
Abstract
Abstract
Background:
The aim of the present study was to use a porcine model to compare one- and two-port transvaginal natural orifice transluminal endoscopic surgery (NOTES) with single-port laparoscopic surgery (SPLS) for sentinel node basin dissection.
Study Design:
Three groups (n=3 per group) of healthy female pigs were subjected to lymph node dissection. For hybrid NOTES, an endoscope was inserted via the transvaginal route. For SPLS, a 5-mm 30° telescope with two-port laparoscopic instrument was inserted via the transumbilical port. The three methods were used to dissect the regions of the pig stomach that corresponded to four lymph node areas on the lesser curvature of the anterior wall and greater curvatures in humans.
Results:
For two-port NOTES, SPLS, and one-port NOTES, the overall rates of complete dissection of the lymph node stations were 91.6 %, 83%, and 50%, respectively (P>.05). The mean resected tissue weights were 49.3, 37.9, and 22.5 g, respectively (P=.03). The mean operation times for two-port NOTES (69.9 minutes) and SPLS (68 minutes) were shorter than that for one-port NOTES (99 min) (P>.05).
Conclusion:
Two-port NOTES and SPLS are more feasible than one-port NOTES for sentinel node basin dissection in a porcine model. One-port NOTES is difficult to perform and requires long operation times; however, we foresee this operation as becoming more common in the future.
Introduction
A sentinel node (SN) is defined as the first lymph node to receive lymphatic drainage from the primary cancer; cancer metastasis should therefore occur first in an SN. 13 SN navigation surgery for breast cancer and melanoma has been accepted worldwide and is now an established form of oncological surgery. The SN concept and the lymphatic basin concept have become a focus of attention in recent years. This development is expected to provide a novel diagnostic tool for the identification of clinically undetectable lymph node metastasis in patients with early gastric cancer. 14 Abe et al. 15 reported that a combination of endoscopic submucosal dissection and laparoscopic lymph node dissection enabled the complete resection of the primary tumor and the histological determination of lymph node status. We have extended this surgical concept further in the present study by examining whether the lymph node dissection could be performed with hybrid NOTES or SPLS. We previously reported our study in a porcine model of gastric lymphatic basin dissection for SN biopsy by using NOTES with laparoscopic assistance. 16
The aim of the present porcine model study was to compare the feasibility of one- and two-port NOTES and SPLS for SN basin dissection.
Regarding terminology, we mainly used a laparoscopic device as an energy device even in NOTES animals. We termed this procedure “flexible endoscopic-assisted laparoscopic surgery,” but this term is not commonly used. Instead, we have used here the term “hybrid NOTES.”
Materials and Methods
The protocol was fully approved by Kunkun University Institution Animal Care and Use Committee. Three groups (n=3 per group) of healthy female White Landrace pigs (approximately 60 kg each) were subjected to lymph node dissection. Statistical analysis was performed using PASW Statistics version 18.0 software (IBM Corp., Somers, NY). The data were presented as mean±SD values. The significance of differences was determined using the Kruskal–Wallis test. All statistical tests were two-sided, and a P value of <.05 was considered to be statistically significant.
Operative procedure
Step 1: Preparation
The pigs were admitted to the laboratory 1 week prior to the operation and were allowed water but no food for 24 hours before anesthesia. An intramuscular injection of tiletamine/zolazepam (Zoletil®, Virbac, Fort Worth, TX) (6 mg/kg) and xylazine (Rompun®, Bayer, Leverkusen, Germany) (2 mg/kg) served as a pre-anesthetic. All procedures were performed with the animal under general anesthesia with 1.5%–2% enflurane using 7.0-mm endotracheal intubation. Intravenous access was established via the marginal ear vein.
Step 2: Creation of a pneumoperitoneum, colpotomy, and liver retraction
The anesthetized pig was placed in the supine position. The upper abdomen and the perineal area were disinfected. The vagina was disinfected by using topical iodopovidone. We first made an incision in the periumbilicus. A pneumoperitoneum was created by using the blunt insertion of a 5-mm trocar (designated as () (Auto-suture, Covidien, Norwalk, CT) because the thickness of the pig's abdominal wall makes it difficult to use the Hasson open technique or a Veress needle (Fig. 1). A laparoscopic 5-mm, 30° telescope (Aesculap AG & Co. KG, Tuttligen, Germany) was then inserted into the periumbilical port. The cavity was insufflated with CO2 (6–8 mm Hg of CO2 pressure) through the laparoscopic trocar. A laparoflator was used to control the pressure.
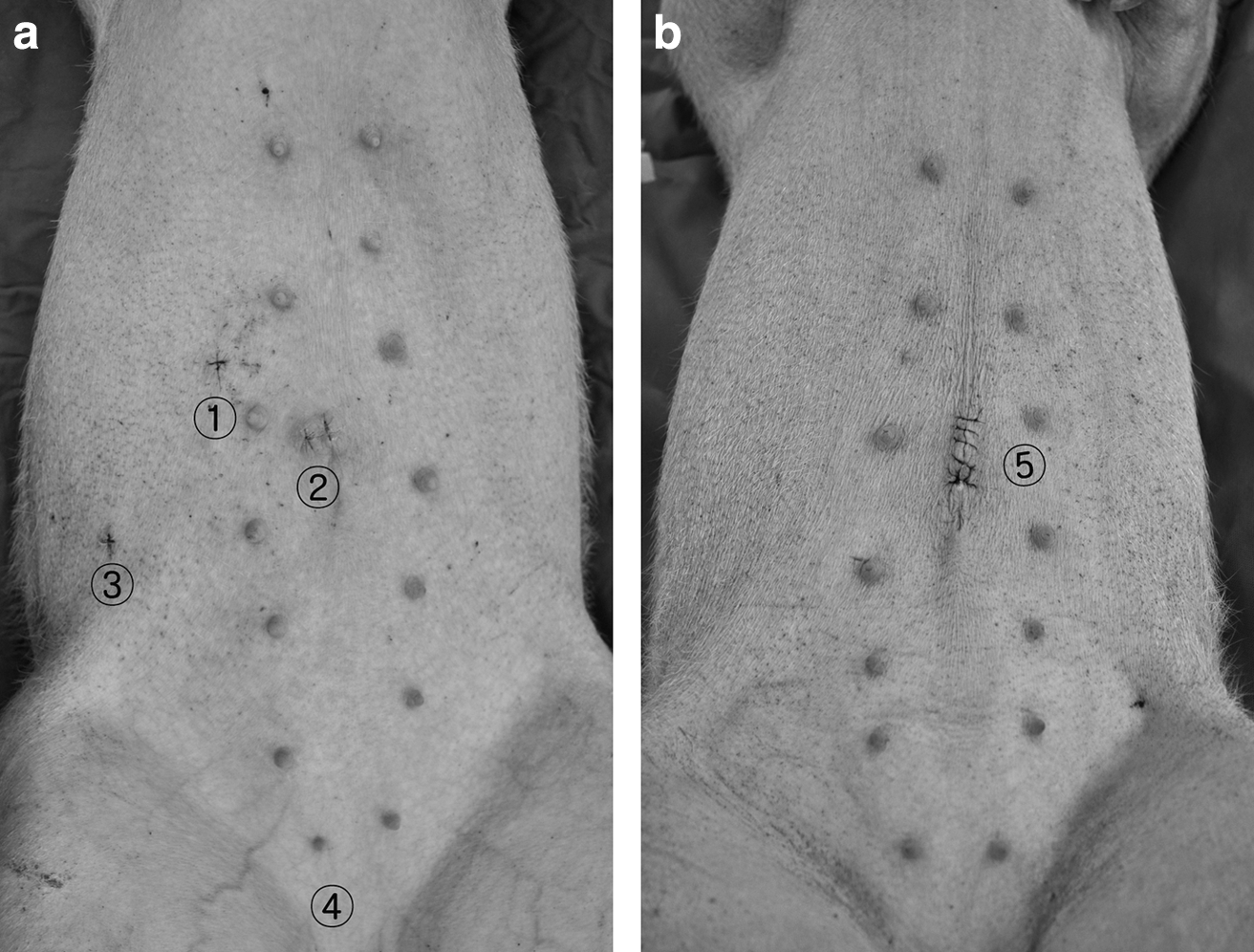
For two-port NOTES, the port sites were the umbilical 5-mm trocar telescope port (designated as (), the upper right port ((), and the right flank port (() for the assisting port (Fig. 1). We used the umbilical port (() and upper right port (() as operating ports during the operation, and the right flank port (() was established because a telescope with one or two assisting ports may be needed for inserting the transvaginal endoscope. However, we did not use the right flank port during the operation, and it will be unnecessary when an experienced gynecologist performs a transvaginal colpotomy in humans. 16 Under laparoscopic observation, transvaginal colpotomy was performed by using a laparoscopic dissector or spatula. To insert the transvaginal endoscope, bladder catheterization with a feeding tube and a Trendelenburg position was necessary. A one- or two-channel endoscope (model GIF-H260 and GIF-2TQ260M, Olympus Co., Ltd., Aomori, Japan) was then inserted into the peritoneal cavity through the incision via the transvaginal route. For one-port NOTES, only the right upper port (() was used for operating, whereas for SPLS, a 2.5-cm-long periumbilical incision was made for the SILS port (US Surgical, Norwalk).
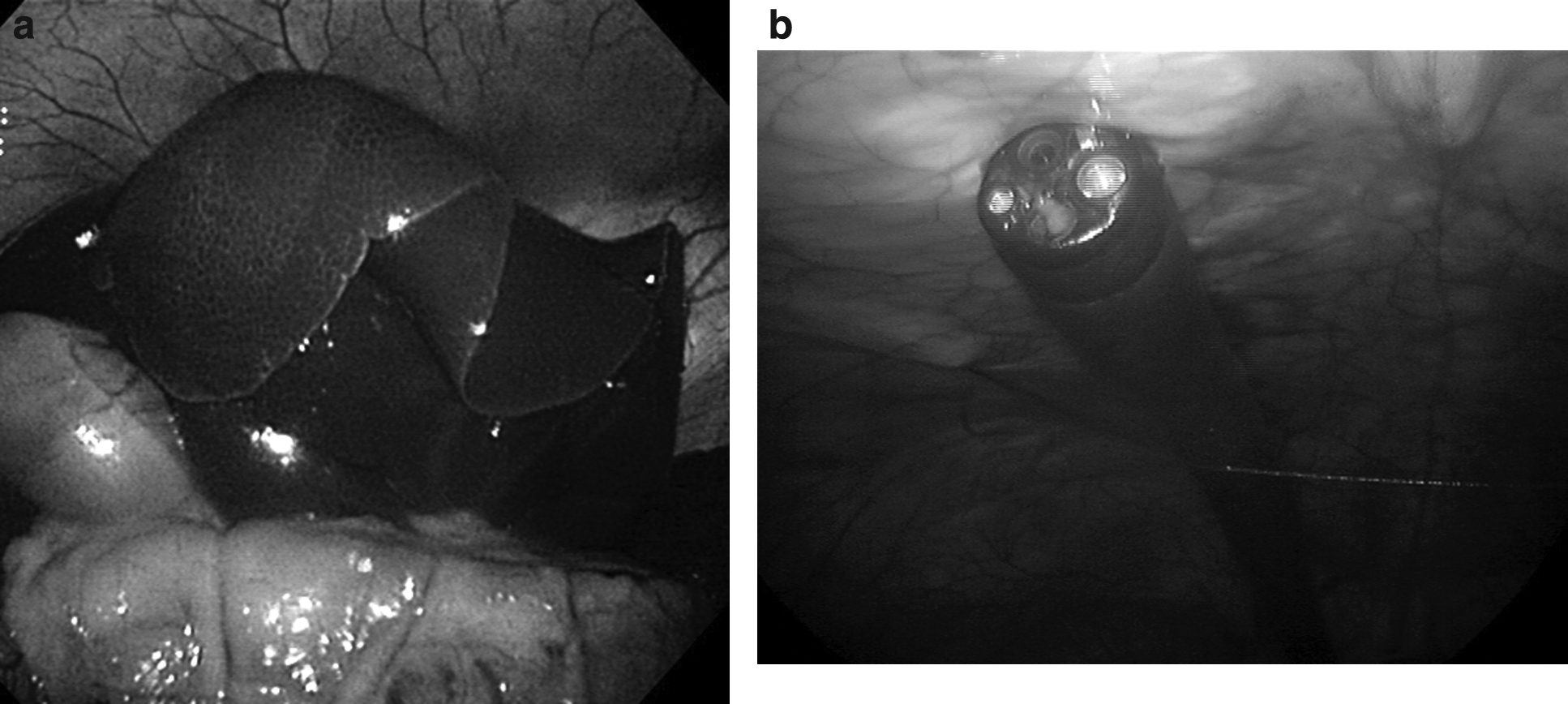
In both pigs and humans, before perigastric dissection can be performed, the liver has to be retracted, which can be problematic. We retracted the multilobulated liver by suturing it with a straight needle (Monosof™ 2-0, US Surgical). 17 For this, we used laparoscopic instruments with one or two ports. On average, 2.2 sutures were needed for liver retraction (Fig. 2a). It was initially difficult to use the multijointed instrument in SPLS during liver retraction. Consequently, the first time liver retraction was performed by SPLS, it took 43 minutes. However, in the second and third pigs, it took less than 10 minutes. Polysorb™ 3-0 (Covidien) was inserted via an endoclosure needle to anchor the endoscope and to present it at an appropriate angle in the lower abdomen (Fig. 2b).
Step 3: Perigastric regional lymph node dissection
One- and two-port NOTES and SPLS were used to dissect the regions of the stomach that correspond to the four lymph node areas found on the lesser curvature of the anterior wall (areas 1&3 and 5) and greater (areas 4 and 6) curvatures in humans (Fig. 3a). In two-port NOTES, the dissection involved transvaginal endoscopy, Sonosurg™ (Olympus), and laparoscopic instruments (Fig. 3b). For one-port NOTES, the dissection involved Sonosurg with an endoscopic grasper (model FG-49L-1, Olympus) or a laparoscopic grasper with an endoscopic needle knife (model KD-1L-1B, Olympus) (Fig. 3c). For SPLS, a 5-mm 30° telescope with a multijointed instrument and Sonosurg were used via the SILS port (Fig. 3d). Two types of multijointed instrument were used: namely, the roticulator type (Endo Roticulator™ Endo Dissect™ or Endo Grasp 5 mm, US Surgical) and the Cambridge-Endo type (Maryland dissector standard or fenestrated alligator grasper 5 mm, Cambridge Endoscopic Devices, Framingham, MA). The rate of overall complete dissection of the lymph node stations was estimated. Complete dissection of the basin was deemed to have occurred when the root of the artery was exposed and ligated. The specimen was removed via the transvaginal route in hybrid NOTES (Fig. 4) and via the umbilical port in SPLS. The resected tissue was weighed, and the operation time was recorded.

Dissection of lymph node areas.

In hybrid NOTES, the specimen was removed via the transvaginal route by using an endoscopic grasper.
Step 4: Postoperative examination
Immediately after the procedure, all of the pigs underwent full laparotomy so that the peritoneal cavity could be examined. The operation site was examined for evidence of hemorrhage, hematoma, or inadvertent organ injury.
Results
Rates of complete perigastric lymph node area dissection
For two-port NOTES, SPLS, and one-port NOTES, the overall complete dissection rates of the lymph node stations were 91.6% (11 out of 12 lymph node areas showed complete dissection), 83% (10/12), and 50% (6/12), respectively (P>.05, Table 1). Thus, two-port NOTES had the highest completion rate, but the difference is not statistically significant. In one case, it was not possible to completely remove lymph node area 4 because it is not easy to expose the root of the left gastro-epiploic area. In SPLS, it was not possible to dissect lymph node area 6 in one pig and area 1&3 in another pig. In one-port NOTES, lymph node area 5 of all three pigs was completely dissected, but areas 1&3 and 4 were dissected incompletely in two pigs, whereas area 6 was dissected incompletely in all three pigs.
Value approaching statistical significance is given in bold.
GC, greater curvature; LC, lesser curvature; LN, lymph node; NOTES, natural orifice transluminal endoscopic surgery; SPLS, single-port laparoscopic surgery.
Resected tissue weights
For two-port NOTES, SPLS, and one-port NOTES, the mean resected tissue weights were significantly different (49.3 g, 37.9 g, and 22.5 g, respectively) (P=.03). However, the mean weights of the greater curvature areas for two-port NOTES, SPLS, and one-port NOTES (41.8 g, 34.1 g, and 18.6 g, respectively) and the mean weight of lesser curvature areas (7.5 g, 3.8 g, and 3.9 g) were not significantly different (P>.05).
Operation times
The mean total dissection times were shorter for two-port NOTES (69 minutes) and SPLS (68 minutes) than for one-port NOTES (99 minutes) (P>.05). Dissection of the lesser curvature areas took 15 and 13.3 minutes for two-port NOTES and SPLS, respectively, whereas it took 29 minutes for one-port NOTES. Similarly, dissection of the greater curvature areas took 54.3 and 54.7 minutes for two-port NOTES and SPLS, respectively, whereas one-port NOTES took 70 minutes (P>.05).
Intraoperative and postoperative complications
There was one case of bladder injury during transvaginal endoscope insertion in one-port NOTES and one case of stomach perforation during tissue resection of area 1&3 in SPLS. Full laparotomy and examination of the peritoneal cavity immediately after the operation revealed no evidence of hemorrhage, hematoma, or inadvertent organ injury (except for the intraoperative complications).
Discussion
Gastric cancer is the fourth most common type of cancer and the second leading cause of death in the world. 18 Although the incidence of gastric cancer and the mortality associated with this disease have decreased gradually in Japan and Korea, it remains the second most frequent cause of death in Korea. 19 Radical surgery with extensive lymph node dissection was first established as a treatment for gastric cancer in the last century. However, an individualized minimally invasive approach is now the key surgical approach for early-stage gastric cancer. Kitano et al. 20 first described laparoscopy-assisted distal gastrectomy in 1994. Since then, this procedure has become the standard treatment for early gastric cancer in Korea and Japan. Thereafter, the NOTES procedure is reported in gastric resection. Nakajima et al.21,22 reported partial gastric resection and transvaginal extraction by hybrid NOTES in humans after testing it in a porcine model.
There are four potential NOTES routes: namely transgastric, transrectal, transvaginal, and transurethral. Given the large volume of perigastric specimens and the thickness of the endoscope, the transurethral route cannot be used for stomach specimen extraction and endoscopy. Although transrectal extraction is feasible, it carries a high risk of infection and postoperative leakage. In regards to gastric cancer, the transgastric route is not a good route for dissecting perigastric lymph nodes because of the strong retroflexion of the scope and the possibility of cancer seeding. In contrast, there have been no reports of any increased risk of postoperative leakage or infection for the transvaginal route. 23 For this reason, this route was selected for the present study. In this study the insertion of the endoscope via the transvaginal route was laparoscopic assisted, but it is possible for experienced gynecologists to perform a posterior colpotomy in humans by eye. 16 Currently, the use of the transvaginal route is limited to elderly parous women, but when the instruments become smaller and more delicate, it will be possible to use the transurethral route for transurethral endoscopy, while the gastric specimen is removed via the transgastric route. This may be one way to expand hybrid NOTES to male and young female patients in the future.
In hybrid NOTES, transvaginal endoscopy proceeds in the upper direction, and, as with laparoscopy, it involves a 0° scope. This can cause difficulties with respect to exposing and grasping tissue. To overcome this problem, we speculated that the endoscope could be hung from the lower abdomen and appropriately angled by using an endoclosure needle to insert Polysorb 3-0 (Fig. 2b). This way the endoscope is both anchored and can be angled similar to a flexible laparoscopic telescope. Although a flexible laparoscopic telescope still inspects the operation field better than the anchored 0° endoscope, we found the latter revealed a 30°–45° field of view in the right and left directions. This is why it is difficult to expose the roots of the left and right gastro-epiploic arteries without the help of a laparoscopic instrument in one-port NOTES.
The trocar site is important in one-port NOTES. We recommend that the midline be avoided because it is on the same axis as transvaginal endoscopy. We inserted the trocar in the right-mid area because the operator is right-handed. In one-port NOTES (Fig. 1a), because the traction power of the endoscopic instrument is weak, it is essential that the tissue is subjected to additional anchoring by using an endoclosure needle. We found that when the tissue was retracted to the midline in this manner that there was better access by the endoscope and the vessels were more readily exposed (Fig. 3c). Our observations suggest that it is possible to use one-port NOTES to dissect one or two areas of the perigastric basin that are located in the midline area. It is notable that although it is easy to coagulate small vessel branches in pigs, it is difficult to dissect perigastric lymph node by using a coagulator without ultrasonic shears in humans. Hybrid NOTES remains safer than pure NOTES in humans at present, but it is likely that technological developments can overcome the problems associated with pure NOTES within a few years.
It is easy for surgeons with experience in laparoscopic surgery to adapt to hybrid NOTES, as the laparoscope is replaced by an endoscope, and the operation is performed just without an assistor. In contrast, an experienced endoscopist is needed to perform transvaginal endoscopy during NOTES. This procedure has several advantages over SPLS: First, larger specimens can be extracted because the vaginal wall is elastic; second, it is associated with less abdominal wound pain and fewer wound complications. 23 We think the development of the laparoscopic instrument will be thinner (5-mm trocar to 2- or 3-mm trocar) and smaller, along with the abdominal incision. Therefore, natural orifice extraction will be important in the future. Third, this procedure will be a useful translational technique for those having little or no experience with the NOTES procedure. However, it cannot be used in males or in female patients with atrophic vaginitis, vaginal infection, or a vaginal prolapse syndrome; there is also a risk of bowel injury in patients with severe pelvic adhesions.24,25 However, if the transurethral route was used for endoscopy and the transgastric route for specimen removal, hybrid NOTES could be adapted to be suitable for both male and young female patients.
SPLS can be used for a wider range of patients than NOTES, which is limited to elderly female patients. However, it is not easy to perform the first few cases of SPLS because the multijointed instruments are difficult to handle. Laparoscopic operation experience is helpful for performing SPLS but is no substitute for SPLS experience. Santos et al. 26 reported that SPLS is more technically challenging than standard laparoscopic surgery, and they suggested that specialized training curricula should be developed for inexperienced surgeons who wish to perform SPLS. We recommend to first attempt easy operations such as appendectomies or gastric wedge resections. The multijointed instrument is difficult to use by surgeons who are unfamiliar with SPLS; however, curved and reusable instruments (DAPRI single-site direct access, Karl Storz, Tuttlingen) are now available, which should greatly facilitate the implementation of this procedure, even by novices.
We experienced a case of bladder injury during a transvaginal endoscope insertion and a case of gastric perforation during lesser curvature tissue resection in SPLS. The bladder injury was probably caused by the inexperience of the surgeon in swine operation. However, this would not be a problem in human operations, if the transvaginal insertion of the endoscope is performed by an expert gynecologist. On the other hand, the intraoperative gastric perforation could have been caused either by the small amount of connective tissue at the lesser curvature side of the pig or by difficulties encountered in handling the multijoint instrument. Intraoperative gastric perforation is also a possible complication in human operations. The present study has several limitations. First, the number of pigs in each group was only three. Second, the surgeon did not have extensive experience in each procedure. However, the present study is the first experimental trial to compare hybrid NOTES with SPLS procedures worldwide.
In conclusion, two-port NOTES and SPLS are more feasible than one-port NOTES for SN basin dissection in a porcine model. One-port NOTES is difficult to perform and requires long operation times; however, we foresee this operation as becoming more common in the future.
Footnotes
Acknowledgments
The authors would like to thank HyunJhung Jhun, DVM, and all the staff of the Laboratory Animal Research Center, Konkuk University, for conducting experiments. This study was supported by the Gyungsang National University Hospital Clinical Research Fund (GNUH CRF 2010-002). The authors wish to thank Covidien for funding and support with laparoscopic instruments, as well as Olympus for support with the endoscope.
Disclosure Statement
No competing financial interests exist.