
Abstract
Abstract
Background:
Recent developments in laparoscopic and retroperitoneoscopic techniques have modified the treatment of renal and ureteral stones. We present the efficacy and possible adverse complications of laparoscopic pyelolithotomy for the treatment of staghorn stones as an alternative to percutaneous nephrolithotomy (PCNL) in our single-surgeon series.
Patients and Methods:
Thirteen patients (10 males and 3 females) underwent transperitoneal laparoscopic pyelolithotomy for removal of staghorn stones. Mean stone size was 5.1 cm (range, 4–6.5 cm). All patients had large stones in the renal pelvis and several (more than two) calices with extrarenal pelvis.
Results:
Mean operative time was 177 minutes (range, 110–240 minutes), and the mean hospital stay was 4 days (range, 3–7 days). Transfusion was not required in any patient, and open conversion did not happen. Overall success rate was 84.6% (11/13), and 2 patients had residual stones that were managed with extracorporeal shockwave lithotripsy. There were no major complications (bleeding, sepsis, bowel injury, or urinary leakage).
Conclusion:
The role of laparoscopic kidney stone surgery has not been defined well, but laparoscopic transperitoneal pyelolithotomy may be performed with proper results and negligible complications in skillful hands. It could be a suitable alternative to PCNL for the treatment of staghorn stones in selected cases.
Introduction
Patients and Methods
From June 2008 to August 2010, 37 patients underwent laparoscopic transperitoneal pyelolithotomy. Of those, 13 patients (10 males and 3 females) had staghorn renal calculi. Preoperative evaluation included taking the clinical history, physical examination, urine analysis and culture, serum creatinine and hemoglobin, intravenous pyelography or computerized tomography (CT) scan, and renal ultrasonography. The contralateral kidney was normal in 11 patients, 1 patient had poor function, and 1 patient had a nonfunctional kidney according to the kidney appearance on CT scan (Fig. 1). An inclusion criterion was large renal stones in the renal pelvis and several (more than two) calices with extrarenal pelvis. Patients with multiple (more than five) renal stones were excluded from this study because of the possibility of stone spillage during washing the renal pelvis. Prophylactic antibiotic was administered on the day of surgery. After general anesthesia, the patient was positioned in the modified lateral decubitus with minimal flexion. A 10-mm camera port was inserted in the umbilicus by open access. Three 5-mm working ports were inserted under direct vision in the midline, 10 cm above the umbilicus, in the midclavicular line parallel to the umbilicus, and 5 cm below the umbilicus lateral to the rectus muscle. The white line of Toldt was incised, and the colon was medially reflected. The pelvis and ureter were identified, the renal pedicle was exposed, and then the renal pelvis was freed from surrounding peripelvic fat. The pyelotomy incision was made by electrocautery on the renal pelvis and extended from the superior to inferior calyx with scissors (Fig. 2), cautiously to prevent excessive pelvis tearing. The tip of the pelvic stone was freed from the ureteropelvic junction (Fig. 3), and then the stone was extracted with a curve grasper and Babcock grasper. Additional stones were removed, and the pyelocalyceal system was washed out with normal saline. A ureteral stent was inserted (Fig. 4), and the edge of the incision line on the renal pelvis was re-approximated using 4-0 Vicryl (Ethicon, Inc., Johnson & Johnson, Somerville, NJ) suture according to the running fashion. The stones were extracted from the abdominal cavity using a surgical glove (Fig. 5). Flexible nephroscopy was not performed at the end of the operation for detection of residual stones.

Preoperative non-contrast computerized tomography scan revealed a staghorn stone in a patient with a solitary kidney.

The pyelothomy incision was made by electrocautery on the renal pelvis and extended from the superior to inferior calyx with scissors.

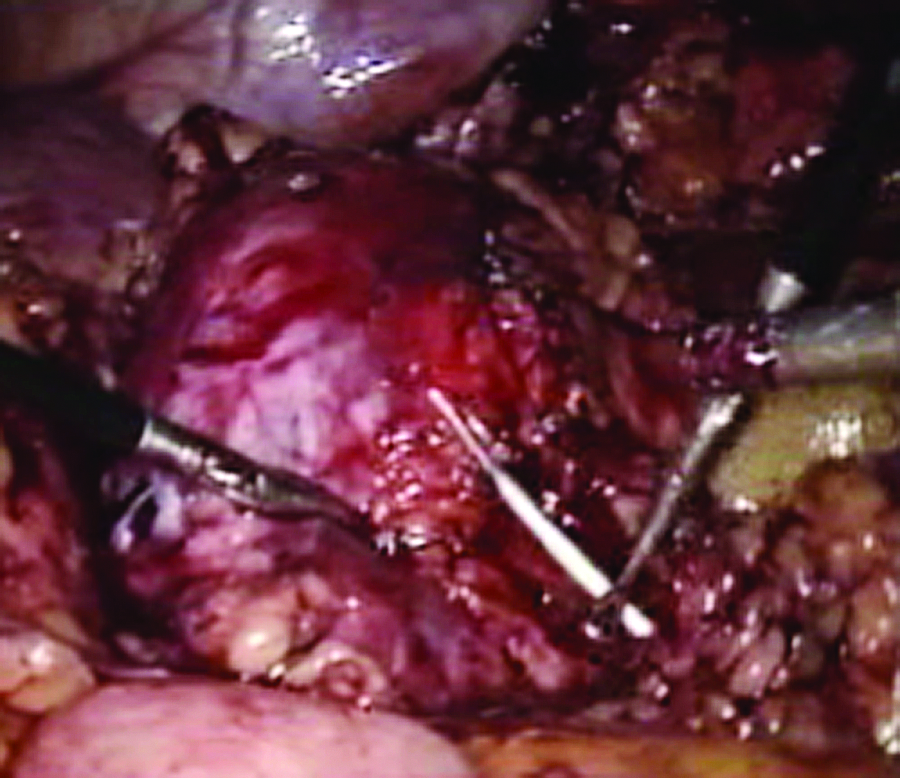
The tip of the pelvic stone was freed from the ureteropelvic junction, and then the stone was extracted with the curve grasper and Babcock grasper.
Additional stones were removed, the pyelocalyceal system was washed out with normal saline, and then the ureteral stent was inserted.

The staghorn stone was extracted from the abdominal cavity using a surgical glove.
The drain was fixed in the peritoneal cavity near the operative field and was subsequently removed 3–5 days after the operation. The Foley catheter was retained for 5–7 days. The ureteral stent was removed 1 month after the surgery. The assessment of residual stones was performed by using plain abdominal radiography 1 day after the operation. All patients were followed up by non-contrast CT scan in the next 2 weeks after the operation.
Results
Thirteen patients with a mean age of 39 years (range, 19–61 years old) successfully underwent laparoscopic pyelolithotomy for the management of staghorn renal stones. The main symptoms were flank pain in 10 cases, urinary tract infection in 2 cases, and accidental finding in 1 patient. Staghorn stones were detected on the left side in 7 cases and on the right side in 6 others. Five patients had a history of previous PCNL or open procedure for managing renal calculi in the same side. The average stone size was 5.1 cm (range, 4–6.5 cm). The main stone was always localized at the pelvis. Table 1 shows demographic data of the patients.
All patients were ambulatory in the first postoperative day and resumed work in 2 weeks. Transfusion was not required in any patient, and open conversion did not happen. Mean operative time was 177 minutes (range, 110–240 minutes), and mean hospital stay was 4 days (range, 3–7 days).
Overall success rate was 84.6% (11/13), and 2 patients had residual stones 8 and 10 mm in diameter, respectively, that were managed with SWL. Six patients had low-grade fever (temperature <38.5°C) for less than 48 hours that was treated by antibiotic therapy. One patient had a collection in the suprarenal area that was managed conservatively and subsided in a few days. There were no major complications, including bleeding, sepsis, bowel injury, and urinary leakage.
Discussion
Staghorn calculi are branched stones that occupy a large portion of the collecting system. Typically, they fill the renal pelvis and branch into several or all of the calices. The management of staghorn calculi includes SWL monotherapy, PCNL monotherapy, combination of PCNL and SWL, and open surgery. Treatment results in SWL depend on stone location, composition, and total stone burden. Stone-free rate with SWL ranges between 45% and 99%, but passage of multiple fragments would create some difficulties for the patients.13–15 Although a single open surgical procedure may be a suitable option in the short term for stone clearance, future stone removal will be compromised because of the extensive scar tissue formation; thus, the American Urological Association guideline has recommended that PCNL should be the first line of treatment for staghorn stones, even though the stone-free rate using PCNL alone in this method was 73%. 16 Patients with large or multiple stones in different calices might need several access sites for PCNL, and these multiple punctures may be associated with an increased risk of hemorrhage. 17 Complete stone particle extraction of staghorn stones may not be possible in one session in a few cases, and hence re-operation is inevitable; the selection of the technique for en bloc removal of these stones perhaps reduces the danger of this disadvantage. The advent of the laparoscopic stone removal procedure has provided the urologist with another means to circumvent current stone surgeries, so using this technique with negligible bleeding and no parenchymal damage in patients with staghorn stones may be an alternative in management of these stones, especially in high-risk patients such as patients with a solitary kidney.
The laparoscopic approach has been performed for ureteropelvic junction obstruction and concomitant pelvic renal stones and in patients harboring stones in poorly functioning polar areas or with nonfunctioning kidneys and pelvic kidneys containing a large stone volume with noticeable results. 18 Although the majority of horseshoe kidneys can be treated with PCNL or ureteroscopy or a combination of these modalities, laparoscopic pyelolithotomy may be an appropriate option in certain cases, and different laparoscopic approaches to these patients have been reported.2–9 Harmon et al. 3 described the first laparoscopic pyelolithotomy in a pelvic kidney.
Gaur 2 originally reported laparoscopic pyelolithotomy using a retroperitoneal approach. Gaur et al. 8 reported a success rate of only 62.5% in 8 patients who underwent the laparoscopic retroperitoneoscopic procedure and the occurrence of conversion to open in 2 patients. It seems that this high failure rate was attributable to a lack of experience and the deep learning curve of this approach. Later, Gaur et al. 10 performed a new technique of retroperitoneal laparoscopic pyelolithotomy using balloon dilatation of the retroperitoneal cavity for the management of staghorn stones in 3 patients; they revealed the feasibility of the retroperitoneal laparoscopic approach for the treatment of a selected group of patients with staghorn calculi in whom any existing minimally invasive technique had failed.
Nambirajan et al. 9 performed four transperitoneal and one retroperitoneal pyelolithotomies. Three of these cases were complicated by urinary obstruction necessitating pigtail-catheter drainage of the kidney, and finally they concluded that laparoscopy is effective for renal stones and that it allows adjunctive procedures. Meria et al. 19 compared 16 patients undergoing laparoscopic pyelolithotomy for a single pelvic stone of over 20 mm in diameter with 16 similar patients undergoing PCNL, although only 1 patient had anomalous renal anatomy. In the laparoscopic group, 2 patients developed urinary leakage, 2 patients required open conversion, and 1 patient had stone fragments that could not be removed; in the PCNL group, 3 patients had bleeding (without transfusion). There was no difference between the two groups regarding the characteristics of patients, stone-free rate, and hospital stay, but the operative time was significantly longer in the laparoscopic group (129 versus 75 minutes).
Ramakumar et al. 20 presented their experience of pyelolithotomy and ureteropelvic junction repair in 19 patients with 3- and 12-month stone-free rates of 90% and 80%, respectively. Srivastava et al. 21 demonstrated the outcome in 20 patients who had undergone transperitoneal laparoscopic dismembered pyeloplasty and concomitant pyelolithotomy; complete stone clearance was possible in 75% of cases. Salvadó et al. 22 performed laparoscopic pyelolithotomy in 9 patients with a large stone in the pelvis and multiple stones in peripheral calices. Average stone size was 2.9 cm. The mean operative time was 176 minutes, and the mean hospital stay was 3.7 days. No major complication was observed, and the overall stone-free rate was 100%. The stone-free rate of laparoscopic transperitoneal pyelolithotomy in our experience was comparable to the previous series8,17,23,24 irrespective of stone size (84% versus 62%–90%), but the mean stone size (5.1 cm) distinguished this study from the previous reports.
Simforoosh et al. 11 performed laparoscopic anatrophic nephrolithotomy for managing staghorn stones in 5 patients. The mean stone size was 53 mm (range, 45–65 mm). They had no blood transfusion, no urine leakage, and no change to open conversion. The mean hospital stay was 5.4 days. Only one 8-mm stone and one 6-mm residual stone remained in the first and the third patients, respectively; both of them were subsequently treated with SWL. Even though this technique was accompanied by a better postoperative period and cosmetic appearance, the renal function impairment is still a major concern after anatrophic nephrolithotomy.
The current study shows our experience for the management of staghorn renal calculi in 13 patients by using laparoscopic pyelolithotomy. The study has revealed that this procedure can be performed with no major complications and acceptable success rate even in patients with previous history of open or PCNL operations and patients with a solitary kidney, although proper case selection and skillful surgeons are the mainstay of stone removal in this manner. We excluded patients with multiple stones in this study and examined the appearance of stones in preoperative CT scan and estimated the residual fragments extracted from the kidney during surgery according to the preoperative imaging. We accept that if flexible nephroscopy was used at the end of the operation for detection of residual stones, the stone-free rate would be higher than our result, but we think that flexible nephroscopy is a time-consuming procedure and requires constant irrigation of fluid in the kidney and abdominal cavity in the transperitoneal approach. The renal stone burden, the number of branches, the adhesion of these branches to the parenchyma, and the position of the renal pelvis (complete intrarenal pelvis with insignificant hydronephrosis may be a dilemma for this technique) can influence the possibility of performance and the outcome of this approach for staghorn stones; therefore, it may not be a suitable alternative to PCNL in all cases.
Conclusion
The role of laparoscopic kidney stone surgery has not been defined well, but laparoscopic transperitoneal pyelolithotomy may be performed with acceptable results and negligible complications in skillful hands. Further evaluation is necessary, and a randomized clinical study is required to confirm the real role of this approach for managing staghorn stones.
Footnotes
Disclosure Statement
No competing financial interests exist.