
Abstract
Abstract
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) has recently become more common, and the challenge of managing neonatal cases is increasing. Meanwhile, there have been reported intraoperative complications or conversion to open surgery due to injury of herniated viscera and inability of organ reduction. We used the endoscopic surgical spacer SECUREA™ (Hogy Medical Co., Ltd., Tokyo, Japan), which is an elliptical sponge made of polyurethane with a radiopaque marker, for preventing these complications in three cases of CDH. The first case was a late presentation in a 10-month-old girl, and the second and third cases were prenatally diagnosed female neonates without severe pulmonary hypertension. All cases were left-sided hernias without sacs. At operation, the SECUREA was grasped using forceps, and the viscera were pushed back gently to avoid injuring the spleen or the short gastric vessels in the second and the third case. The SECUREA was intended to prevent intestinal injury during defect repair in all cases, with placement of the SECUREA between the edge of the diaphragm and the reduced intestine. The procedures in all patients were completed with no complications and without the need for conversion.
Introduction
Intestinal perforation, bleeding from the short gastric vein, and inability to reduce the herniated organs during thoracoscopic repair of CDH have been reported as intraoperative complications or causes of conversion to open surgery.3–5 Technical improvements to resolve these issues are essential to increase the safety of thoracoscopic repair of CDH. We used SECUREA™ (Hogy Medical Co., Ltd., Tokyo, Japan) endoscopic surgical spacers (Fig. 1) 6 in three cases of CDH, resulting in safe reduction of the herniated viscera and repair of the hernia orifice.

The endoscopic surgical spacer SECUREA. This sponge device is made of polyurethane with a radiopaque marker.
Case Report
The first case was a late presentation in a 10-month-old girl, and the second and third cases were prenatally diagnosed female neonates without severe pulmonary hypertension. All cases were left-sided hernias without sacs. For the thoracoscopic approach, the patient was placed in the right lateral decubitus position, and surgery was performed using three trocars. The first 5-mm trocar was placed in the mid-axillary line in the fourth intercostal space. Another 5-mm trocar was used for the second port and inserted below the tip of the scapula. The third port used a 3- or 5-mm trocar placed in the fifth intercostal space below the nipple. The first or second trocar was used for the thoracoscope (5 mm, 45°). The initial insufflation pressure was 4 mm Hg. A SECUREA spacer was inserted directly through the incision for the 5-mm trocar after temporary removal of the trocar.
In the first case, the small intestine and the right-sided colon were herniated, and these viscera were reduced using nontraumatic forceps, without grasping. The diaphragm defect was 4 cm×2 cm. The SECUREA was placed between the edge of the diaphragm and the reduced intestine during defect repair, to prevent intestinal injury (Fig. 2). The defect in this case was repaired without the need for a patch.
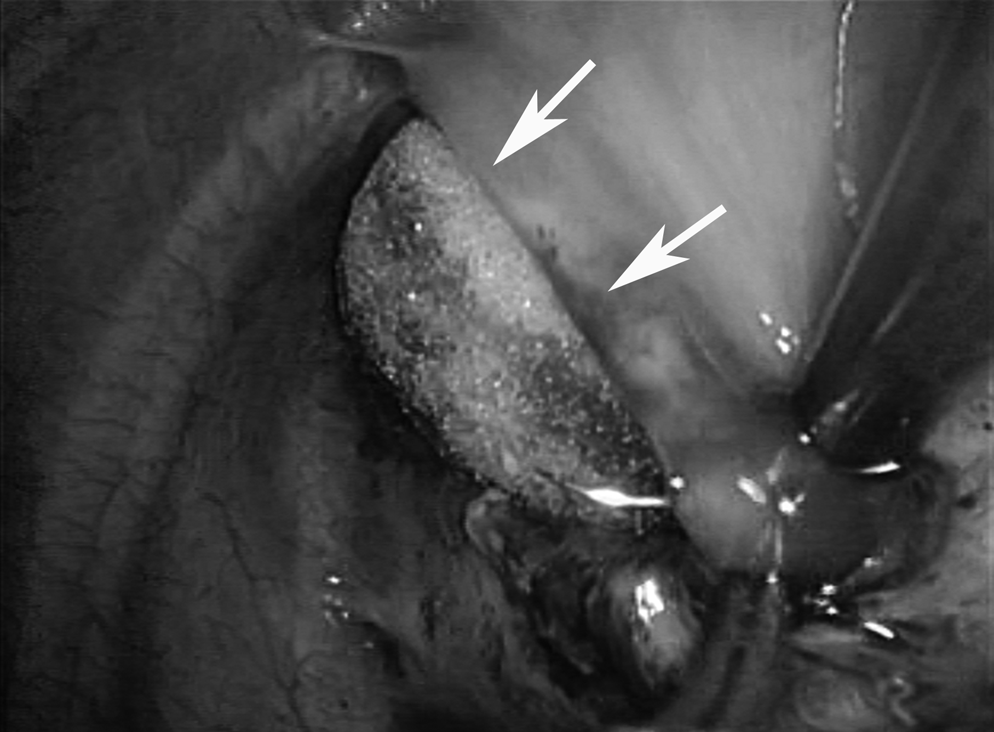
The SECUREA was placed between the edge of the diaphragm (white arrows) and the reduced intestine to prevent intestinal injury during defect repair.
In the second and third cases, the spleen, the small intestine, and the right-sided colon were herniated. The SECUREA was grasped using forceps, and the viscera were pushed back gently to avoid injuring the spleen or the short gastric vessels (Fig. 3). The hernia orifice was 4 cm×4 cm in the second case and 3 cm×2 cm in the third case. The SECUREA was also applied during defect repair, as in the first case. Primary closure without a patch was performed in the third case, but a partial patch was required in the second case. The procedures in all patients were completed with no complications and without the need for conversion.

Safe splenic reduction using a SECUREA. White arrows delineate the defect of the diaphragm. Spl, spleen.
Discussion
The endoscopic surgical spacer SECUREA is an elliptical, easily collapsed sponge made of polyurethane with a radiopaque marker. 6 It measures 4.0 cm×2.5 cm×1.5 cm (extra small size) and can be introduced into the body cavity through a 10-mm trocar or into the wound created for a 5-mm trocar. At placement and removal, the radiopaque marker needs to be grasped with forceps to guide the sponge. The SECUREA spacer is resistant to the heat and vibration that emanate from endoscopic energy devices. It was developed (1) to permit the use of forceps to safely exclude organs and tissues from the surgical field, (2) to prevent secondary injuries caused by the use of surgical instruments, and (3) to prevent the spread and facilitate the removal of exudate or blood, in place of gauze. SECUREA spacers can be restored to their original state by aspirating the absorbed content, and there is therefore no need for replacement.
The thoracoscopic repair of CDH is associated with relatively high conversion rates, ranging from 3.4% to 37.5%,3,4,7–9 with irreducibility or injury of herniated viscera during reduction being cited as causes of conversion.4,5 The liver and spleen are often herniated and can easily be damaged by endoscopic forceps during mobilization. The development of a safe reduction procedure could thus play an important role in improving the conversion rate. Use of a SECUREA allowed us to mobilize the organs using the soft surface, without grasping the organs, facilitating the reduction of the spleen in the second and third cases. Reduced organs sometimes return to the thoracic cavity and interfere with the repair of the diaphragmatic defect, thus increasing the risk of injuring the organs with the suture needle. In all three cases presented here, the safe repair of the defect was aided by placing a SECUREA spacer between the edge of the diaphragm and the reduced intestine. A SECUREA was left in the abdominal cavity until the last stitch was placed on this occasion and then removed to the pleural space around the ligation.
We have used the spacer only in left-sided cases with a relatively small defect in this series. In cases with a larger defect, extra small-sized SECUREA spacers might be too small for safety repair. There are two more different-sized SECUREA spacers: The small size measures 5.0 cm×3.0 cm×1.5 cm and can be introduced through a 10-mm trocar, whereas the medium size measures 6.0 cm×3.5 cm×2.0 cm and can be introduced through a 12-mm trocar, and these devices would be helpful for large diaphragmatic defects. Regarding right-sided hernias, this sponge can be expected to work especially for preventing liver injury.
In conclusion, SECUREA spacers could represent useful devices for allowing the safe thoracoscopic repair of CDH. However, further clinical studies are needed to confirm the efficacy of this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.