
Abstract
Abstract
Background:
Recent technological developments and improved endoscopic procedures have greatly enlarged the applications of laparoscopic pancreatic resection.
Patient and Methods:
A 77-year-old female with invasive ductal cancer of the pancreatic body touching the common hepatic and splenic arteries underwent a pure laparoscopic distal pancreatectomy with en bloc celiac axis resection (DP-CAR). The celiac axis, the celiac plexus and ganglions, the left gastric artery, the Gerota fascia, the left adrenal gland, and the retroperitoneal fat tissues above the left renal vein were removed en bloc.
Results:
The procedure took 245 minutes and there was minimal blood loss. The postoperative course was uneventful and the patient was discharged on the seventh postoperative day. The surgical margins were histologically clear (R0 resection).
Conclusion:
Pure laparoscopic DP-CAR is minimally invasive, safe and feasible, and can achieve R0 resection in selected patients with pancreatic invasive ductal adenocarcinoma.
Introduction
Patient and Methods
A 77-year-old female with invasive ductal cancer of the pancreatic body touching the common hepatic and splenic arteries was referred to us for surgical treatment. The patient was placed in a supine position with her legs apart. Trocars were placed on the same sites as are used for laparoscopic pancreaticoduodenectomy.5,6 A 12-mm trocar was placed via the umbilicus, through which carbondioxide gas was delivered. The pneumoperitoneum was controlled electronically to a pressure of 10 mmHg. Another 4 trocars were located on the left lumbar quadrant (12 mm), right lumbar quadrant (5 mm), left midclavicular subcostal line (5 mm), and right midclavicular subcostal line (5 mm). The gastrocolic ligament was divided and the omental bursa was then opened. The dissection was performed along the superior surface of the pancreas to isolate the common hepatic, proper hepatic, and gastroduodenal arteries. After separating the pancreas neck from the portal vein, the pancreas was transected with a laparoscopic stapler close to the gastroduodenal artery (Fig. 1). The common hepatic artery was too adherent to be separated from the pancreas. Despite temporary clamping of the common hepatic artery, pulsation of the proper hepatic artery could be visualized (Fig. 2). The common hepatic artery was tied and divided (Fig. 3). After dividing the splenic vein with a laparoscopic stapler, dissection of the nerve plexus around the superior mesenteric artery proceeded to the celiac axis (Fig. 4). The celiac axis, which was sutured and divided, the celiac plexus and ganglions, the left gastric artery, the Gerota fascia, the left adrenal gland, and the retroperitoneal fat tissues bearing lymph nodes above the left renal vein were removed en bloc (Fig. 5). The specimen was placed in a plastic endobag, and extracted through a navel incision, which was extended to 3 cm. A drainage tube was left near the pancreatic stump.
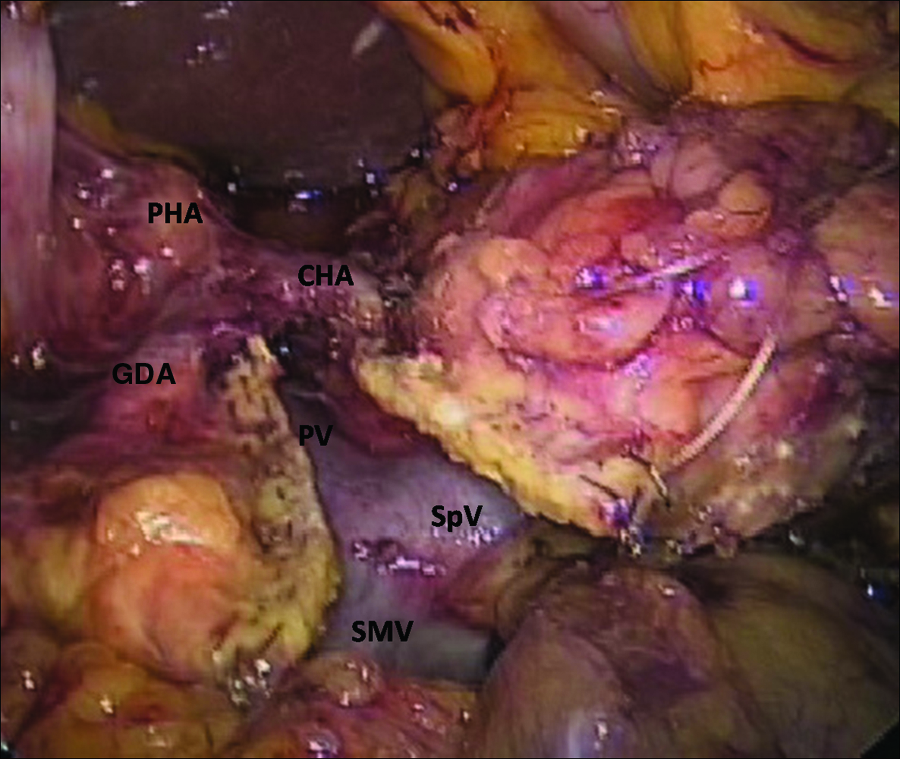
Transaction of the pancreas using a laparoscopic stapler. PHA, proper hepatic artery; GDA, gastroduodenal artery; CHA, common hepatic artery; SMV, superior mesenteric vein; SpV, splenic vein; PV, portal vein.
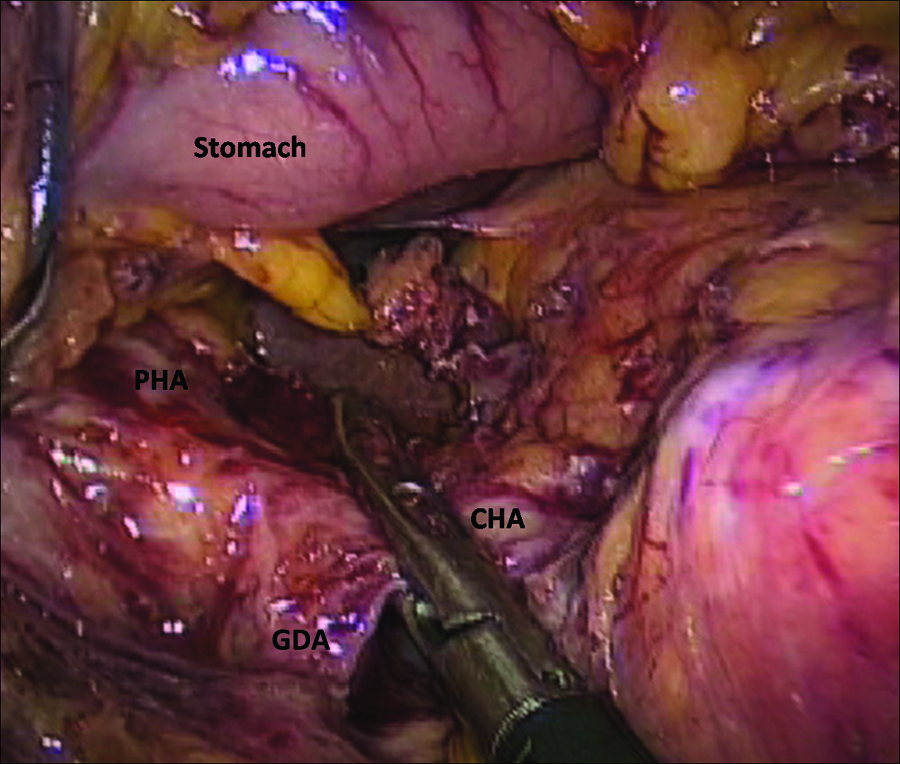
Temporary clamping of the common hepatic artery using a laparoscopic vascular clamp.

The common hepatic artery was tied and divided. SMA, superior mesenteric artery.
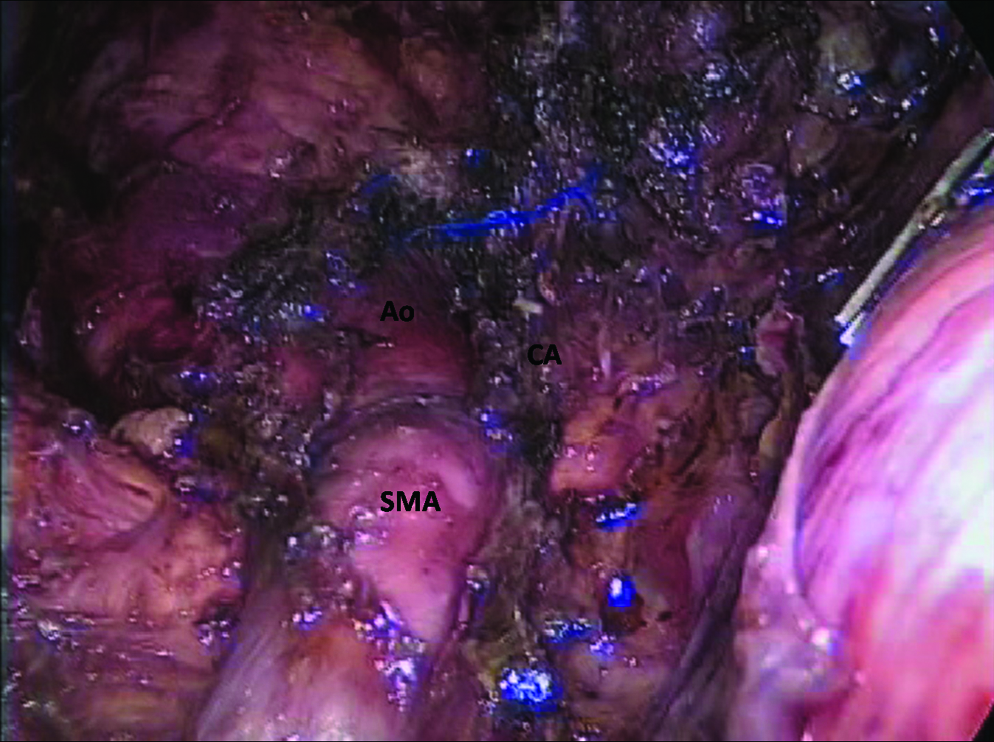
Dissection of the nerve plexus around the superior mesenteric artery. CA, celiac axis.
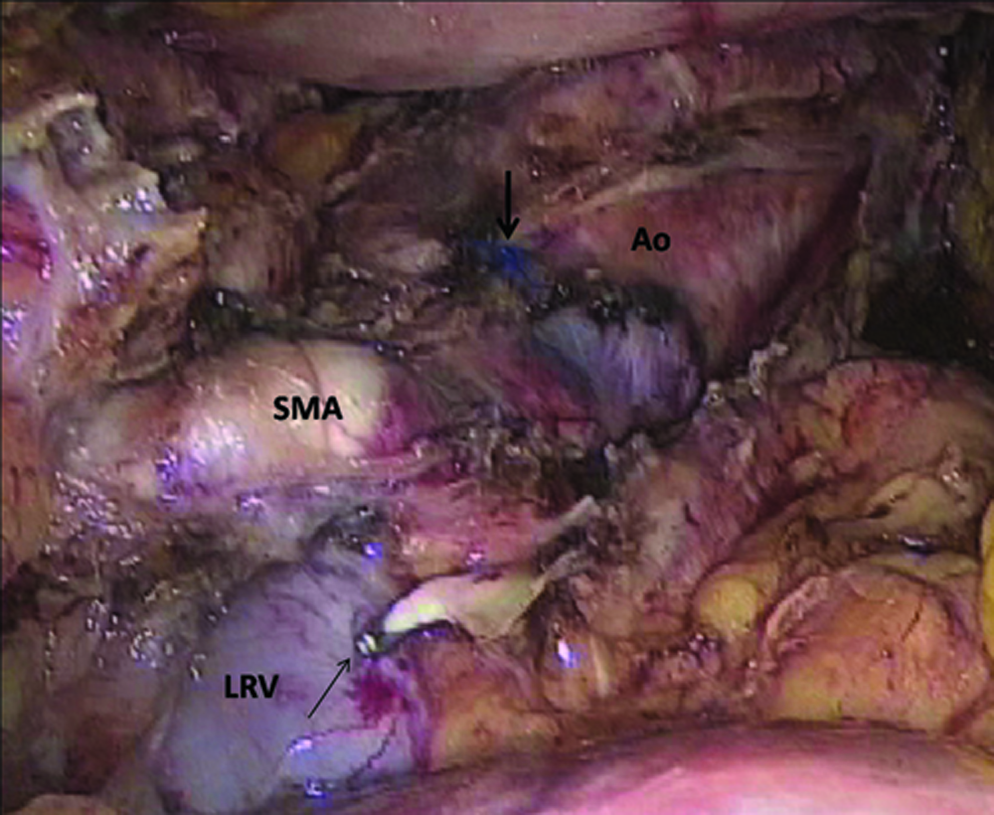
En bloc resection of the celiac axis, the celiac plexus and ganglions, the left gastric artery, the Gerota fascia, the left adrenal gland, and the retroperitoneal fat tissues bearing lymph nodes above the left renal vein (LRV). The stump of the celiac axis was sutured (thick arrow) and the left adrenal vein was clipped (thin arrow).
Results
The procedure took 245 minutes and there was minimal blood loss. The nasogastric tube was removed on the following day. Oral intake was initiated on the first postoperative day. The abdominal drainage tube was removed on the fourth postoperative day. The patient was discharged on the seventh postoperative day. A histological examination showed tubular adenocarcinoma, of the moderately differentiated type. Although the tumor had infiltrated to the common hepatic and splenic arteries, the surgical margins, including the retroperitoneum, were histologically clear (R0 resection).
Discussion
Minimally invasive surgery has been widely accepted in many gastrointestinal fields, even for malignancy. However, laparoscopic pancreatic resection for invasive ductal adenocarcinoma is still not universally accepted as an alternative approach for open surgery, and only a limited number of procedures have been reported7–9 because of the difficulty of oncologic resection and a lack of consensus regarding the adequacy of this approach. Kang et al. 8 reported that only bloodless resection and R0 resection were significant prognostic factors in laparoscopic left-sided pancreatic resection for invasive ductal cancer. Therefore, a laparoscopic approach for pancreatic ductal cancer may be adequate if R0 resection can be achieved. DP-CAR can potentially achieve complete local control by en bloc resection of the distal pancreas, together with the entire surrounding structures, especially the nerve plexuses along the common hepatic, celiac, and superior mesenteric arteries. Hirano et al. 3 reported a high R0 resectability rate of 91% and an estimated 5-year survival rate of 42% for patients with locally advanced cancer of the pancreatic body, which is excellent considering the advanced stages of the disease that are generally present in these patients. In the present case, laparoscopic DP-CAR enabled R0 resection in spite of the involvement of the common hepatic artery, and the patient did not develop a pancreatic fistula, and obtained the usual benefits from laparoscopic surgery, such as less pain and a shorter hospital stay. Although our experience is limited and appropriate indications must await future studies, we believe that laparoscopic DP-CAR can be feasible, safe, and effective in highly selected patients. However, the benefits of laparoscopic DP-CAR have yet to be conclusively proven, and careful selection of patients is essential in order to successfully perform this procedure.
Conclusions
This report suggests that pure laparoscopic DP-CAR is safe, feasible, and minimally invasive, and can achieve R0 resection in patients with pancreatic invasive ductal adenocarcinoma. Large, prospective studies will be necessary to determine the benefits and results of this approach over open surgery for pancreatic ductal cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.