
Abstract
Abstract
Objectives:
To report our initial experience with transvesicoscopic cross-trigonal ureteral reimplantation (TVUR), describing stepwise the surgical procedure and determining critical aspects of this surgery in the actual surgical field.
Subjects and Methods:
Between September 2008 and April 2010, 48 patients with bilateral vesicoureteral reflux (VUR) underwent TVUR. To identify the critical aspects affecting the surgical difficulty, we divided our TVUR procedure into four steps: TVUR set-up, mobilization of ureters, creation of submucosal tunnels, and ureterovesical anastomosis. To evaluate the evolution of our TVUR, we analyzed changes in the operative time and complications versus increase in surgeon experience (dividing our cases into three groups: the first third, the second third, and the last third). Changes in operative time for all four steps of TVUR were analyzed separately, as well as change in overall operative time.
Results:
Of a total of 48 cases, 45 patients underwent TVUR successfully except for 3 cases of open conversion. Among the 45 cases, the mean overall operative time was 155.6 min. In 1 patient, proximal migration of the ureteral catheter occurred. No other perioperative complications were observed. The mean postoperative hospital stay was 1.6 days. The VUR resolution rate was 96.4%. Upon analysis of our results by step, Step 4 (ureterovesical anastomosis) required the largest portion of the overall operative time in most cases. During the early period of our TVUR, we encountered several technical difficulties. However, the operative times for all four steps were stabilized with increasing number of cases, without deteriorating surgical outcomes.
Conclusions:
Our report demonstrates that TVUR might potentially be a safe and effective alternative to open ureteral reimplantation in children with VUR, with a shorter learning curve than expected.
Introduction
Cohen's cross-trigonal ureteral reimplantation 6 is the most widely used technique and is familiar to most urologic surgeons. Recently, transvesicoscopic cross-trigonal ureteral reimplantation (TVUR) under CO2 pneumovesicum was introduced to minimize surgical trauma and serve as an alternative to open Cohen's surgery. Since the initial report, 7 six reports7–12 have been published; these studies have suggested that TVUR can be performed safely and effectively with a high success rate and minimal invasiveness.
However, compared with many other laparoscopic surgeries in the urologic field, information on the technical experience of TVUR remains insufficient. This is probably because of the current status that experiences of this surgery are limited to only a few centers with a relatively small number of patients. It seems that the technique of this surgery has been relatively unfamiliar, even to pediatric urologic surgeons until now. So, we aimed to identify the critical aspects that might affect the surgical difficulty of TVUR and to evaluate the evolution of our procedure during the learning curve of this surgery.
Subjects and Methods
Between September 2008 and April 2010, 48 patients with bilateral VUR underwent TVUR at our institution, all of which were performed by the same surgeon (C.H.H.). Surgical indications included breakthrough urinary tract infections despite antibiotic prophylaxis, persistent VUR after 4–5 years of observation with medical treatment especially in association with significant renal scarring, and/or persistent VUR after endoscopic subureteric injection of bulking agent. Treatment options, including endoscopic management and open/vesicoscopic reimplantation, were discussed with parents (and patients, if possible).
Patient charts were reviewed retrospectively; we collected preoperative, intraoperative, and postoperative data, including age, grade of reflux, operative time, perioperative complications, postoperative hospital stay, and findings from the postoperative ultrasound (US) and voiding cystourethrography (VCUG). Our surgical methods followed those reported by Valla et al. 10 with minor modifications. Operative time was defined as the time from the start of cystoscopy to skin closure. The bladder catheter was kept in place until cessation of hematuria, and patients were discharged without drainage. Follow-up US was performed 1 or 3 months postoperatively, and VCUG was performed at 6 months postoperatively. Success of our procedure was defined as resolution of hydroureteronephrosis on postoperative US and VUR on postoperative VCUG.
To identify the critical aspects affecting the surgical difficulty, we divided our TVUR procedure into four steps: (1) TVUR set-up (including cystoscopy, port placement, bladder wall suspension, and fixation of ureteral catheters), (2) mobilization of ureters (including closure of the detrusor defect), (3) creation of submucosal tunnels (including placement of the ureter in the tunnel), and (4) ureterovesical anastomosis (including closure of the mucosal defect). To evaluate the evolution of our TVUR, we analyzed changes in the operative time and complications versus increase in surgeon experience (dividing our cases into three groups: the first third, the second third, and the last third). Changes in operative time for all four steps of TVUR were analyzed separately, as well as change in overall operative time.
Surgical technique
TVUR set-up (Step 1)
Each patient was placed in the modified lithotomy position with abducted thighs. The bladder was distended with saline for the initial cystoscopic examination. After a small skin incision was made in the midline of the bladder dome, a 5-mm vesicoscopic port (Fig. 1A) was placed into the bladder under cystoscopic guidance. To suspend the bladder wall, a 17-gauge needle was inserted near the camera port and passed into the bladder, and a loop was made inside the bladder. Then a 21-gauge spinal needle was inserted near the camera port into the bladder and passed into the loop, and a 3-0 suture was introduced into the loop through the spinal needle. This suture was trapped by the loop and extracted outside the skin by pulling the loop upward. The suture was then tied at the site of skin incision to fix the anterior bladder wall to the abdomen and was subsequently tied to the trocar. Two ureteral catheters (3 Fr.) were inserted into both orifices, and a urethral Foley catheter was inserted into the bladder. The bladder was emptied and was insufflated with CO2 via the camera port at a pressure of 10 mm Hg and flow of 2 L/min. Two lateral trocars (3 mm) were then introduced through the anterolateral wall of the bladder along the interspinous skin crease (Fig. 1A) under vesicoscopic vision. Bladder wall suspensions around the two lateral trocars were also placed using the same technique described above. We then fixed the ureteral catheters to the ureteral orifice: The ureters were canulated with 3 Fr. ureteral catheters, which were sutured to the bladder mucosa at the inferior edge of the ureteral orifice with a 5-0 monofilament traction suture (by extracorporeal slipping knots). At the knot, a small loop was made. This loop was used in the following (second and third) steps. The ureteral catheter was cut, leaving some distance from the ureteral orifice; the remnant catheter was removed through the urethra. Here, a short segment of the catheter (about 5 cm) was prepared for using to measure the ureteral diameter and the length of submucosal tunnel (in Step 3).

Mobilization of ureters (Step 2)
All successive steps of the classical open Cohen's technique were then reproduced. The ureters were mobilized with hook electrocautery. Mobilization of the ureters was continued until an adequate ureteral length of 2.5–3 cm was obtained. Defects in the detrusor muscle were repaired with 5-0 absorbable sutures using extracorporeal slipping knots. This muscular repair was achieved during traction of the small loop tied on the ureter with the help of a 2-mm Endoclose® device (Tyco Healthcare, USA), which was inserted at the midpoint between the two lateral trocars. At that time, the ureter was attached to the detrusor with one superficial stitch to prevent retraction into the perivesical space.
Creation of submucosal tunnels (Step 3)
We determined the length of submucosal tunnel equal to four times the ureteral diameter. (The diameter of ureter and the length of submucosal tunnel were measured using the segment of remnant ureteral catheter, which was cut after it was fixed to the ureteral orifice in Step 1.) Dissection of the submucosal tunnel was then started from the medial aspect of the ipsilateral ureteral hiatus and advanced to a point above the opposite orifice using 3-mm scissors. After the creation of a submucosal tunnel, a 3-mm grasper was passed, and the ureter was gently drawn through the submucosal tunnel. To pass the other ureter into the lower-part tunnel, we used the loop tied on the ureter to pull it toward the contralateral hiatus. For all patients, the terminal part of the ureter was resected. Then the distal portion of the ureter was fastened to the detrusor muscle with one superficial stitch (by intracorporeal suturing), to prevent its retraction within the submucosal tunnel.
Ureterovesical anastomosis (Step 4)
Ureterovesical anastomosis was performed with intracorporeal suturing using 5-0 monofilament sutures at four points per ureteral orifice. In the case of a nondilated ureter, a ureteral catheter was placed to avoid any obstructive suturing. The mucosal defect of the original orifice was closed with 5-0 absorbable interrupted sutures.
Removal of the instruments and skin closure
After ureteral reimplantation, the working ports and fixation sutures between the bladder and abdominal wall were removed. The skin incision was closed with absorbable subcuticular sutures without bladder port closure. A ureteral stent or drain was not usually used. The bladder catheter was indwelled.
Statistical analysis
Statistical analysis was performed by applying Student's t test and Spearman's rank correlation test. A P value of <.05 was considered statistically significant.
Results
Of a total of 48 cases, 45 patients underwent TVUR successfully in our institution, whereas 3 cases required open conversion. The reasons for open conversion were displacement of the port (cases 2 and 5) and injury of the posterior bladder wall during trocar placement (case 26). Among the 45 cases, mean patient age was 3.7 years (range, 7 months–13 years), and patient age among the three groups (the first, the second, and the last third) was similar (P>.05). Reflux was bilateral in all cases. There were 4 patients who had a duplicated ureter. Of the total of 90 ureters, reflux grade was I in two ureters, II in seven ureters, III in 30 ureters, IV in 31 ureters, and V in 20 ureters. The mean overall operative time of our TVUR procedures was 155.6 min (SD 42.77). The overall operative time decreased significantly with increasing surgeon experience (Spearman's rank correlation coefficient [ρ] −0.56, P<.0001). The mean overall operative times in the first and last third of patients were 190.9 (SD 50.95) and 135.0 (SD 46.95) min, respectively (Table 1). Blood loss was minimal in all cases. Proximal migration of the ureteral catheter occurred in one patient (case 4). No other intraoperative complications were observed. There were only a few (n=4) patients who needed anticholinergic medication for 2–3 days postoperatively. For all other patients, postoperative courses were uneventful. The mean postoperative hospital stay was 1.6 (SD 0.91) days (1 day [n=30], 2 days [n=12], 4 days [n=2], and 5 days [n=1]), which was equal to the mean duration of bladder catheterization. The median follow-up period was 16.3 months; 3 patients were lost to follow-up. No patients showed persistent hydroureteronephrosis on US taken 3 months postoperatively. Three patients (cases 4, 8, and 20) showed unilateral VUR on VCUG at 6 months postoperatively. The postoperative VUR resolution rate was 96.4% (81/84 ureters).
TVUR, transvesicoscopic ureteral reimplantation; V-U, vesicoureteral.
Upon analysis of our results by step, Step 4 (ureterovesical anastomosis) required the largest portion of the overall operative time in most cases (Table 1). The operative times for all four steps decreased significantly with increasing surgeon experience: Spearman's rank correlation coefficient (ρ) −0.47, −0.51, −0.53, and −0.51 for Steps 1, 2, 3, and 4, respectively (P<.001) (Fig. 2).
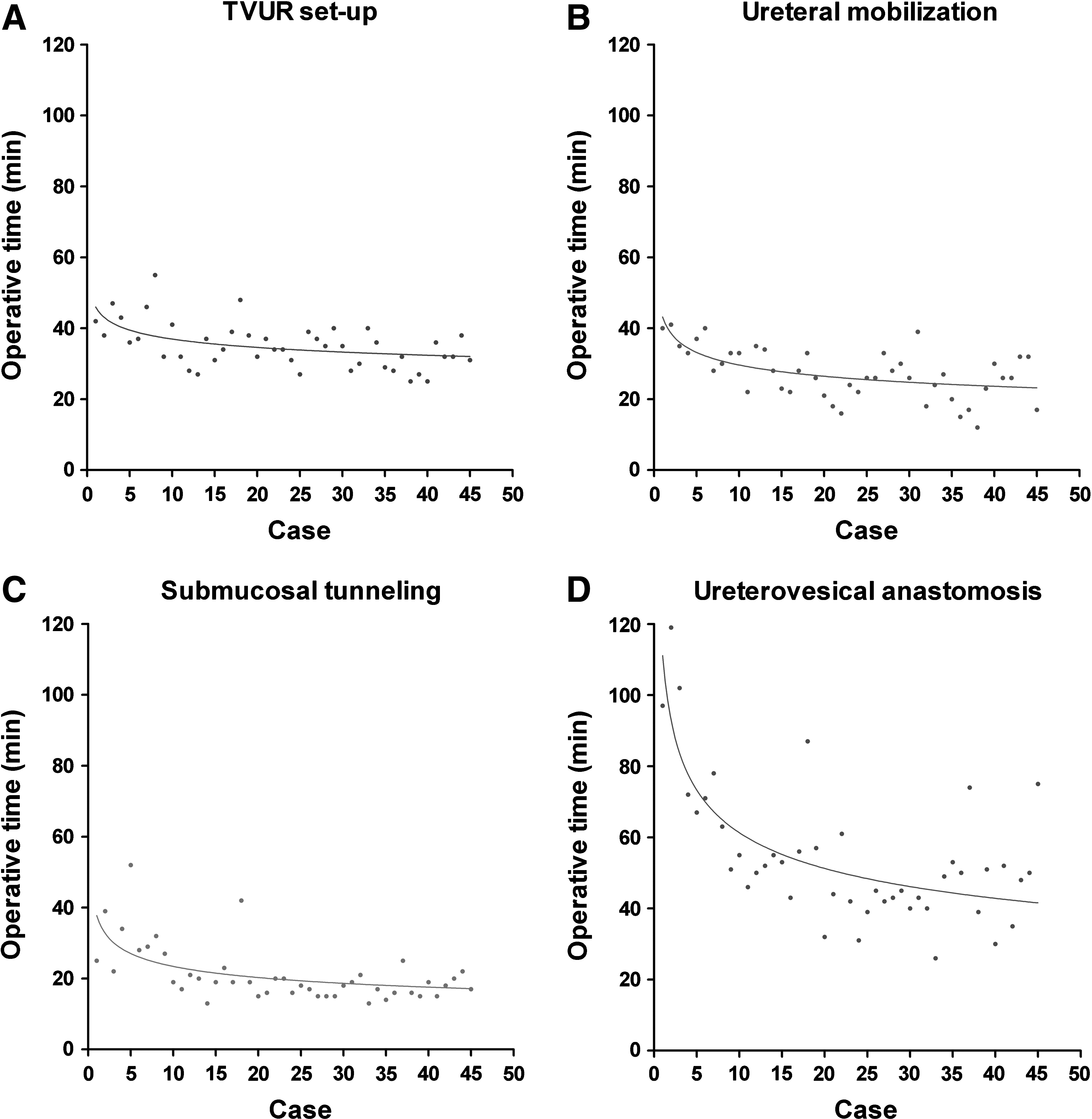
The operative times for each step of transvesicoscopic ureteral reimplantation (TVUR):
Discussion
In our experience, TVUR can be performed safely and effectively and has comparatively low morbidity and fast recovery times. The overall postoperative VUR resolution rate of our TVUR procedures was 96.4%. This success rate is comparable to those reported in other TVUR7–12 series (91%–96%) and those of open ureteral reimplantation13–16 series (96%–98.3%). TVUR is also known to have a rapid recovery time because of reduced bladder trauma and the potential lack of postoperative hematuria and bladder spasm.
Although TVUR has several advantages, it is true that TVUR has been considered a difficult and unfamiliar surgical technique. Its actual role in meeting the theoretical advantages of laparoscopic surgery without deteriorating treatment outcome also seems to be inconclusive.8–11,17 Concerns that the technique might have a steep learning curve8,9 and would be compromised in cases of small bladder capacity8–10 seem to be the main reasons for its limited use.
For a new surgical procedure with limited experience, the learning curve is especially important. Obviously, analysis of the learning curve with a surgical procedure should include surgical difficulty and operative time, as well as the number of complications or surgical outcome. In our experience, a continuous decrease in the overall operative time was observed with increasing numbers of cases. The mean overall operative time in the last third of patients was 135.0 (SD 23.59) min. Comparing the first third with the last third, the mean overall operative time decreased by almost 1 h. In addition to decreasing overall operative time, we became comfortable with performing TVUR after the first third of the cases. Most of our complications occurred during the first third of the cases: There was open conversion in 3 patients (cases 2, 5, and 26), an intraoperative complication (proximal migration of the ureteral catheter) in one patient (case 6), and 3 cases of persistent reflux in three ureters (cases 4, 8, and 20). Thus, our results with TVUR indicate that the learning curve of TVUR may be shorter than expected.
We divided our TVUR procedure into four steps to identify the critical steps affecting the learning curve or level of difficulty of this surgery. For most of our cases, Step 4 (ureterovesical anastomosis) was the major determinant of overall operative time (Table 1) and required a great deal of concentration by the surgeon. Intracorporeal suturing is one of the most difficult and complex laparoscopic tasks. TVUR is an example of urological procedure that relies upon adept suturing skills in a small working space. In the same context, Canon et al. 9 commented that the surgeon's baseline laparoscopic skills and experiences influence the slope of the learning curve for this technique. Although we agree with this, our experience showed that TVUR did not have as long a learning curve than expected: In fact, our surgeon had experiences of laparoscopic renal surgery in adult patients but had not experienced any laparoscopic pediatric reconstructive surgery before performing this surgery (TVUR). Nevertheless, we found that the time required for the fourth step also decreased significantly with an increasing number of cases performed (P<.001) (Fig. 2D), although this step remained the most time-consuming step.
TVUR set-up (Step 1) is the procedure of preparation for ureteral reimplantation. The mean operative time for this step was approximately a quarter of the overall operative time in our experience. The operative time of this step also decreased significantly with increasing surgeon experience (P<.001) (Fig. 2A), as was the case for the anastomosis step. In this step, proper suspension of the bladder wall was important. If this suspension is done incompletely, the bladder port can be displaced from the bladder when the pneumovesicum is deflated, resulting in air leakage. Then this will make the working space smaller, and the subsequent procedures will be disturbed: Among the three open conversions we experienced, two were due to port displacement. For these reasons, we believe that bladder wall suspension is no less important than baseline laparoscopic skills in the initial experience of TVUR, especially for beginners in pediatric transvesicopic procedures.
Step 2 (ureteral mobilization) was performed without difficulty in most cases. In this step, no specific TVUR skills are needed, especially for surgeons who are already skilled in open Cohen's reimplantation. One noticeable aspect in this step was that we made a minor modification during the repair of the bladder floor: When retracting the mobilized ureter during repair of the bladder muscular defect, we used an additional 2-mm puncture grasper inserted at the midpoint of the abdomen. Other methods for retracting the ureter exist; for example, Valla et al. 10 and Kawauchi et al. 11 used a 3-mm device through the urethral route. However, we think that such an approach cannot be used in very young pediatric patients because their urethral diameters are often too narrow to pass the proper equipment for the procedure. Therefore, our technique in this step may be very promising because it can be widely applied, regardless of patient age.
The operative times for Step 3 (submucosal tunneling) occupied the smallest portion of the four steps (Table 1) and also decreased significantly with increasing number of cases (P<.001) (Fig. 2C). Although some authors 17 emphasize the intrinsic problem of submucosal tunneling with TVUR, we think this procedure with TVUR might be easier in some ways than in the open technique. When the instruments move through the lateral trocars with TVUR, the angle between the direction of instrument required for the tunneling and the bladder floor can be less sharp than with the open technique, so submucosal dissection would be easier and more natural with TVUR. From our experience, one crucial aspect in this step is that the lateral trocars should not be placed too close to the orifice. If they are located too far medially, the angle between the direction of the instrument and the bladder floor becomes sharp, making this step difficult (Fig. 1B–D). From our experience, another important factor was that the creation of the lower-part tunnel was a somewhat embarrassing procedure because of its more caudal position relative to the lateral trocars: In creation of the upper-part tunnel, the rigid grasper can move bidirectionally within the tunnel because the direction of the grasper used to create the tunnel and the direction of the tunnel are parallel. Therefore, passing the grasper through the tunnel to the opposite side and grasping and pulling the ureter within the tunnel toward the neo-hiatus were not problematic. On the other hand, during creation of the lower-part tunnel, the movement of the grasper within the tunnel was allowed only unidirectionally because the angle between the direction of the grasper used to pass the tunnel and the direction of the lower-part tunnel is sharp. In our experience, this aspect usually made this step difficult. To enable us to make the safe and effective “separated” submucosal tunnel, we passed “the loop” tied on the ureter through the lower-part tunnel up to the neo-hiatus and then pulled the loop at the neo-hiatus to pass the ureter.
From our analysis of each step, we think TVUR might not be such a difficult or troublesome surgical method. TVUR possibly will be performed effectively with a relatively short learning curve, as long as a surgeon has enough experiences of open Cohen's technique, baseline laparoscopic skills, and knowledge on several particular areas of care described above. In addition, we think that constant self-training of intracorporeal manipulations would be important for a laparoscopically naive surgeon. This can be supported by the fact that studying available video clips allowed our surgeon to become acquainted with the procedure despite the lack of a mentor.
Conclusions
Although technical difficulties and long operative time were encountered during the early period of our TVUR, the operative times for all four steps of our TVUR procedure decreased significantly with increasing numbers of cases. Our results from this study indicate that TVUR appears to be a safe and effective alternative to open ureteral reimplantation in children with VUR, with a shorter learning curve than expected.
Footnotes
Disclosure Statement
No competing financial interests exist.