoagulation scalpel. Pushing, scraping, suction, and coagulation were then performed simultaneously, which exposed the intrahepatic ducts. Small vessels were coagulated directly, and large vessels were occluded using titanium clip or Hem-o-Lok® (Teleflex Medical, USA) clamping. Larger structures were secured with clips. Portal pedicles and major hepatic veins were divided by application of a Hemo-Lok clip.
Removing the resected specimen
The 12-mm trocar was removed, and its site was enlarged. An endo bag was inserted and deployed in the intraabdominal cavity, and the resected specimen was placed in the specimen retrieval bag. The specimen retrieval bag was closed and brought against the anterior abdominal wall. For larger samples, anhydrous alcohol was injected before samples were removed from the sample bags, and the samples were removed after tumor cells had been destroyed.
Statistical analysis
The clinical characteristics analyzed, including blood loss, operation time, changes in postoperative liver function, morbidity, and mortality, were analyzed using a statistical analysis program package (SPSS version 15.0, SPSS Inc., USA). The results are expressed as mean±standard deviation values. The statistical significance of observed differences was tested by using the chi squared test, Fisher's exact test, or the Mann–Whitney test. A probability of .05 or less (P<.05) was considered statistically significant.
Results
There were 41 patients in the group (28 men and 13 women) with a mean age of 50.3 years (range, 26–77 years) and no conversion to open surgery (Table 1). Mean operative time was 170 minutes (range, 70–260 minutes), with mean blood loss of 245 mL (range, 50–1000 mL). All patients experienced postoperative recovery of gastrointestinal function within 24–48 hours, meaning that they began to eat and got out of bed. Postoperative bile leak rate was 4.9%; these leaks were treated with drainage for 2 weeks. One patient with diabetes, which involved infection with formation of abscesses, who underwent liver resection 1 month after discharge was cured by percutaneous drainage. The ascites rate was 9.7%; ascites was cured after liver-protective diuretic therapy. The subphrenic effusion rate was 2.4%.
There were no significant difference in preoperative data among the three groups (P>.05).
HVO, hemihepatic vascular occlusion; IPC, intermittent total pedicle occlusion; SD, standard deviation; SVO, selective vascular occlusion.
The underlying pathology was hepatocellular carcinoma (n=18), cholangiocellular carcinoma (n=4), liver metastasis from colon cancer (n=3), liver metastasis after stromal tumor surgery (n=2), intrahepatic cystadenocarcinoma (n=1), left hepatic stones (n=5), hepatic hemangioma (n=7), and hepatic vascular lipoma (n=1). The mean postoperative hospital stay was 9 days (range, 6–19 days). Mean maximum lesion size was 6×4×5 cm (range, 3×2×2–11×8×9 cm). Twelve cases had hepatocellular carcinoma associated with different degrees of cirrhosis of the liver, combined with splenomegaly, and 6 cases had hypersplenism.
The tumors were located in segments II, III, and IV (n=8), segments II and III (n=4), segment II (n=1), segment III (n=2), segment IV (n=5), segment V (n=8), segment VI (n=10), segment VII (n=1), and segment VIII (n=2). Preoperative preparation was the same as for open surgery. In terms of liver resection, there were 7 cases of left hepatectomy and 6 cases of hepatic left lateral lobectomy. The other cases involved liver wedge resection: There were 5 cases in liver segment IV, 7 cases in segment V, 6 cases in segment VI, 1 case in segment VII, and 1 case in segment VIII. Six patients with splenomegaly underwent splenic artery ligation to control hypersplenism. Two patients with early intrahepatic bile duct stones combined with cholangiocellular carcinoma were subjected to bile duct exploration along with the surgery.
Intraoperative outcome
In this study, 26 patients in the IPO and SVO groups underwent liver wedge resection; in the HVO group, there were 6 cases with left lateral resection and 9 cases with left hepatectomy. Statistical t tests revealed no statistically significant difference among the IPO, HVO, and SVO groups with regard to average hepatic inflow flow occlusion time, surgical time, or blood loss (Table 2) (P>.05).
Data are mean±SD values.
Compared with the IPC group, the HVO and SVO groups do not have significant differences in operation time, blood loss, and occlusion time (P>.05).
Changes in liver function
Figures 2–5 show changes in liver function for patients in the three groups. The HVO and SVO groups had significantly higher levels of prealbumin than the IPO group at 3 days. On the other hand, the magnitudes of the serum bilirubin, alanine aminotransferase, and aspartate aminotransferase level increases in the IPO group were significantly higher than in the HVO and SVO groups (P<.05), but there were no significant difference between the HVO and the SVO groups.
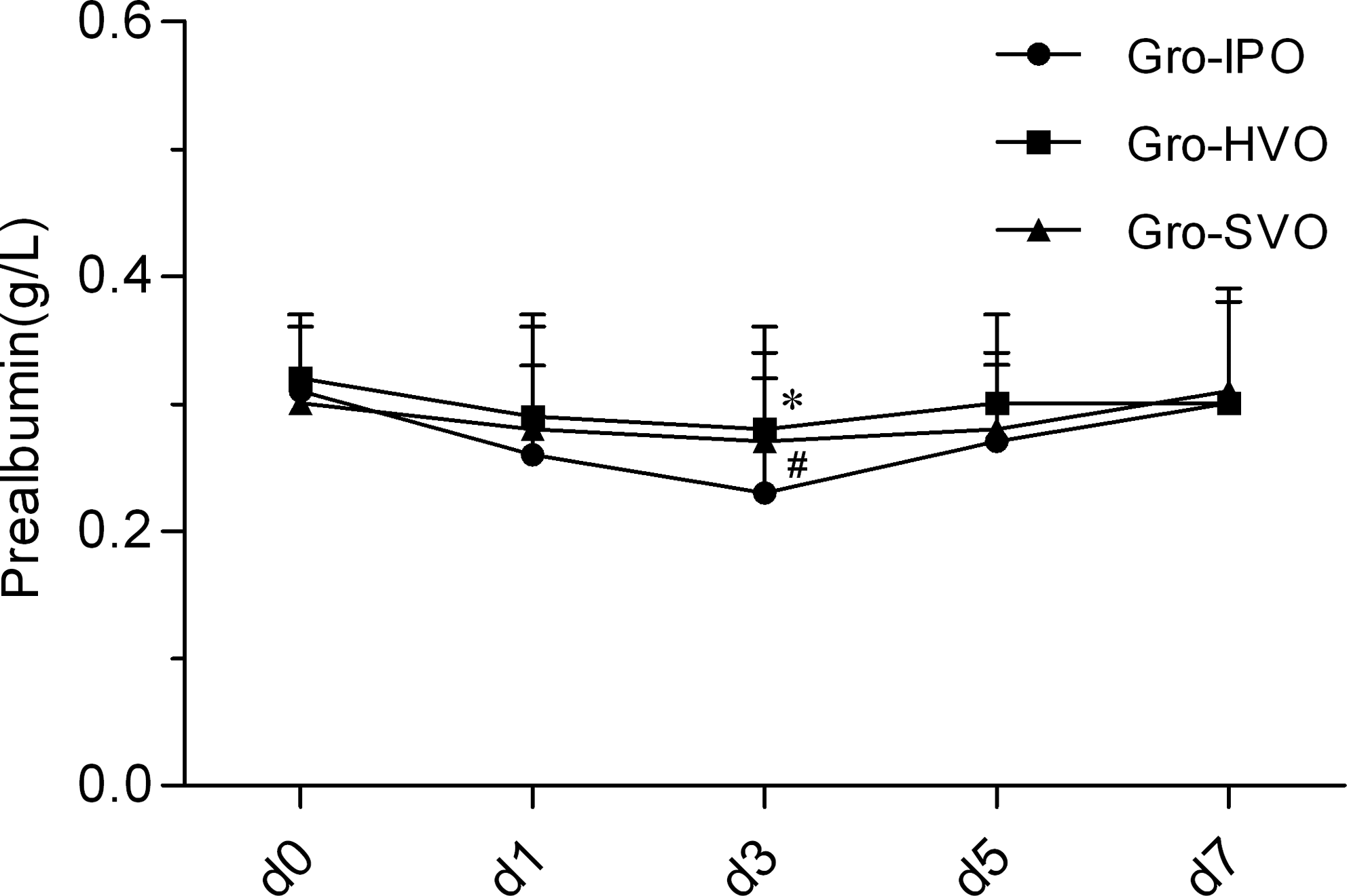
Changes in serum prealbumin level after surgery for the three groups of patients: Intermittent total pedicle occlusion (Gro-IPO), hemihepatic vascular occlusion (Gro-HVO), and selective vascular occlusion (Gro-SVO). Data are mean±standard deviation values. *P<.05, Gro-HVO compared with Gro-IPO; #P<.05, Gro-SVO compared with Gro-IPO.
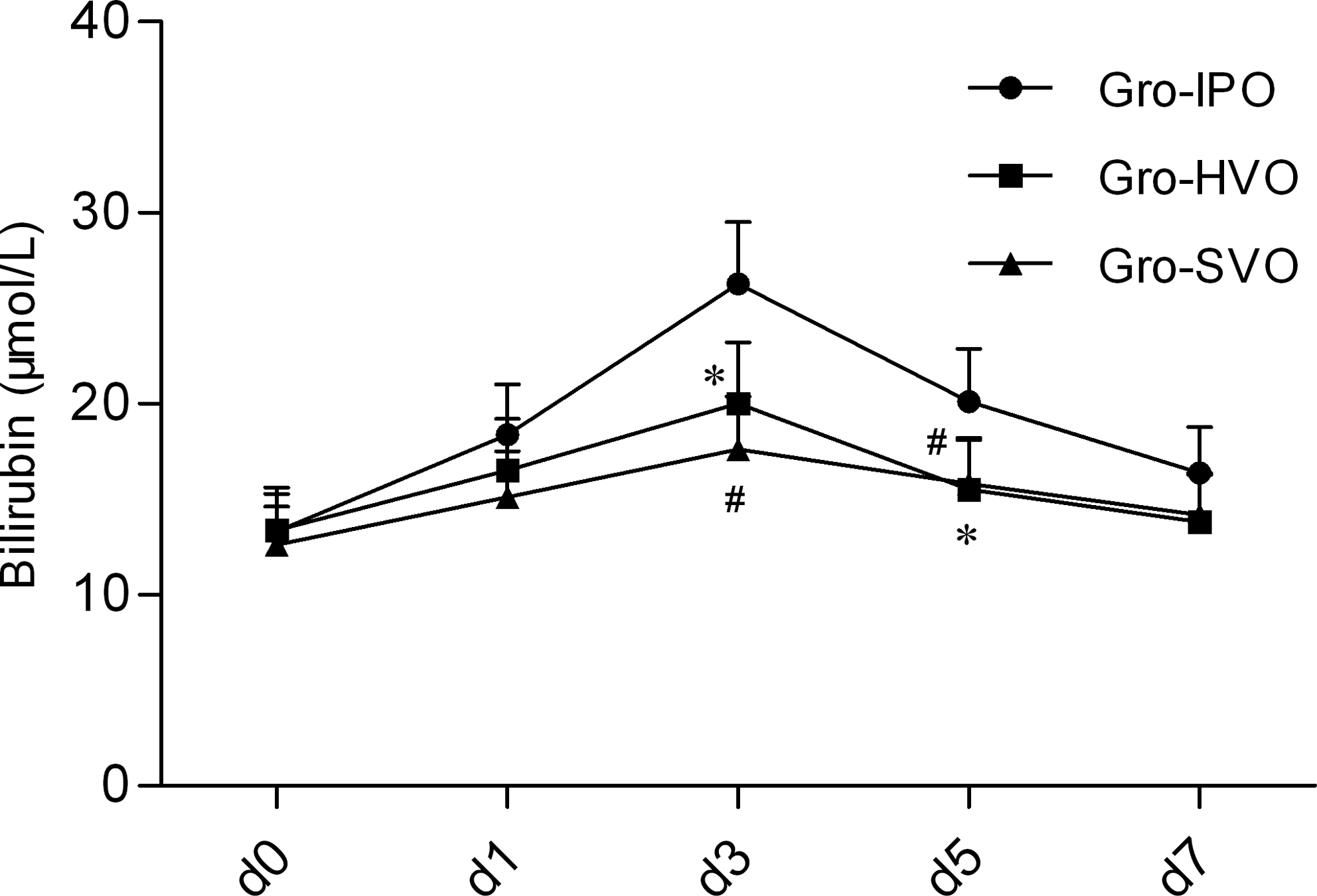
Changes in serum bilirubin level after surgery for the three groups of patients: Gro-IPO, Gro-HVO, and Gro-SVO. Data are mean±standard deviation values. *P<.05, Gro-HVO compared with Gro-IPO; #P<.05, Gro-SVO compared with Gro-IPO.
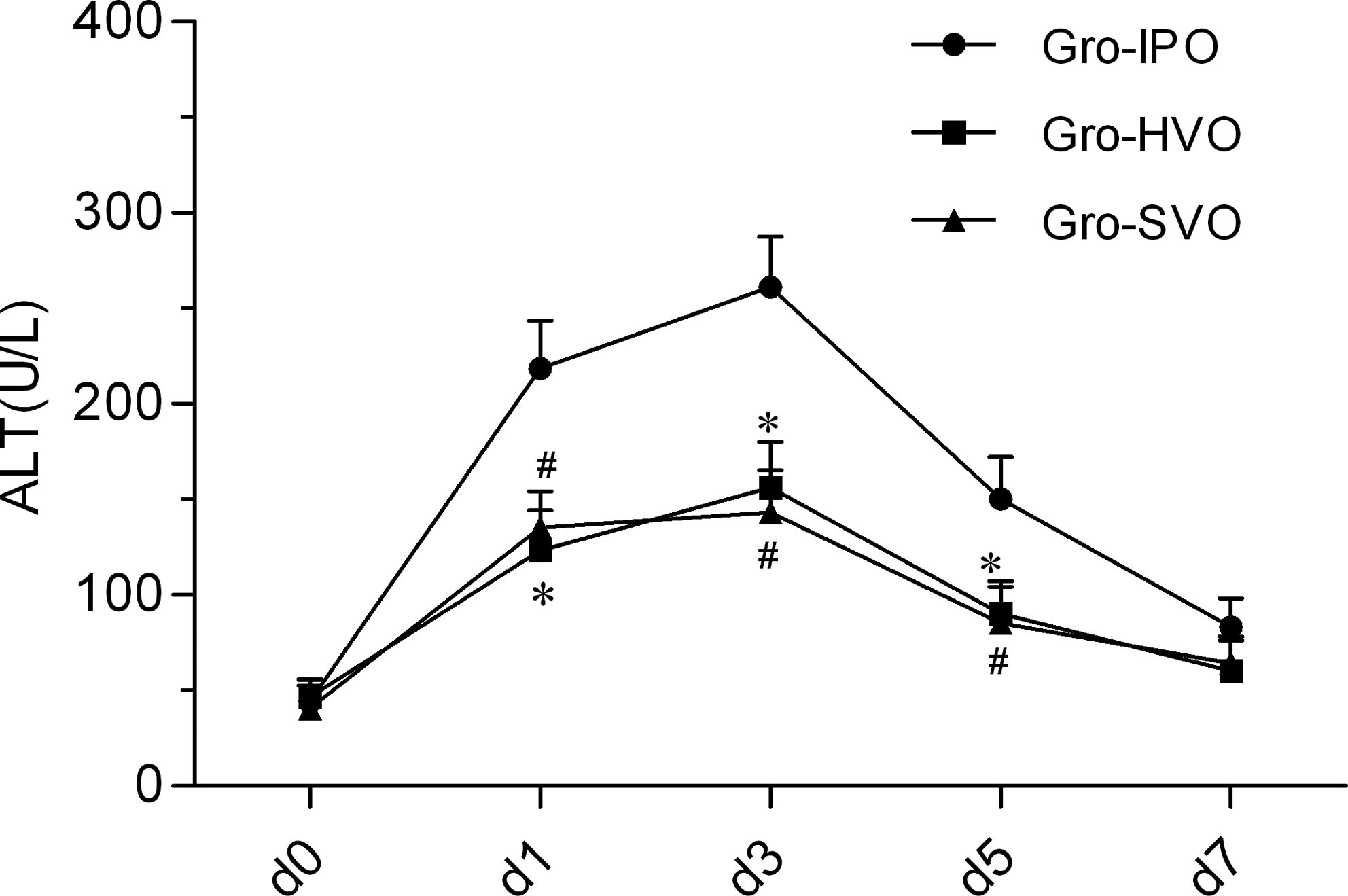
Changes in serum alanine aminotransferase (ALT) after surgery for the three groups of patients: Gro-IPO, Gro-HVO, and Gro-SVO. Data are mean±standard deviation values. *P<.05, Gro-HVO compared with Gro-IPO; #P<.05, Gro-SVO compared with Gro-IPO.
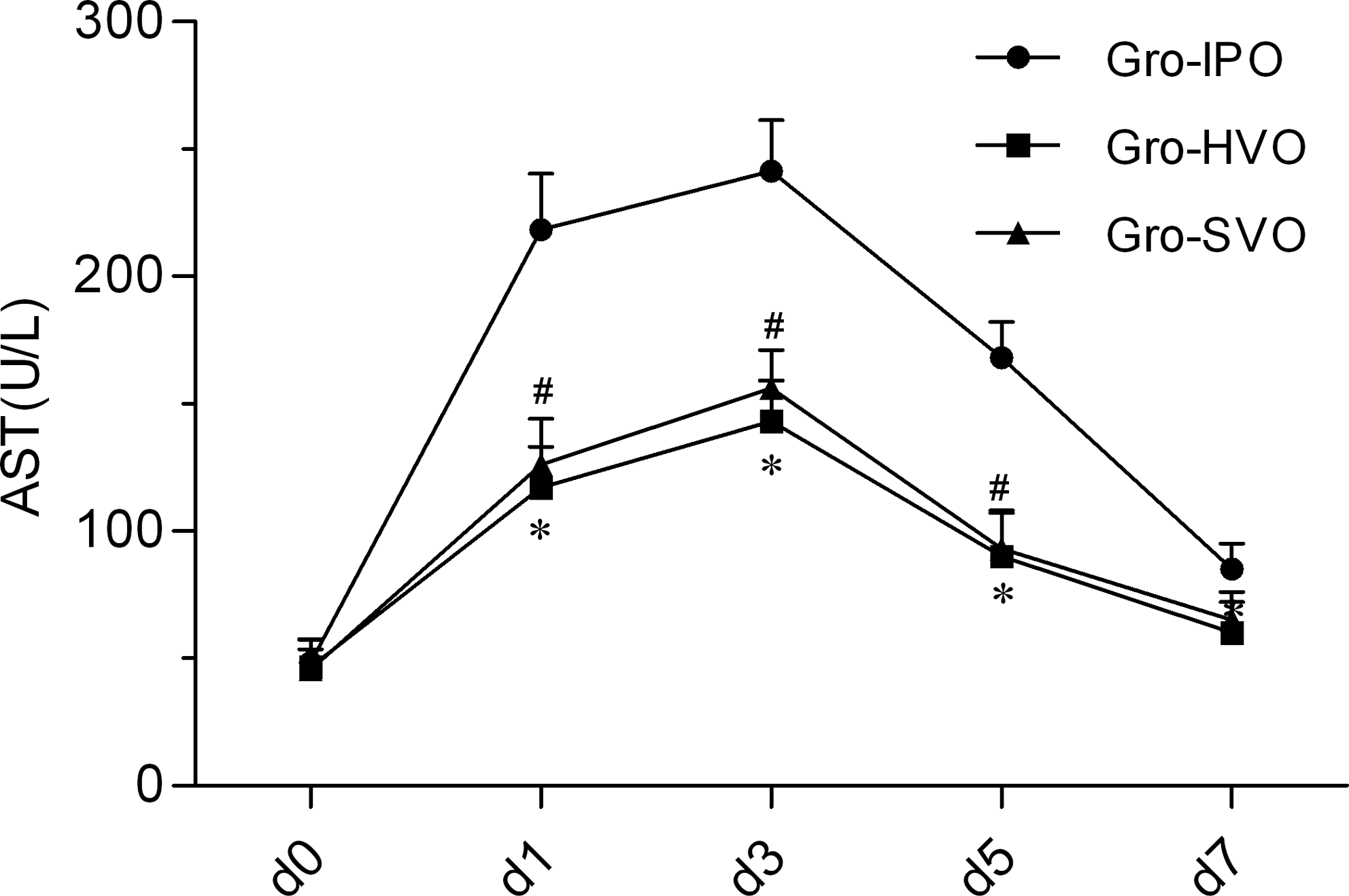
Changes in serum aspartate aminotransferase (AST) after surgery for the three groups of patients: Gro-IPO, Gro-HVO, and Gro-SVO. Data are mean±standard deviation values. *P<.05, Gro-HVO compared with Gro-IPO; #P<.05, Gro-SVO compared with Gro-IPO.
Postoperative complications
In total, 10 patients experienced various complications; the incidence rate was 24.4%. In the IPO group, 5 patients had complications, yielding a rate of 33.3%, including 1 case with subphrenic fluid infection, 4 cases with intractable ascites, and 1 case with pulmonary infection. In the SVO group, there were 2 cases (18.2%) with complications (2 cases with ascites). In the HVO group, 3 patients (20%) had complications: 1 case with subphrenic infection and 2 cases with biliary fistula. After complications were found, patients in the three groups were cured by conservative treatment; there was no perioperative death. The univariate logistic regression analyses demostrated that hepatic vascular occlusion methods and the amount of bleeding after liver resection were independent risk factors of morbidity rate (Table 3).
Data are mean±SD values.
P<.05, significant compared with before surgery in the same group.
P<.05, significant difference compared with the IPO group.
Discussion
The primary concern in liver surgery is to minimize blood loss and avoid transfusions, which have been shown to have a deleterious impact on both short- and long-term outcome.1,2 This goal can be achieved by intraoperative clamping of the hepatic pedicle (inflow occlusion) or by total vascular occlusion. Among these techniques, IPO (the Pringle maneuver) still stands out as the most simple and effective method. 12 This maneuver involves control of hepatic vascular inflow by clamping the hepatoduodenal ligament. During hepatectomy, the Pringle maneuver is still commonly used as a routine procedure.13–16 However, ischemic insult to the remnant liver is always a concern when this maneuver is applied, particularly in cirrhotic livers.17,18
As reported in the literature,19–22 the normal liver can tolerate up to 60 minutes, or even longer, at room temperature under continuous inflow occlusion. Liver cirrhosis and chronic liver disease patients exhibit shortened tolerance.22,23 Giuliante et al. 24 have proposed that patients with the application of IPO have significantly higher bilirubin and transaminase levels and experience more postoperative complications, where these effects may be related to extended occlusion. In East Asia and other regions with a high incidence of liver cancer, the majority of liver resections are performed for primary liver cancer patients, 80% of whom have cirrhosis, and the liver tolerance to occlusion is poor.23,25 Especially for laparoscopic liver resection, it is necessary to clamp the portal triad for a long time; therefore, extended hepatic inflow occlusion or intraoperative bleeding can increase the burden on the compensatory liver, causing liver dysfunction and even severe liver failure. Therefore, determining how to control bleeding in liver resection while minimizing hepatic ischemia and hypoxia is the key to ensuring successful surgery and postoperative recovery. 23
HVO was performed to selectively block one side of the liver lesion (left or right liver) and complete the hepatic artery and portal vein resection, so that blood circulation is maintained. 26 Thus, function of the healthy side of the liver is retained in order to avoid contralateral hepatic ischemia–reperfusion. The incision line for resection is clear, allowing for intraoperative hemodynamic stability, which allows for prolonged blood flow occlusion. The surgeon therefore has sufficient time for detailed processing of the section. Mesenteric blood flow can still flow back through the liver to enter the circulation of the healthy side. Intestinal bacteria and endotoxin translocation and intestinal damage should not occur because of portal triad clamping, and the postoperative complication rate is low. Therefore, damage to the liver is minimal, and recovery is rapid.27,28 However, this method should first be performed after separating the left and right hilum, to allow for side-specific portal triad clamping. In our patients, laparoscopic left liver resection was performed using left HVO, which benefited from its anatomical superiority or an easy division of the left hepatic artery and portal branch, with good results and minimal bleeding. The left portal branch is comparably easy to expose because of the clear hilar anatomy of the left liver relative to the right portal branch. Therefore, HVO is the most appropriate blood flow occlusion method for left hepatic removal.
In our study laparoscopic right liver resection was performed using SVO, which benefited from maintaining contralateral hepatic artery blood flow. For laparoscopic right hepatectomy, we exposed the left hepatic artery and maintained hepatic artery blood flow on the left side, with occlusion of the portal vein and right hepatic artery. In this way, the portal circulation can be completely blocked, and right liver tumor resection can be performed; the contralateral liver tissue receives continuing blood supply from the hepatic artery. The theoretical basis of this technique is the liver's blood and oxygen supply; the normal blood supply to the liver is 25%–30% derived from the hepatic artery and 70%–75% derived from the portal vein. Because the hepatic artery has higher pressure, the proportion of oxygenated blood is high, so it supplies 40%–60% of oxygen demand. The portal vein collects blood from the intestinal tract, the liver, and the associated nutritional supply.8,25 The advantages of this method are that it is relatively simple and that blood flow occlusion is complete during liver resection, resulting in reduced blood loss. However, because of the existence of a contralateral hepatic artery blood supply for a short time, the technique will not cause severe ischemia. Compared with the Pringle maneuver, this method can be tolerated for a longer time, but it may also be necessary to block the portal venous system, resulting in intestinal stasis. It can be seen from the results that these three vascular occlusion methods all involve reduced blood loss, yield reliable effects, and are simple and easy to apply. However, the Pringle method requires longer occlusion times and induces more extensive liver damage, especially in cases of liver cirrhosis and other chronic liver disease. This could easily lead to serious liver damage and related complications, and it is therefore better suited to patients with better functional liver reserves and those who require hepatectomy with a short occlusion time.
HVO does not cause intestinal congestion of liver damage and can maintain full flow to one side. It should represent an ideal blocking method for laparoscopic liver resection. 28 In this group, laparoscopic hepatic left lateral lobe resection and left liver resection were performed using this method, resulting in reduced injury to the liver and less bleeding. HVO is particularly suitable for left hepatectomy with portal dissection. However, for patients with right liver resection, because freeing the right hepatic portal branch is complex and time-consuming, right liver resection by exposing the hepatic artery anatomy in combination with occlusion of the right hepatic artery and portal vein is a simple operation, with no significant difference compared with the Pringle maneuver with respect to blood loss or operation time. With less damage to liver function and decreased postoperative complications, SVO is suitable for patients undergoing resection of the right liver lobe who are lacking in functional liver reserves and require extended portal triad clamping.
Footnotes
Disclosure Statement
No competing financial interests exist.