
Abstract
Abstract
Introduction:
Improvement in laparoscopic skills requires practicing, and it is mostly beneficial when live animal models are considered for use. Apart from pelvic trainer, dogs and rabbits are used as the animal models for training laparoscopic surgeries at our center. Every effort is made to keep the animals alive after surgery.
Materials and Methods:
From January 2007 to January 2010, German shepherd dogs and Angora rabbits were selected as the animal models for laparoscopic skill training. Under general anesthesia, trainees performed several laparoscopic surgeries under the supervision of experienced surgeons.
Results:
A total number of 72 animals including 54 dogs and 18 rabbits were used for training laparoscopy. In total, some 107 different laparoscopic procedures were performed by trainees including nephrectomy, nephropexy, vesicotomy and vesicorrhaphy, vasectomies, spermatic cord ligation, and unilateral oophrectomy. There were one vascular and two visceral injuries in the rabbit model that were laparoscopically controlled, and conversion to open surgery happened in one case due to the failure in extracting the specimen from the abdominal cavity. Three visceral and six vascular injuries occurred in the canine model. Total mortality was five including three rabbits and two dogs.
Conclusions:
The sacrifice of the animal is important to be avoided from both ethical and technical stand points. Dogs and rabbits are good models for laparoscopic training in urology, and it is possible to keep the animals alive after surgery by close monitoring. We also found the rabbit to be a good model for practicing infantile laparoscopic surgery, as it simulates the real surgery in this difficult age group.
Introduction
Patients and Methods
From January 2007 to January 2010, we held seven laparoscopic training workshops using the animal models for general urologists to improve their laparoscopic skills. On average, 5 trainees participated in each course. Likewise, we designed a scheduled training program for our fellows and residents from January 2009. This program encompasses laparoscopic animal operations and practice on pelvic trainers once a week. The 3-day crush courses during workshops included didactic lecture sessions on practical points of laparoscopy and specific laparoscopic surgeries with stress on our country and the prevalent regional diseases, supervised practice on the pelvic trainer (locally designed and domestically patented), and 2 to 4 laparoscopic surgeries on the animal models (German shepherd dogs and Angora rabbits). The characteristics of the animals have been listed in Table 1.
We used abattoir materials including chicken thighs for practicing the tissue handling, cutting, and suturing in the pelvic trainer before proceeding to the laparoscopic surgery on the animal. Our animal facility works under the national regulations for working on the laboratory animals (Pasteur institute of Iran) 5 compatible with Institutional Animal Care and Use Committee guideline. 6 The animal use protocol included regulations for transportation, housing, environment, husbandry, personnel training and safety, and hazard prevention measures, which had been approved by the national research ethics committee. The operations were performed by trainees under the close supervision of the experienced surgeons and attending veterinarian. Trainees also attended the hospital operating room to observe live human laparoscopic surgery performed by experienced laparoscopic surgeons.
Animals were transferred from the laboratory animal institute to our center by an experienced veterinarian and his team on the day of the surgery. Preoperative preparation consisted of ensuring the animals' health through physical examination by the veterinarian; 12-hour and 6-hour fasting periods for dogs and rabbits, respectively; and an intravenous catheter fixation for intra-operative fluid and drug administration. A preoperative single dose of the intravenous antibiotics (ceftriaxone 1000 and 100 mg, and gentamicin 80 and 8 mg, for dogs and rabbits, respectively) was administered. Sedatives were administered 30–40 minutes before anesthesia induction. Acepromazine (acetylpromizine, 0.03–0.1 mg/kg), which is a phenothiazine derivative, and xylazine (0.5–1 mg/kg), an α2 sympathetic agonist, were intramuscularly injected (IM) for dogs, whereas xylazine (4–6 mg/kg) was administered for rabbits. Atropine (0.22 mg/kg, IM) was used to reduce the oropharyngeal secretions, prevention of bradycardia, and for its synergistic depressant effect on the central nervous system. General anesthesia was induced by using a combination of intravenous Ketamin (6.6–11 mg/kg and 35–40 mg/kg, for dogs and rabbits, respectively) and the inhalation of halothane gas. After orotracheal and nasogastric intubation, animals were attached to the ventilator apparatus. Vital signs were closely monitored during the operation. After positioning the animals to the right flank and securing them to the operative table by adhesive tape, animals' abdomens and flanks were thoroughly shaved, prepped, and draped.
Laparoscopic ports were placed in a diamond configuration by using reusable bladed laparoscopic trocars. A 12 mm umbilical trocar for a telescope was inserted by using modified Hasson technique as previously described by Simforoosh et al. (Fig. 1).7,8 A 10 mm lateral working port was inserted above the telescopic port in the flank area under direct laparoscopic view. Two other 5 mm trocars were placed in the subcostal and lower abdomen area along the midclavicular line (Fig. 2). Pneumoperitoneum was established by CO2 with the maximum pressure of 15 mm Hg and the flow rate of 3 L/minute for dogs, and 10 mm Hg and a flow rate of 1.5 L/minute for rabbits.
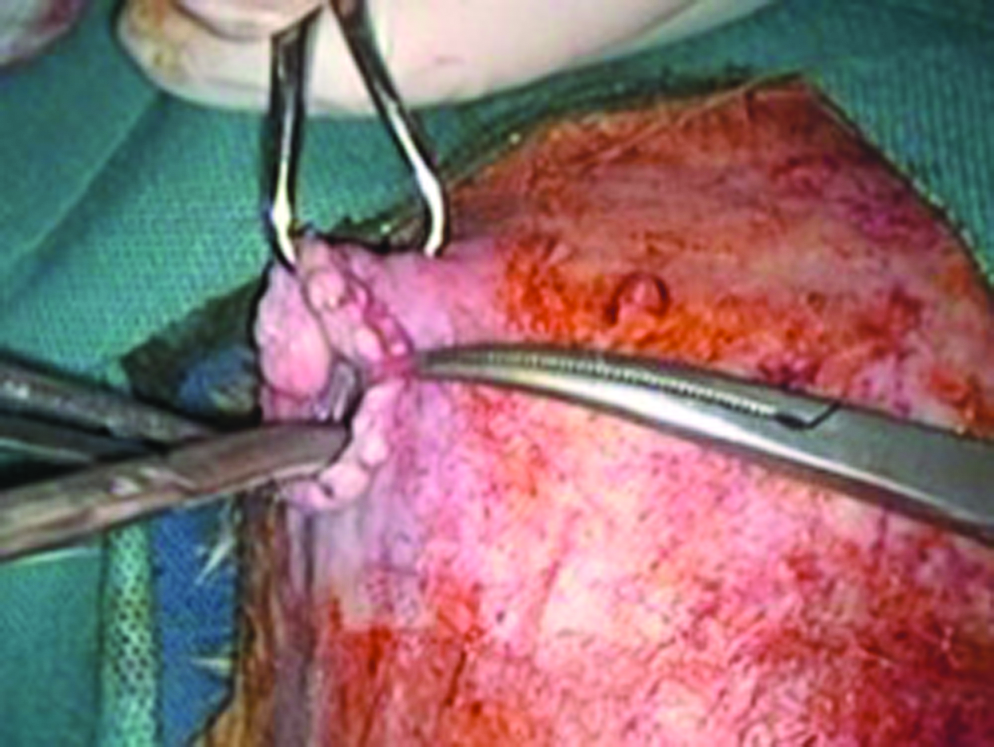
Open access technique for trocar insertion.
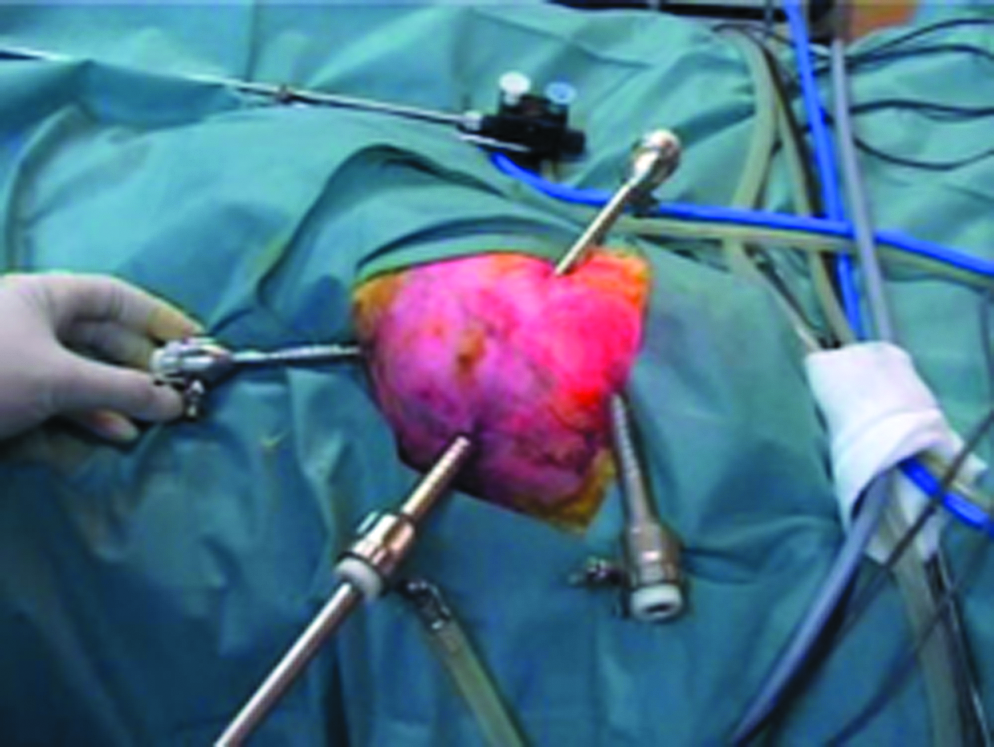
Port placement in the rabbit model for laparoscopic training.
Every effort was made to keep all situations under control, similar to a human laparoscopic surgery (Figs. 3 and 4). Each animal was closely monitored for at least 6 hours after the operation in the recovery room; however, the postprocedural care and observation was tailored on an individual basis. Pain control during recovery and convalescence phase were achieved by using both nonpharmacological and pharmacological methods. The animals were kept in a quiet and dark recovery room with appropriate ambient temperature, and their normal feeding would be started at the end of the recovery period. Nonsteroidal anti-inflammatory drugs (Diclofenac sodium, 2.5 mg/kg bw/day, IM) were used for analgesia, either as a single-agent therapy or combined with opioids (Morphine sulfate, 0.1 mg/kg, IM, every 3–4 hours) as a multimodal analgesia based on the predicted intensity of pain to alleviate the pain and distress of the animal. 9 They were returned to the animal institute for continued care and follow-up during the convalescent period including frequent dressing change and wound maintenance. The operated animals were excluded from any other future experiments and returned to their natural food chain after a normal follow-up visit by the veterinarian in charge 2 weeks after the operation.
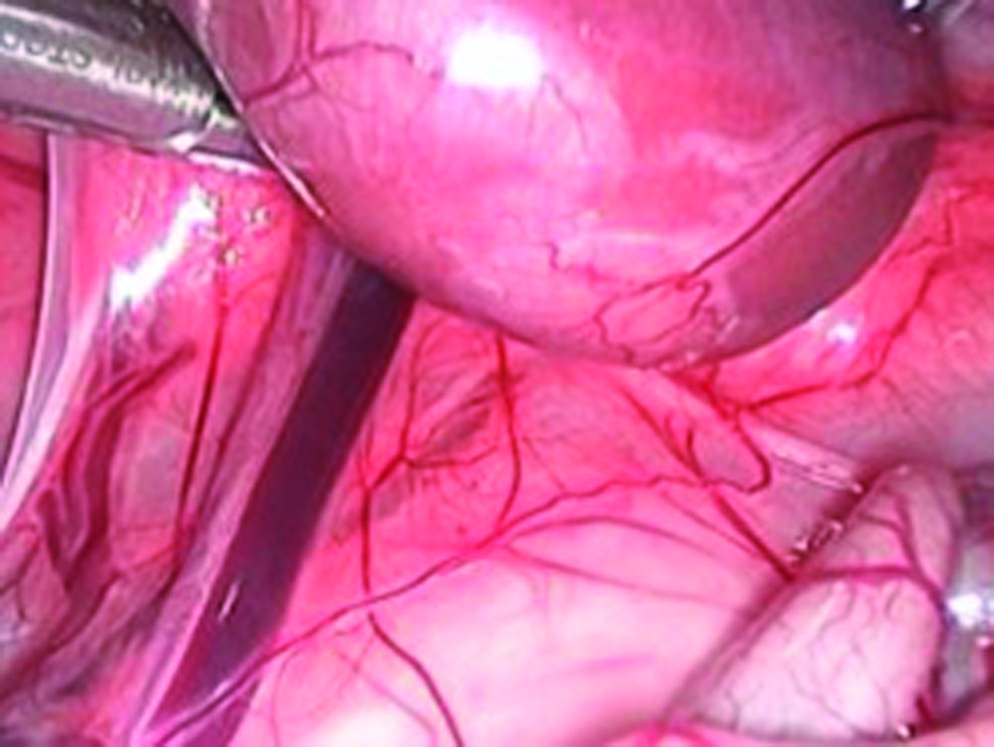
Laparoscopic view of the rabbit kidney.
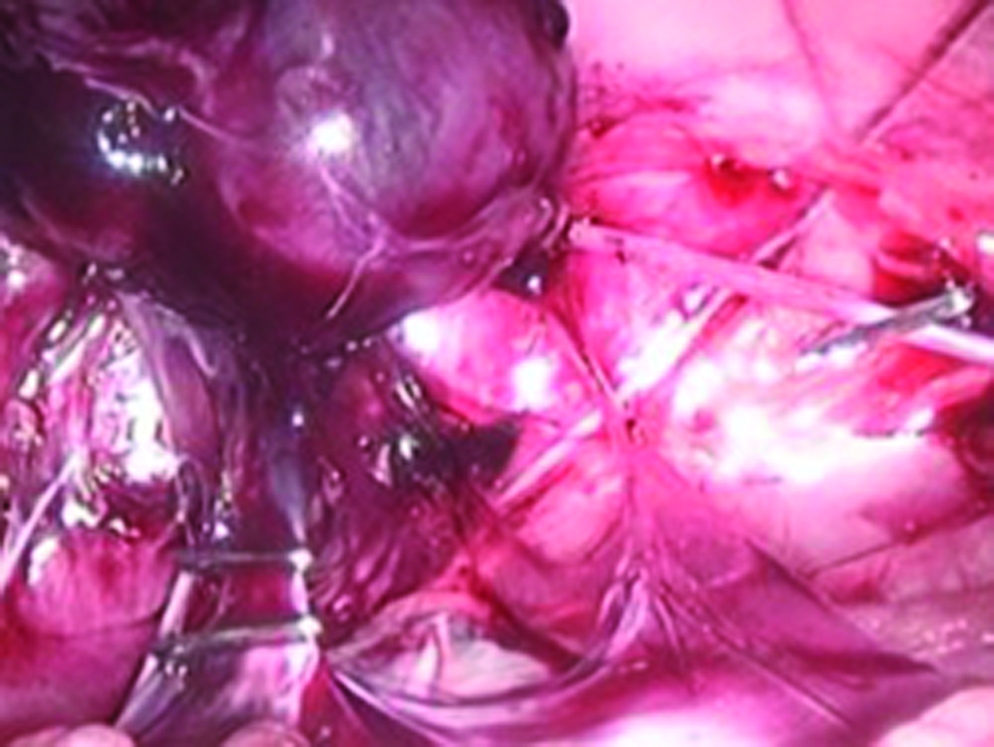
Application of metal clip during rabbit nephrectomy.
Results
During a 3-year period, a total number of 72 animals (54 dogs and 18 rabbits) were included in this study. Trainees performed 107 surgical procedures (detailed information is listed in Table 2). Minor complications that were encountered in the rabbit laparoscopy were mostly related to the ports; including the frequent outward dislocation of the trocar due to the thin abdominal wall and gas leakage around the ports, thus resulting in limiting the working space. There were 2 cases of visceral injuries in the rabbits including 1 case of liver injury which was managed by bipolar cautery and one case of gastric perforation during trocar insertion that was managed by primary laparoscopic repair. Postoperative course of both was uneventful. In addition, there was one case of renal vessel tearing and bleeding in a rabbit when applying the clip that was laparoscopically controlled. The specimen that needed conversion to open surgery for its retrieval was lost in the abdomen in one rabbit surgery. Dogs had less trocar-related problems, but still we secured the trocars to the abdomen to prevent outward slippage of the port in all procedures. Major complications were more frequent among dogs and included 3 cases of small-sized injuries of the bowel that were primarily repaired during laparoscopy, six cases of renal pedicle injury and bleeding which could be laparoscopically controlled in 3 cases, and open conversion in two and unsuccessful bleeding control leading to animal death in one case. One case of the rabbit model and three cases of the dog models underwent conversion from laparoscopy to open surgery (5.5%). One dog and three rabbits had perioperative mortality due to anesthetic problems. The causes of death were supposed to be barotraumas during pneumoperitonum creation and maintenance. The average anesthesia time was 3.5 hours (2.5 to 5 hours), and 2.5 hours (2 to 4 hours) for dogs and rabbits, respectively. Average estimated blood loss was 100 mL (50–1500 mL) for dogs and 20 mL (10–200 mL) for rabbits. During the 2-week follow-up, all animals were healthy.
Discussion
Laparoscopic training with box trainer and animal models are important means for a novice laparoscopic surgeon. They improve the laparoscopic skills, simulate the laparoscopic operation in humans, and provide an excellent platform for learning the basic laparoscopic skills. 10 A direct step from the model to the operating room could be too difficult for a trainee, and that is why the animal model is necessary. Our 3-day training program course consisted of 2-hour lectures followed by 2-hour training on pelvic trainers, and 4-hour laparoscopic surgery on animals during the first 2 days. On the 3rd day, participants attended live human laparoscopic surgery to observe what they had learned in the real setting.
Wolfe et al. 11 described the animal-care protocol for training courses, but they killed the animals at the end (terminal animal). Our strategy to keep the animals alive compelled us to design procedures that improved the participants' skills and likewise to be less traumatic to the animals. We were successful in keeping most animals alive after surgery by using controlled anesthesia and monitoring the vital signs during the surgery, ensuring complete homeostasis during and at the end of the surgery, laparoscopic or open repair of untoward complications as soon as possible, and close observation of the animal in the recovery phase. Avoiding animal sacrifice is not only important from the ethical viewpoint, but it also enables our team to assess the relative postoperative outcome. We think that using this strategy encourages the trainees to work safer and become more familiar with laparoscopic techniques and the proper management of the complications if they occur. Only one case in 5 cases of mortality was related to the surgical technique, and the other four deaths were possibly related to barotraumas in our early experiences; such mortality disappeared after the decline of the pneumoperitoneal pressure threshold.
Chiu et al. 12 and Rassweiler et al. 13 described laparoscopic nephrectomy in the porcine model. Partial nephrectomy was also performed in pigs by McDougall et al. 14 and Barret et al. 15 We did not use a pig as a model in our experience because of its lower availability here; thus, dogs and rabbits were selected as animal models. Although these animals had intraperitoneal urinary tracts, complete mobilization of the kidney needed dissection of the lateral attachments that simulate laparoscopic dissection around the human kidney. Nephropexy is performed by suturing the kidney to the lateral abdominal wall, and this performance is a good model for learning intracorporeal suturing. Securing the pedicel during laparoscopic nephrectomy was achieved by using a clip applier. The extraction of the specimen from the abdominal cavity could be a good model for entrapping the specimen in a retrieving bag. Dissecting the animals' ureter mimicked the human counterpart. However, they had a low caliber, so it could not be a good model for ureteropelvic or ureterouretral anastomosis for novice surgeons. Gonadal vessel dissection, clipping, and transaction are good models for varicocelectomy. The trainees also performed vasectomy and unilateral oophorectomy to reach the acceptable skills for intracorporeal tying and dissection in the pelvic cavity. Making a vesicotomy and then repairing the bladder may be a suitable model for bladder reconstructive surgery.
We described the modified open access for the first trocar insertion that is routinely used in our center.7,8 The trainees also learned and tried this technique in our skill lab, and we had no first trocar complication after the adherence to this technique. Securing the ports to the skin with a nylone suture helped us prevent slippage of the trocars during laparoscopic surgery, especially in the rabbit that has a very thin abdominal wall.
Luks et al. 16 used the rabbit model for gasless laparoscopy to perform standard Nissen fundoplication in 11 animals and left nephrectomy in 7 animals. They concluded that the rabbit can serve as a training model for laparoscopy in the infant. In gasless laparoscopy, using abdominal wall elevation may be particularly useful in very small patients. They used only inhalational anesthesia without intubation and ventilation. We also selected rabbits as animal models for infantile laparoscopy in a more controlled condition by using pneumoperitoneum and successfully performed 16 left nephrectomies. This model simulated the laparoscopy in neonates and infants, despite the difficulties due to thin abdominal wall, small working space, and complications of pneumoperitoneum.
In contrast to terminal animal labs, a “nonterminal” animal lab needs a dedicated veterinarian team to care for the animals in a controlled environment. Although this setting could provide an estimation of the procedural outcome, the cost of this model would be higher than that of a terminal animal lab. Special conditions of urinary tract system in dogs and rabbits made laparoscopic surgery unrealistically straightforward. Further, the results of this study are subjective without any objective evaluation of the improvements in the surgical skills of the trainees.
Despite these limitations, our 3-year experience with a “nonterminal” animal lab justifies this setting in the centers of excellence with fellowship training programs. We plan to run this training model in its advanced level for experienced laparoscopists by adding more difficult procedures including radical prostatectomy, ureteroureterostomy, bowel anastomosis, and enterocystoplasty to our curriculum in the near future. Developing criteria for “technical correctness and improvement” is also necessary for objective assessment of trainees.
Conclusion
The avoidance of animal sacrifice is not only important from the ethical standpoint, but it also enables the trainees to work safer, to prevent complications, and to learn their management in an environment closer to the laparoscopy in humans. The use of dogs and rabbits as animal models for laparoscopic training is feasible, and there are good available operations that both increase the skills of the trainees and save the animals. For infantile laparoscopy, however, the rabbit seems capable of providing a good simulation.
Footnotes
Disclosure Statement
Our skill lab has been established and equipped with the collaboration of Storz Company.