
Abstract
Abstract
Purpose:
Exposing the recurrent laryngeal nerve (RLN) during all types of thyroid surgery is essential to protect this nerve. Endoscopic thyroidectomy (ET) has gained acceptance from both patients and physicians, in part due to the cosmetic benefits. Therefore, the avoidance of intraoperative RLN impairment during ET is of critical significance. We have developed a standard approach to expose the RLN during ET that prevents RNL impairment.
Patients and Methods:
ET was performed in 120 consecutive patients with thyroid disease. In order to develop a standard procedure that protects the RLN, several steps that differed from the traditional open procedure were introduced. First, the thyroid gland was freed from the isthmus instead of the superior pole. Then, the inferior pole of the thyroid gland was meticulously freed, and the lateral side of the thyroid gland was freed followed by the superior pole. At this point, the RLN was easily visualized in the tracheoesophageal groove. The thyroidectomy was then performed simultaneously with exposure of the RLN from the inferior to superior aspects. All RLNs were exposed when hemithyroidectomies, subtotal thyroidectomies, or total thyroidectomies were performed. The operative time and parathyroid hormone (PTH) and calcium levels were recorded prospectively and analyzed.
Results:
Using this method, all RLNs were easily exposed within 15 minutes. Only one case of transient RLN palsy occurred due to accidental contact of the harmonic scalpel to the nerve. Postoperative hypocalcemia occurred in 23 cases (19.2%), and the PTH level decreased significantly in 33 cases (27.5%). The PTH levels returned to normal within 3 months.
Conclusion:
Use of the described approach to expose and protect the RLN when performing ET is safe and feasible.
Introduction
Patients and Methods
Clinical data
Between January 2009 and June 2011, a total of 120 patients underwent ET at the Xiangya Hospital of Central South University, Changsha, China. The group consisted of 110 female and 10 male patients 24–74 years of age (mean age, 35.6 years). Twenty-two patients had unilateral multiple nodules, and 98 patients had bilateral lobe nodules as determined by B-type ultrasound. The tumor diameter ranged from 1.2 to 5.5 cm (mean diameter, 3.4 cm). Malignant pathologic changes were suspected in 6 cases based on psammoma bodies noted on B-type ultrasound. The pathology results of intraoperative frozen sections and paraffin sectioning after treatment showed that all samples were papillary carcinomas. All 6 patients were low risk (<2 cm, no definite evidence of local invasion or central nodal metastasis based on preoperative examinations). In addition, the remaining 114 cases were diagnosed as adenomatous nodular goiters or adenomas.
All patients underwent preoperative indirect laryngoscopy. The parathyroid hormone (PTH) and calcium levels of these patients were routinely obtained pre- and postoperatively.
Operative methods
All operations were performed by the same team. ET was performed using an anterior/breast approach. The procedure was performed with the patient under general anesthesia and endotracheal intubation. The patient was placed in the supine position with the neck extended. A 1-cm longitudinal incision was made at one-third of the distance from right to left nipples. The other two 5-mm incisions were made at the superomedial edge of the breast areolae (Fig. 1). Epinephrine (1:500,000) diluted in 0.9% NaCl solution was injected into the working area under the platysma in the neck and subcutaneously in the anterior chest. One 10-mm trocar and two 5-mm trocars were then punctured into the subcutaneous space, respectively. A 10-mm 30° laparoscope was then introduced into this space through the 10-mm trocar (Fig. 2). The flap extended by ultrasound scalpel from the thyroid cartilage superiorly to 4 cm below the suprasternal fossa inferiorly and laterally from just beyond the medial border of the sternocleidomastoid muscle under euthyphoria. The working space was maintained using low-pressure CO2 insufflation at 5–6 mm Hg. The midline of the strap muscles was identified and separated.
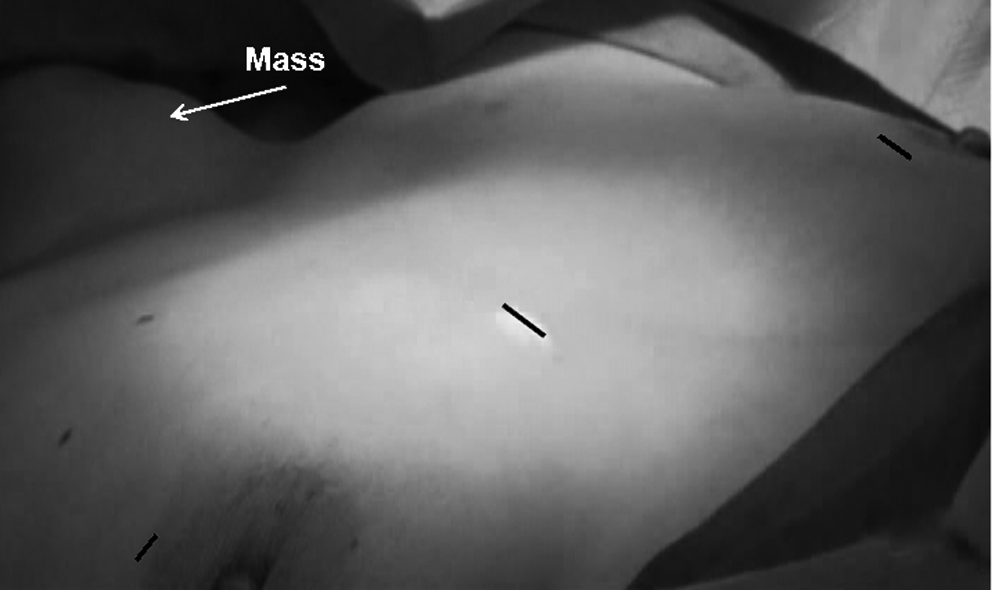
Location of the incisions.

View from the operation external field, showing the instruments in place.
Dissection of the thyroid was initiated by dividing the isthmus from the trachea using a harmonic scalpel. At this point, the front one-third of the tracheal rings was exposed (Fig. 3). This step facilitated the dissection of the gland laterally and posteriorly and allowed for optimal visualization of the superior thyroid pedicle and the RLN.
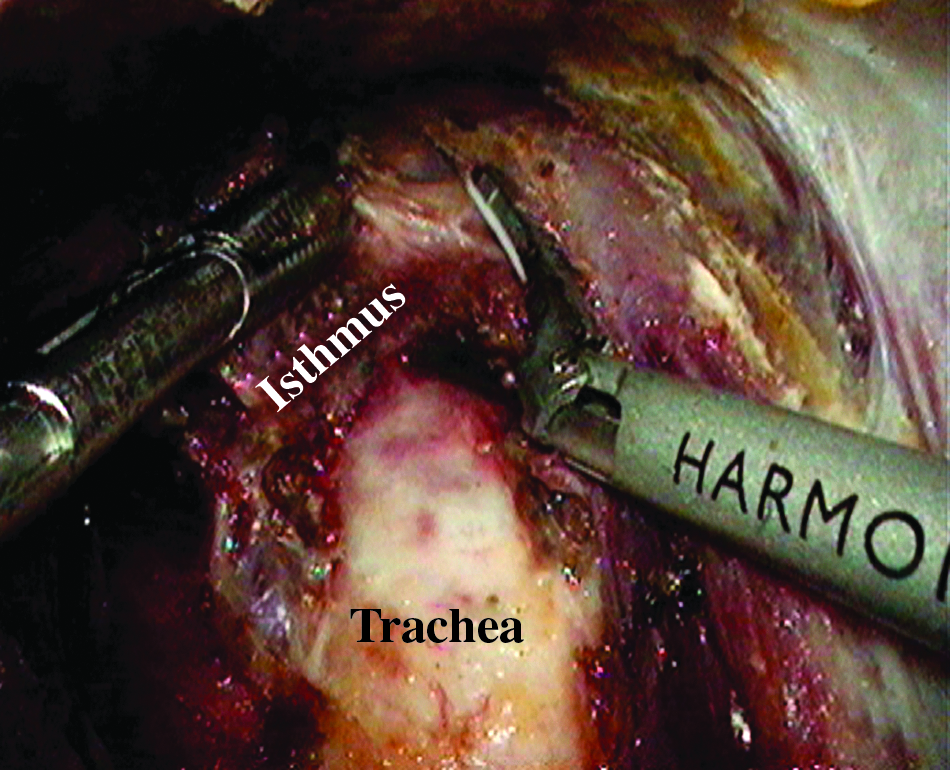
Dissection of the isthmus from the trachea.
Then, the inferior pole of the thyroid was carefully and meticulously dissected, which mainly included the inferior thyroid vein, by ultrasound scalpel hemostasis (Fig. 4). The dissection was carried out as close as possible to the surface of the thyroid gland. The main trunk of the inferior vessels was protected to avoid compromising the blood supply to the parathyroid glands. Considering the variants of the RLN, no core-like structure should be extirpated unless the RLN is definitely excluded. When the inferior pole of the thyroid gland was freed, the thyroid gland was extracted to the middle-superior aspect using an assistant clamp.
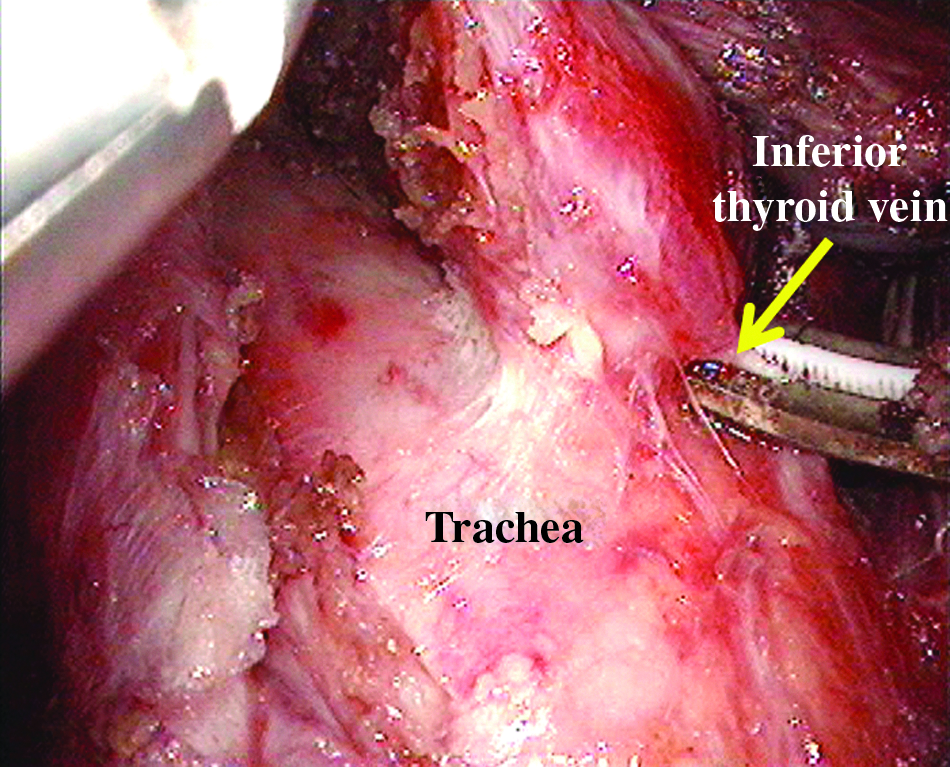
Dissection of the inferior vein by ultrasound scalpel hemostasis.
The RLN was exposed as follows. The lobe of the thyroid gland was retracted to the inner and upper aspects. A plane was developed between the thyroid lamina propria and the surgical capsule, and the peripheral tissues adhering to the gland were divided using a separation bar (Fig. 5). If the middle thyroid vein was clearly exposed, it was dissected from the gland; otherwise it was dissected later. At this time, the gland could be tipped freely, and the inferior thyroid artery was easily exposed. The gland was then retracted to the inner superior aspect, and the formative region between the tracheoesophageal groove and the inferior thyroid artery was separated using curved forceps and suction (Fig. 6). There are always small accompanying vessels in this area. Fortunately, if bleeding occurs it can be controlled by compression. Use of the ultrasonic scalpel to achieve homeostasis blindly was unnecessary and forbidden. With the magnifying effect of the laparoscope and the excellent hemostatic effect, the operative field was always clear, and the RLN was generally quite bright, which made it easier to discriminate from blood vessels. The RLN can be partially exposed (Figs. 6 and 7) at this time. The branch of the inferior thyroid artery adhering to the gland was dissected close to the gland, and the inferior pole was totally freed under euthyphoria. There was no urgency to track and expose the nerves. The entire gland was pulled downward, and the Berry's ligament and upper pole of the thyroid gland including the corresponding blood vessel were revealed and dissected (Fig. 8). As the gland near the RLN entering larynx was not separated, this procedure needed multiple combinations of front and back movements of the upper pole. Eventually, curved forceps were able to separate the nerve to the point where it entered the larynx near the inferior horn of thyroid cartilage. The cervical segment of the RLN was then exposed completely (Fig. 9).
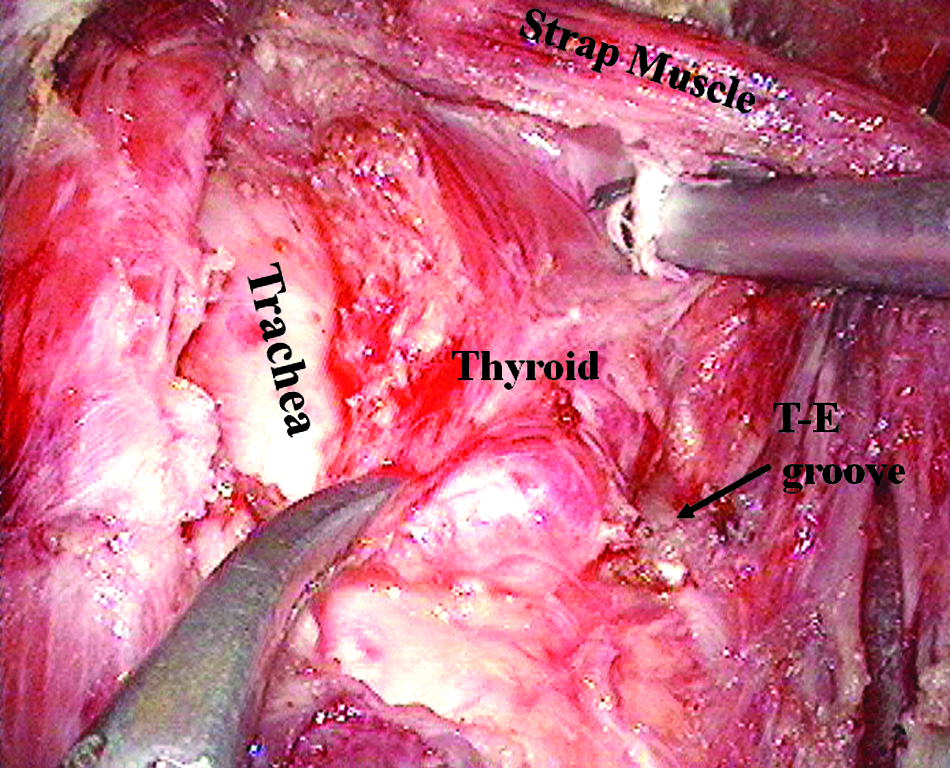
Extracapsule anatomical technology. The separation bar was applied to separate the thyroid gland and surgical capsule, pulling the peripheral tissue to the posterior lateral side to avoid the nerves involved moving up. T-E, tracheoesophageal.
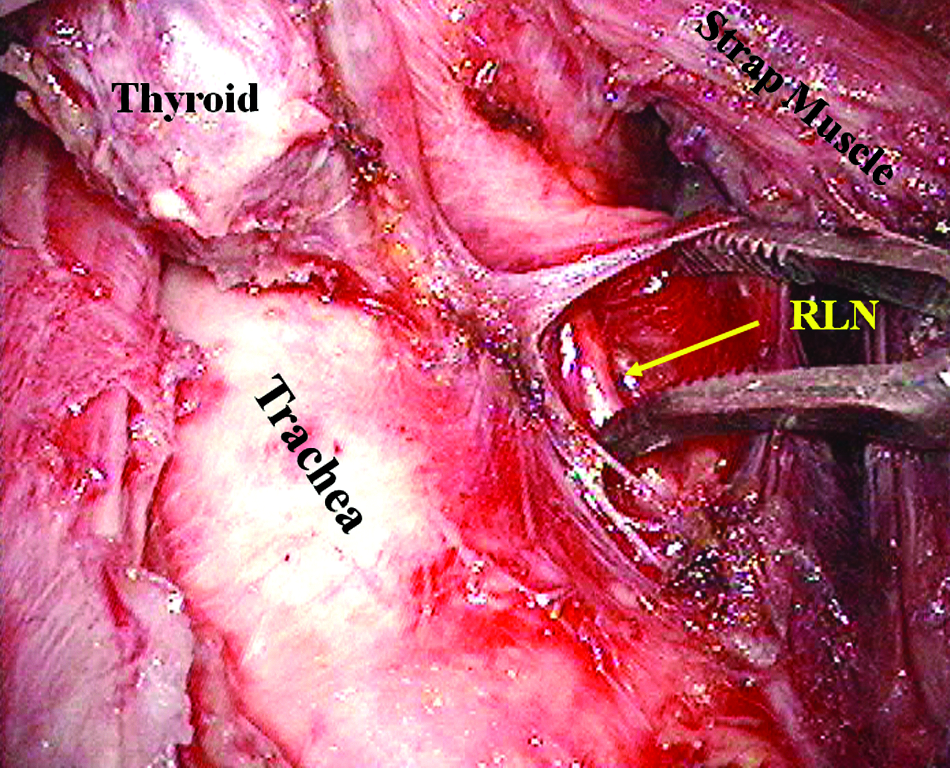
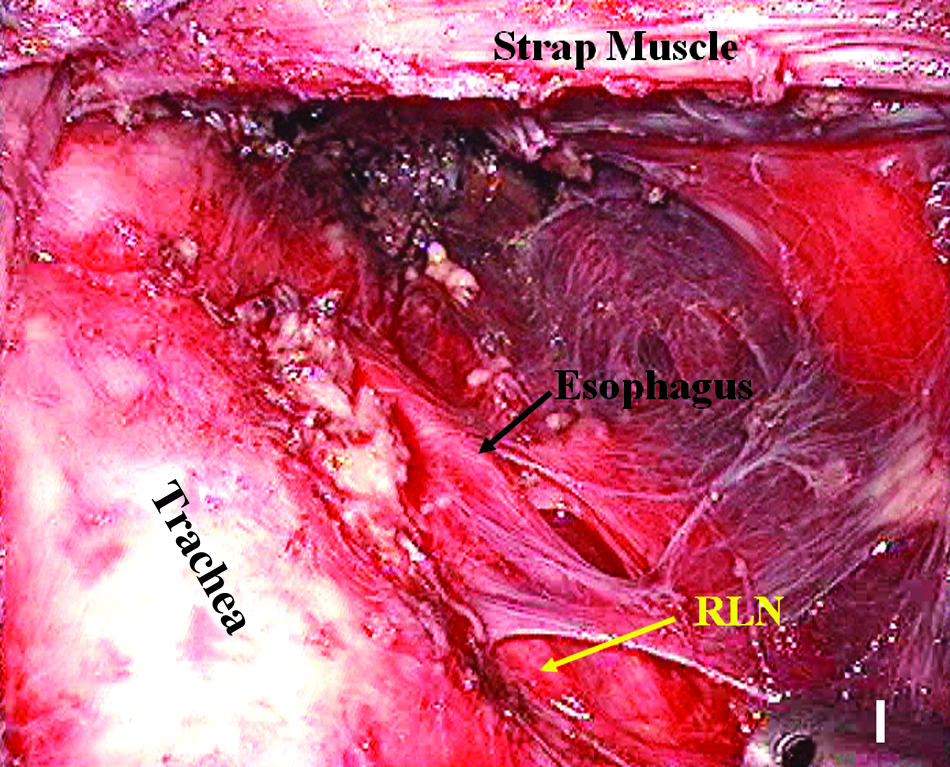
The recurrent laryngeal nerve (RLN) was exposed in the tracheoesophageal groove. Use caution not to damage the esophagus.
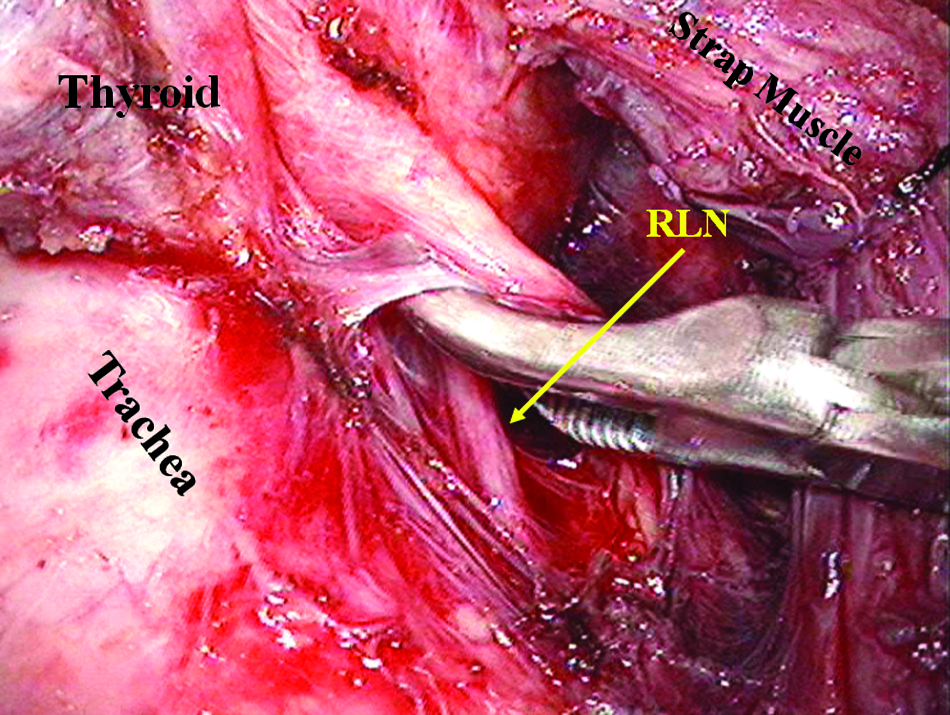
Exposing the nerve to the position where it enters the larynx.
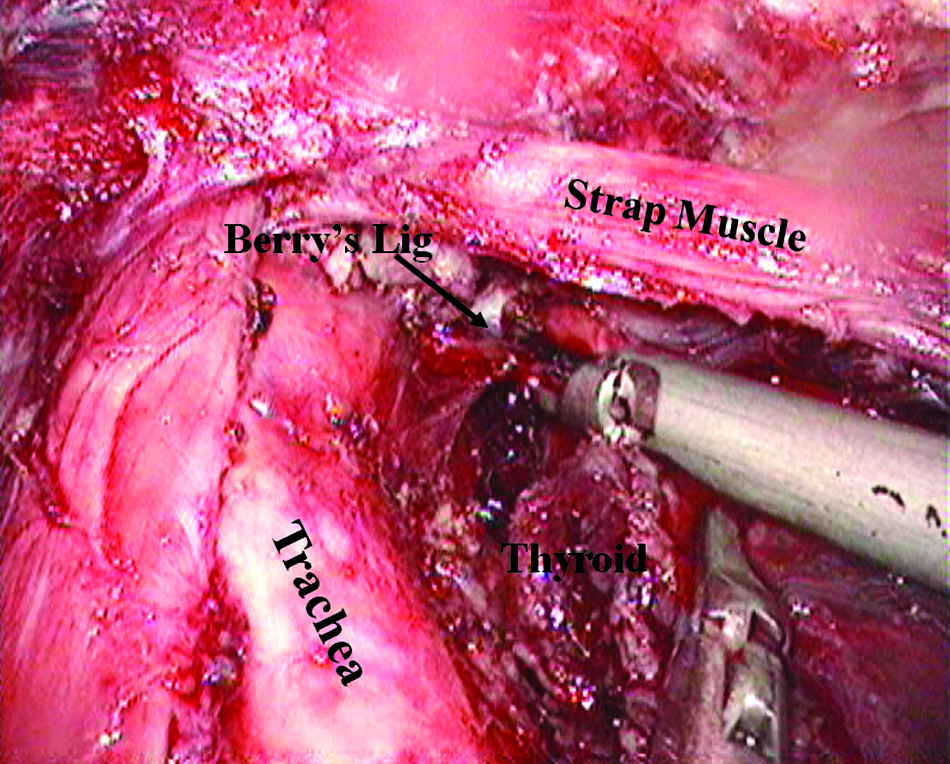
Mobilizing the upper pole and cutting off Berry's ligaments (Lig).
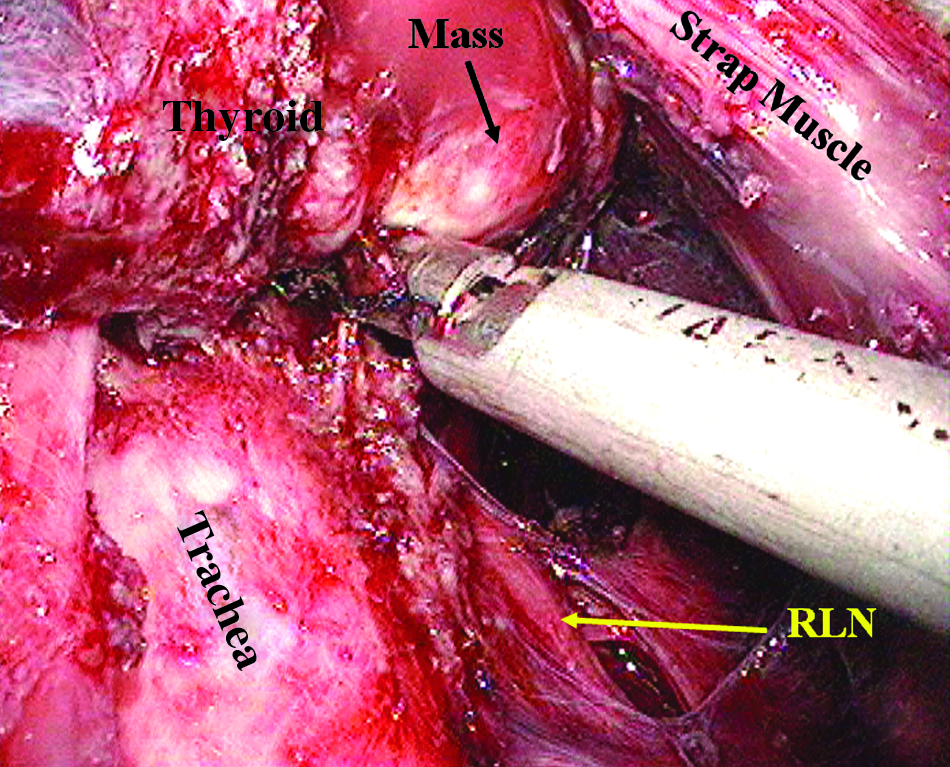
The gland was dissected at the position where the RLN enters the larynx, and attention was paid to the correct application of the ultrasound scalpel.
The specimen was placed into a specimen bag and pulled out of the middle pore for frozen sectioning. Distilled water was applied to flush and soak the wound surface, and ribbon-gauze was used to wipe the surface dry. The entire length of the RLN was then confirmed to be intact (Fig. 10). The strap muscles were sutured, and a drainage tube was placed through the right operative pore into the operation field. The incision was closed.
View of the operative field after resection of the left gland lobe.
The resection range was based on the character of the lesion being the same as for the open operation. With regard to unilateral nodules, whether single or multiple, a unilateral lobectomy resection plus isthmectomy was performed (16 cases), whereas the Hartley Dunhill operation was performed in those with bilateral nodules (98 cases). A prophylactic/elective central compartment dissection was performed under endoscopy in the remaining 6 patients who had proven papillary carcinoma (cN0) by frozen sectioning.
Results
All 120 cases underwent ET successfully without conversion. The mean operative time was 72 minutes, and the mean blood loss was approximately 20 mL. Of these 120 cases, 114 (95%) were diagnosed as nodular goiters, 7 of whom had Hashimoto's thyroiditis. Six had papillary carcinomas, and 1 had central compartment lymph node metastasis.
One hundred twenty-eight RLNs were exposed (8 patients underwent bilateral explorations). The rate of complications was similar to that reported in open surgical methods. 4 Transient RLN palsy occurred in 1 of the 128 patients (0.8%). Postoperative hypocalcemia (serum level <2 mmol/L) occurred in 23 of the 120 cases (19.2%). Serum PTH level decreased significantly compared with the preoperative level in 33 of the 120 patients (27.5%); only 2 patients had serum PTH levels below the low normal range (15 pg/mL) (data not shown). Twelve patients complained of numbness of the fingers or toes. An intravenous bolus of calcium gluconate (2 g of calcium) was given to those patients for 2 days followed by oral calcium lactate for 1–2 weeks. No permanent RLN palsy, hypocalcemia, or hypoparathyroidism was noted during a minimum of 3 months of follow-up. There was 1 case of chylous leakage encountered in the cancer group, which spontaneously resolved within 2 weeks. The drainage tubes was removed after 24–48 hours except for the patient with chylous leakage. The mean postoperative hospital stay was 2.3 days. Four patients had red swelling in the skin flap in the frontal area of the chest 1 week after discharge from hospital. These symptoms disappeared following the application of antibiotic for 2 days. Twenty-four patients complained of cutaneous hyperalgesia in the anterior region of the neck, which normalized after 1–2 months.
Discussion
ET provides a satisfactory cosmetic solution in patients with thyroid nodules who have concerns about visible scarring in the front of the neck. 5 A scar is unacceptable after surgery, let alone a change in voice. Thus, RLN palsy in patients almost always results in medicolegal litigation.3,4,6,7 To prevent RLN injury, routine identification of the RLN is now included in the treatment recommendations and is regarded as the standard of care in patients undergoing open thyroid surgery. Because of the different visual angle and manipulation methods used in ET, detection and exposure of the RLN are technically different from those in open thyroidectomy. Herein, we describe an easy and practical way to achieve this critical step via an anterior chest approach. Using this method, 128 RLNs were exposed during ET without complications, such as permanent nerve palsy and hypoparathyroidism.
During this procedure several key points are emphasized:
1. Mobilization of the thyroid gland was initiated from the isthmus, which is the safest portion of the gland. The isthmic portion and the pyramidal lobe should be mobilized together, whereas the ipsilateral side is separated from the lateral side as far as possible (Fig. 3). Sufficient mobilization of the isthmic portion was beneficial for tipping the lobe, while mobilizing the lateral portion to expose the RLN and enhancing the visual angle when identifying the RLN. 2. Freeing the thyroid requires staying close to the gland. This can protect the blood supply of the parathyroid gland as well as decrease the thermal damage to the RLN. Caution is necessary to avoid damage to any fiber-like structures before the RLN is visualized. 3. After the inferior portion of RLN was exposed in the tracheoesophageal groove, freeing the upper pole of the lobe subsequently was suggested. Do not try to trace the entire portion of the nerve before the lobe is sufficiently freed. Otherwise, in cases with bleeding, achieving hemostasis can be a challenge due to the narrow operation field and bad visualization, which increased the risk of damaging peripheral structures as the esophagus or RLN. Sufficient mobilization of the gland is a prerequisite for exposure of the RLN in ET. Only after the ipsilateral lobe was totally freed was the inferior part pulled to the internal upper side using the assistant clamp. The nerve was then easily traced to the end point upon entering the larynx by dissection of the lateral side synchronously. As mentioned previously, dissection of any vessels is required close to the gland to avoid affecting the blood supply of the parathyroid glands and inducing low calcium hyperspasmia postoperatively. 4. During the entire procedure, attention must be paid to avoid heat damage to the RLN caused by the ultrasonic scalpel. The RLN is quite fragile at high temperature. Although the ultrasonic scalpel has a good reputation for generating lower heat than an electric scalpel, it can also cause demyelination of the nerve. The functional side of the ultrasonic scalpel should be used with caution and as far away from the nerve as possible. It was previously reported that the safety distance between ultrasound scalpel and nerve is 5 mm; moreover, the active scalpel should not contact the nerve. Owaki et al.
8
suggested that a distance of >3 mm from the knife and working continuously for 20 seconds at a grade of 3 is quite safe. Our experience has indicated that using an ultrasound scalpel at a grade of 3 for <5 seconds when close to the RLN is safe. Furthermore, we suggest that the head of the scalpel should be cleaned to reduce the temperature between each application (Fig. 9).
In conclusion, our experience showed that under the premise of sufficient mobilization of the gland, synchronized exposure of the RLN is quite safe during ET.
Footnotes
Disclosure Statement
No competing financial interests exist.