
Abstract
Abstract
Introduction:
Despite the well-documented safety and effectiveness of laparoscopic colorectal surgery in curative intention, the role of conversion and its impact on short- and long-term outcome after resection of a carcinoma are unclear and continue to give rise to controversial discussion.
Methods:
Within the framework of a prospective, multicenter observational study (Laparoscopic Colorectal Surgery Study Group), into which a total of 5,863 patients from 69 hospitals were recruited over a period of 10 years, a subgroup of all patients who had undergone curative resection was analyzed with regard to the effects of conversion.
Results:
Of the 1409 patients who had undergone curative resection for colorectal carcinoma, conversion had to be performed in 80 (5.7%) cases for the most diverse reasons. The duration of surgery (median: 183 vs. 241 minutes; P<.001) was significantly longer in the conversion group. Perioperatively, significant disadvantages were noted in converted patients in terms of intraoperative blood loss (median: 243 vs. 573 mL, P<.001), need for perioperative blood transfusion (10.8% vs. 33.8%; P<.001), and resumption of bowel movement (median: after 3 vs. 4 days; P<.001). With regard to postoperative morbidity, significant disadvantages were observed in converted patients, in particular in terms of specific surgical complications, including a higher rate of anastomotic insufficiency (5.0% vs. 13.8%; P=.003) and a higher reoperation rate (4.9% vs. 15.0%; P=.001). In the long term, conversion was associated with lower overall survival, but not with poorer disease-free survival.
Conclusion:
Significantly higher postoperative morbidity was observed in patients after conversion, in particular in terms of specific surgical complications. In addition, conversion is associated with overall lower survival but not with poorer disease-free survival.
Introduction
Despite the extensive worldwide use of laparoscopic procedures in the meantime and the evidence that these approaches are equivalent for treatment of colorectal carcinoma, as shown in controlled and prospective randomized studies,1–4 minimally invasive resection procedures—in particular in curative intention—continue to give rise to controversial discussion.5,6
One of the primary issues frequently disputed here is the role of conversion, and this discussion continues.7–11 There is uncertainty about the impact of conversion after laparoscopic resection on short-term outcome, and even more so on long-term outcome after curative resection of carcinomas.
The aim of the study was to evaluate the role of conversion, its impact on postoperative morbidity and mortality, and the oncologic and prognostic long-term outcome in patients undergoing curative resection of colorectal carcinoma.
Methods
The present data were prospectively collected within the framework of a multicenter study conducted by the Laparoscopic Colorectal Surgery Study Group, after approval by the institutional review board. A total of 5853 patients from 69 hospitals were recruited between August 1 and March 31, 2005. All patients who had undergone curative resection of colon or rectum carcinoma were retrospectively evaluated in a subgroup analysis.
Each participating hospital bore responsibility for indication, choice of surgical method, and for obtaining their patients' consent to take part in the study. Data collected included age, gender, body mass index (BMI), preoperative findings, perioperative approach, surgical course, histological work-up, complications, and the postoperative course.
After checking for plausibility, data were entered into the database and analyzed by using a database program (SPSS Base 8.0, SPSS Interactive Graphics 8.0, SPSS 17.0.1; SPSS Inc., Chicago, IL).
The Kolmogorov–Smirnov test for normality showed that the majority of the continuous variables significantly deviated from the normal distribution. Therefore, the group differences between the converted and laparoscopic groups were checked for these variables by using the Mann–Whitney U test for significance. Accordingly, the median as well as the minimum and maximum values are given for descriptive purposes. Group differences for categorical data were checked for statistical significance with Fisher's exact test.
The postoperative morbidity was hierarchically tested, that is, to begin with summarized in the complication groups. If a significant finding was noted, then the individual subpoints were tested. Hence, an overall error probability of 5% was assumed for each test.
Follow-up entailed examination of tumors at quarterly intervals during the first 2 years after surgery, at 6-monthly intervals in the next 2 years, and at yearly intervals in the 5th year. All patients who had undergone at least one complete follow-up examination were included in evaluation of 5-year survival. Testing for significance was done with the log-rank test (Mantel-Cox). Kaplan–Meier survival curves showing overall survival and disease-free survival were generated with the database program SPSS Advanced Statistics 8.0 (SPSS 17.0.1; SPSS Inc.).
Results
Overall, 1,409 of the 5,853 patients recruited into the study underwent curative resection of a colorectal carcinoma. For 1,329 patients, it was possible to complete surgery as a laparoscopic or laparoscopically assisted procedure; whereas for the remaining 80 patients, intraoperative conversion to “open” surgery had to be performed, thus corresponding to a 5.7% conversion rate.
Sociographic data showed no significant differences between the two groups with the exception of BMI (25.2 vs. 26.4; P=.001; Table 1).
Bold signifies p < 0.05.
The duration of surgery was significantly higher in the conversion group (180 vs. 232 minutes; P<.001). Tumor-related factors or formation of adhesions were the main reasons for conversion in half of the cases. Conversely, intraoperative injuries to blood vessels, intestines, or the urogenital system were implicated in fewer than 20% of all conversions (Table 2).
However, no significant differences between converted and nonconverted patients in terms of the pathological stage was found (UICC III for laparoscopic resections n=407/1329; 30.8% versus n=28/80; 35.0% for converted patients; P=.454). In addition, in terms of the tumor location, there was no significantly higher rate of rectum tumors in the converted group (rectum carcinoma in laparoscopic resected patients n=569/1329; 42.8% vs. n=39/80; 48.7% in converted patients; P=.298).
With regard to postoperative recovery, significant disadvantages were observed in the conversion group: poorer outcomes were observed in the conversion group in terms of intraoperative blood loss (median 200 vs. 500 mL, P<.001), number of patients requiring blood transfusion (10.8% vs. 33.8%; P<.001), and resumption of bowel movement (median after 3 vs. 4 days; P<.001; Table 1).
Looking at postoperative morbidity, no relevant differences were discerned with regard to the general medical complications. At most, a significant, albeit slight disadvantage was noted in the conversion group for onset of pneumonia (2.0% vs. 6.3%). There was more robust evidence of this difference in investigating specific surgical complications: for virtually all parameters, significant advantages were observed in the patient group for whom the entire procedure had been laparoscopically conducted; such parameters included, for example, anastomotic insufficiency rate (5.0% vs. 13.8%; P=.003), onset of postoperative impaired passage (disrupted peristalsis) persisting for 3 days (2.6% vs. 8.8%; P=.008) or occurrence of wound healing disorders (10.4% vs. 20.0%; P=.016), and a trend toward bleeding or abscess formation (4.9% vs. 10.0%; P=.060). With regard to the reoperation rate (4.9% vs. 15.0%; P=.001), this was also significantly higher in converted patients (Table 3).
Bold signifies p < 0.05.
DVT, deep vein thrombosis; UTI, urinary tract infection.
Conversely, only a slight significant difference was seen in postoperative hospital mortality (1.5% vs. 5.0%; P=.04; Table 3).
With regard to the long-term results (mean follow-up 2.1 years, range 0.3–5.0 years), a significant difference (78.5% vs. 74.3%; P=.028) was observed only in 5-year overall survival (Fig. 1). However, no significant differences were seen for stage-related survival (Fig. 2). The survival curves for disease-free survival (73.3% vs. 74.6%) were virtually identical (Fig. 3).

Overall survival for patients with laparoscopic resection (78.5%) versus converted patients (74.3%); (P=.028).
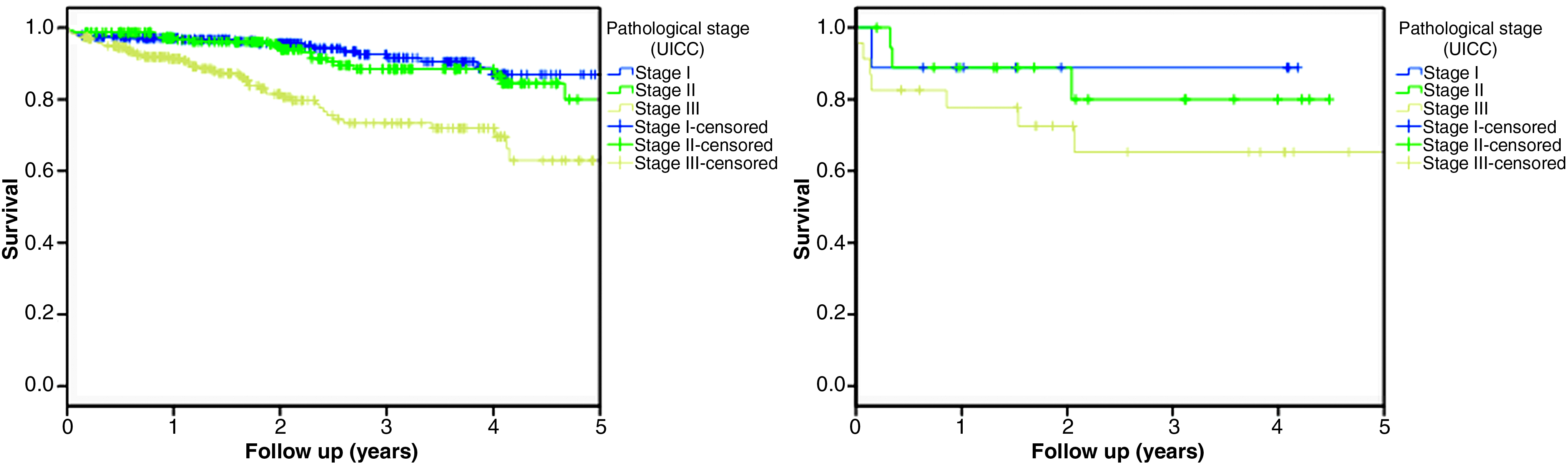
Stage-related overall survival for patients with laparoscopic resection (left) (I:88.8%, II:84.4%, III:66.3%) versus converted patients (right) (I: 88.9%, 80.0%, III: 65.3%).
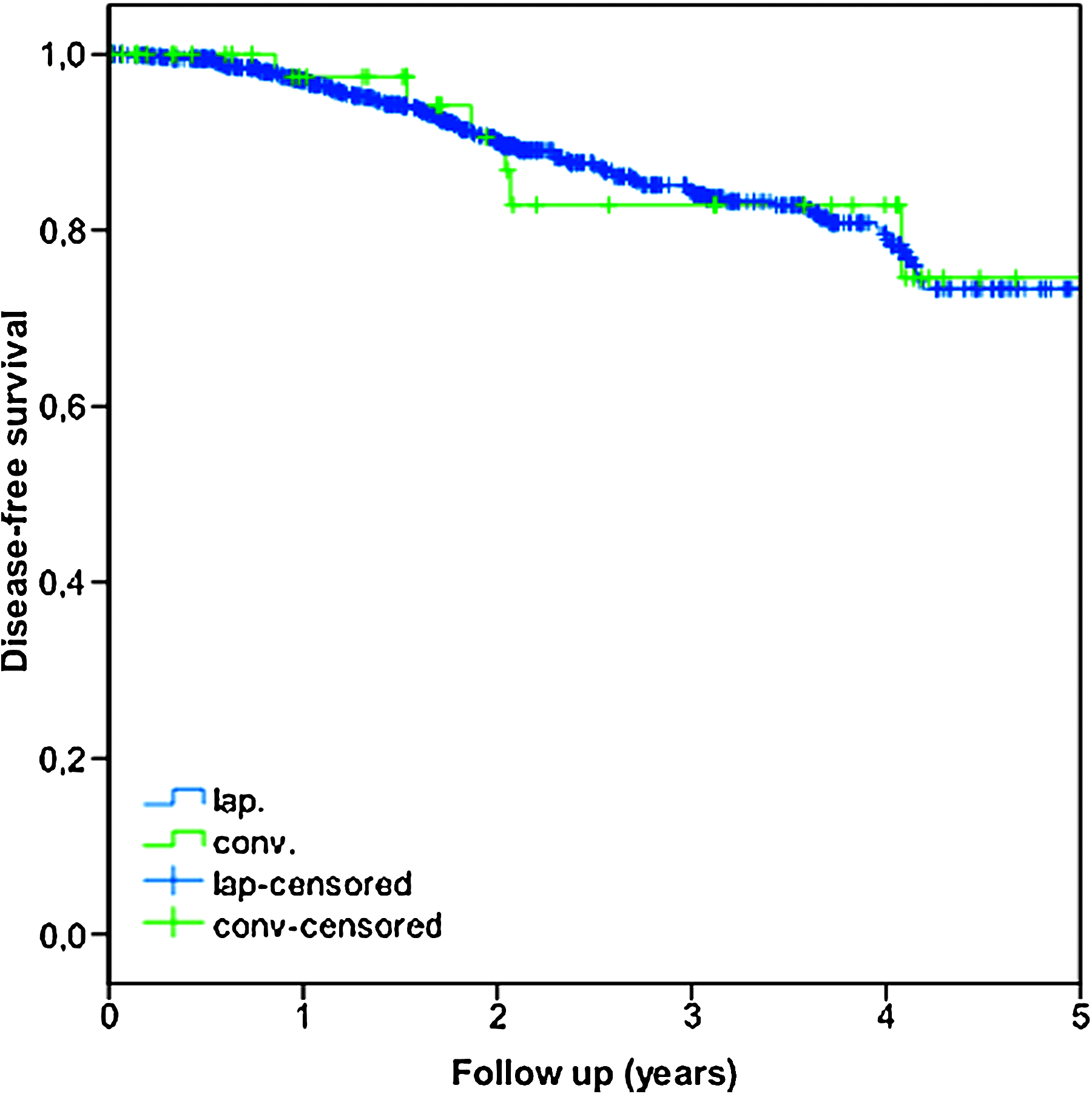
Disease-free survival for patients with laparoscopic resection (73.3%) versus converted patients (74.6%).
Discussion
The role of conversion and resultant consequences are decisive for classification of the possible advantages of laparoscopic colorectal surgery. Conversion is viewed in a critical light in terms of prognosis, in particular when evaluating curative resection of colorectal carcinomas,12,13 despite it not being deemed per se to be a complication. 7 However, in the current literature, there are divergent views of the role of conversion,7,9,10 with some authors stating that converted patients face no disadvantages,3,6,8,11,14–17 whereas other groups of authors believe that there are potential drawbacks in terms of morbidity and mortality2,7,10,11,18,19 or long-term outcome.3,12,13,20
The conversion rate of the 5.7% identified here is somewhat at the lower end of the range of 1.9% to 25% given in the literature for larger patient collectives6,7,12,13,16,19,21 and is not higher than in the case of patients undergoing colorectal resection for a benign indication.6,18,19
The data collected here on the short-term postoperative outcome show a clearly discernible increase in morbidity. Noteworthy is the fact that this increase in the complication rate relates less to general medical complications, having instead more or less selective implications for specific surgical complications, especially risk of anastomotic insufficiency, which in the current study proved to be highly significant; other authors have also shown evidence of this to some extent.2,7,10 There is also, albeit tentative, evidence of a higher risk of re-bleeding. The highly significant increase in the reoperation rate for converted patients completes this picture, showing that overall the postoperative outcome for converted patients should be viewed as being markedly poorer. This clear evidence would seem to suggest that the short-term postoperative outcome is lower than that seen for open surgery, as already described in the direct comparison of open, laparoscopic, and converted groups: on comparison of these three groups, converted patients fared worse in terms of morbidity not only than the laparoscopic group but even worse than patients undergoing open surgery from the outset.2,7
A significant rise in pronounced impaired passage—defined as delayed bowel movement of longer than 3 days—was also noted after conversion (Table 1). Increased wound problems should also be viewed in the same light, which is understandable due to the much larger wound surface and that also has been reported in almost all other studies.2,7,10,11,19,20
Evaluation of long-term outcome revealed a significantly poorer overall survival with identical disease-free survival (Figs. 1, 2, and 3). This was exactly the same finding as uncovered within the framework of the CLASSICC trial, a prospective randomized study published a few months ago. 3 Jayne et al. 3 attributed this phenomenon to the fact that conversion, and hence its associated adverse effects, is performed not only for reasons related to the tumor but also for other reasons (obesity, technical reasons, intraoperative complications, etc.); this is a fact that also holds true for the current study (Table 2). Our findings did not support the second possible explanation related to age, as no significant age differences were noted between the two groups (Table 1).
In the current study, conversion was performed in almost half of the cases because of adhesions or for tumor-related reasons, whereas intraoperative complications (injury to blood vessels, ureter, or intestines) were implicated only in 17.5% of the cases. This concords to a large extent with a number of studies in which intraoperative complications occurred in only between 5% and 16% of cases, whereas conversion because of adhesions or for tumor-related reasons ranging from 40% to 66% was markedly more common.1,11–15,19,20 However, this appears to suggest that, in principle, a decision in favor of conversion can be taken in the majority of cases at an early, and, thus, relatively favorable, time point. 11
The conversion rates given in the literature for colorectal surgery are between 2% and 35%;7,16,22 hence, our conversion rate of 5.7% for the comparatively large patient collective tends to be at the lower end. This broad spectrum is no doubt imputable to the fact that, so far, there is no adequate definition for the phenomenon of conversion.7,16,21,22 The findings from the literature to date on the issue of conversion during laparoscopic surgery suggest that it constitutes a very heterogeneous intraoperative problem from which no reliable general conclusions can be drawn and is difficult to compare. Inevitably, conversion in the early stage of laparoscopy will have less impact on the perioperative course than when performed after occurrence of a serious intraoperative complication;17,19 hence, one conversion is not similar to another conversion! In a recent publication, Yang et al. postulated as core message “… preemptive conversion is associated with a better outcome than reactive conversion.” 11 However, to date, there are no, or very few, more clear-cut classifications or precise definitions.7,22 For that reason and based on the findings of the present analysis compared with the current literature, we propose the classification outlined next (Table 4). The applicability and practicability of such a classification should, however, still be evaluated.
Footnotes
Disclosure statement
No competing financial interests exist.